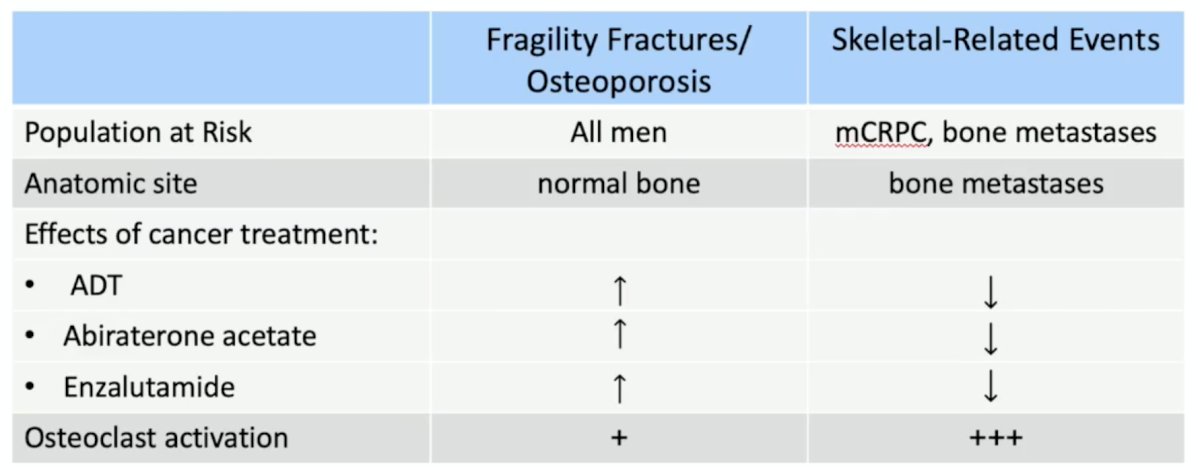
(UroToday.com) The 2026 Advanced Prostate Cancer Consensus Conference (APCCC) meeting featured a management and prevention of frequent side effects and modifying the metabolism session, and a presentation by Dr. Matthew Smith discussing bone protection in patients with hormone-sensitive prostate cancer starting on long-term ADT and in patients with mCRPC. There are important differences when considering skeletal-related events versus fragility fractures and osteoporosis. All men are at risk of fragility fractures and osteoporosis, whereas skeletal-related events are specific to patients with bone metastatic CRPC:
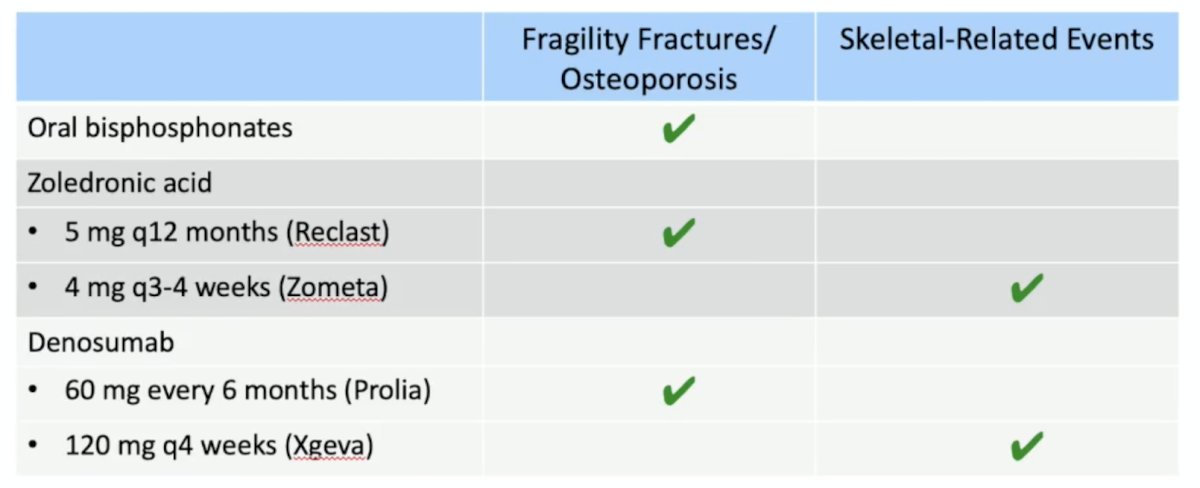
FDA-approved uses of osteoclast-targeted therapy include oral bisphosphonates, zoledronic acid, and denosumab:
When assessing men for fracture risk, it is important to consider age, prior fracture history, and low bone mineral density, which are the strongest predictors of fracture risk. Most fragility fractures occur in individuals with a normal bone mineral density, thus bone mineral density alone is insufficient to evaluate fracture risk. Dr. Smith notes that the National Osteoporosis Foundation has Fracture Prevention Guidelines for Men, and that there should be consideration of FDA-approved medical therapies based on the following:
- A vertebral or hip fracture
- Femoral neck or spine T-score <= -2.5
- FRAX 10-year probability of a hip fracture > 3% or 10-year probability of any major fracture > 20%
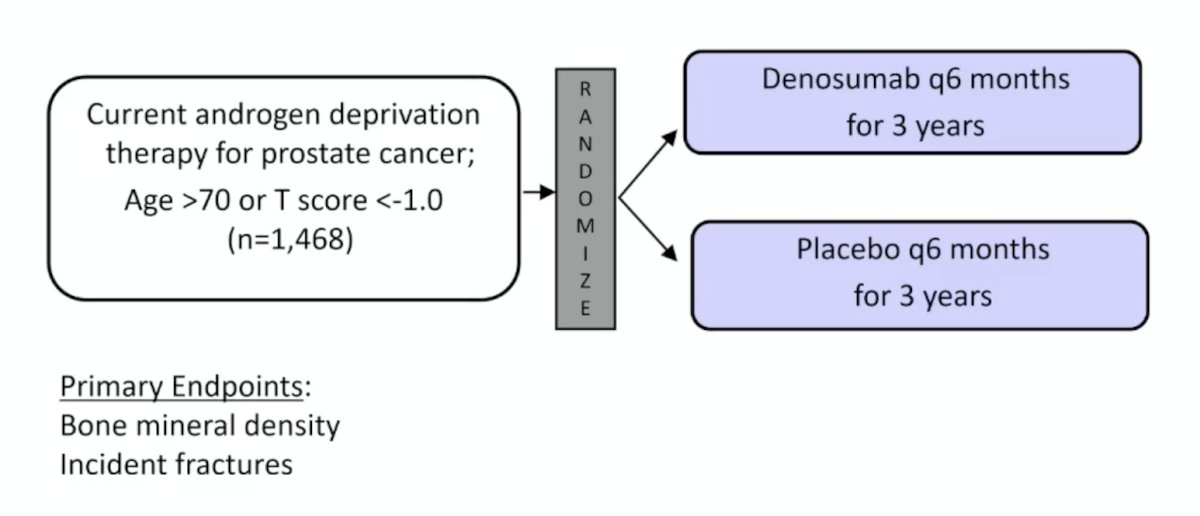
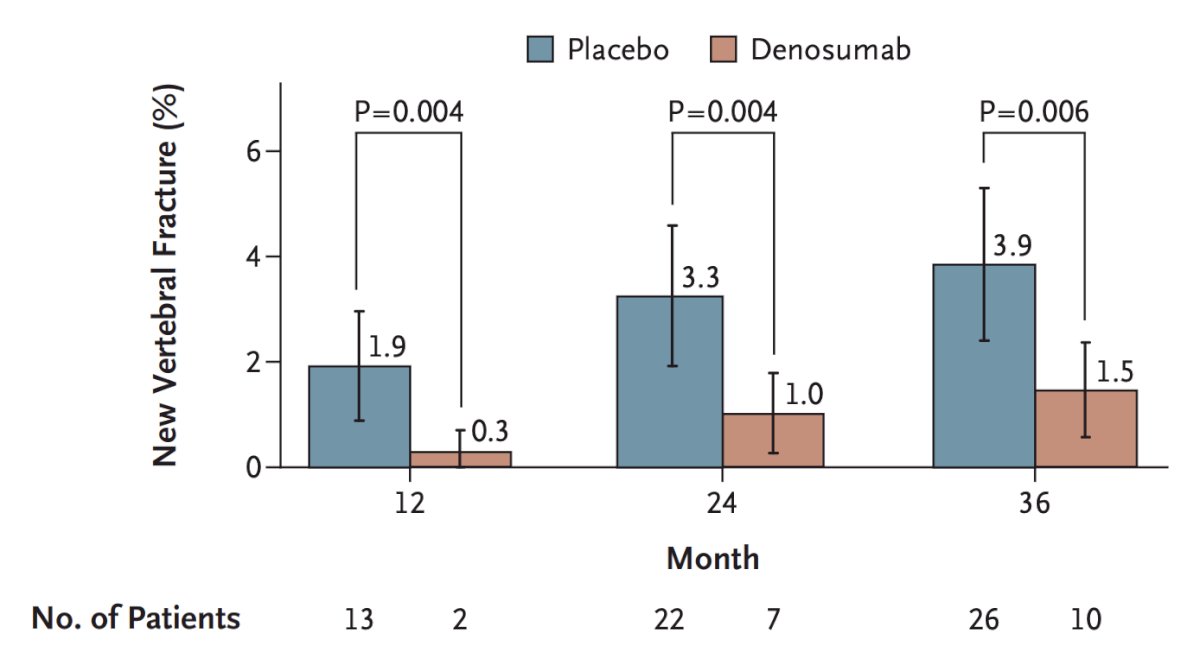
Published in 2009, the denosumab fracture prevention study1 enrolled 1,468 men on androgen deprivation for prostate cancer and randomized them to denosumab every 6 months for 3 years versus placebo every 6 months for 3 years:
Denosumab was found to increase bone mineral density at all skeletal sites: lumbar spine, total hip, femoral neck, and distal third of the radius:
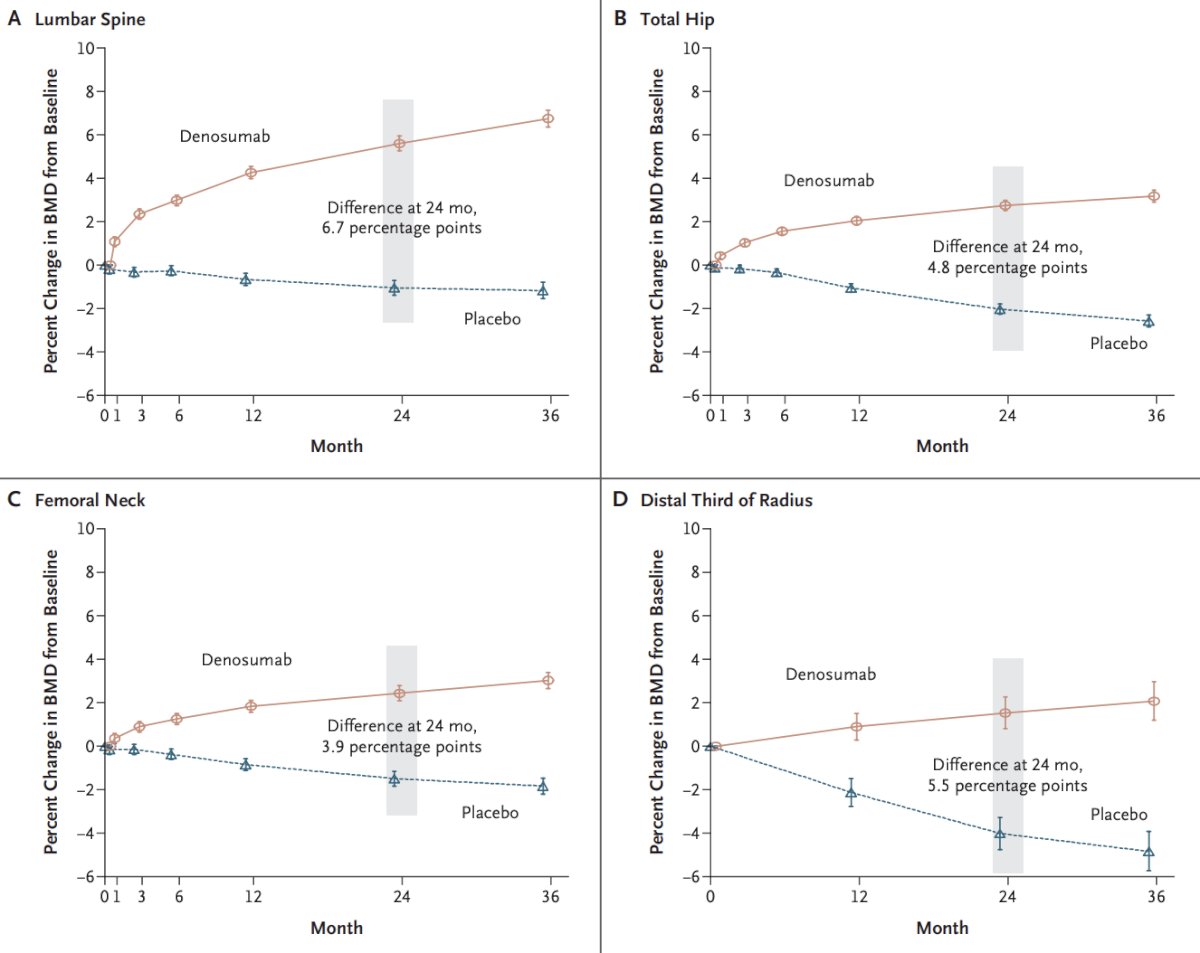
Additionally, patients who received denosumab had a decreased incidence of new vertebral fractures at 36 months (1.5% versus 3.9% with placebo) (relative risk, 0.38; 95% CI 0.19 to 0.78; p = 0.006):
Dr. Smith provided the following conclusions regarding the prevention of osteoporotic fractures:
- For all men receiving ADT:
- Assess fracture risk with the FRAX tool
- Adequate dietary calcium intake, supplemental vitamin D
- Weight-bearing exercise, fall prevention, and smoking cessation
- For most men receiving long-term ADT: perform a DEXA scan to better characterize fracture risk
- Men with prior fracture, osteoporosis, or fracture risk above the National Osteoporosis Foundation thresholds: FDA-approved therapy to prevent fractures
- For men discontinuing denosumab: Consider initiation of bisphosphonate to prevent rebound
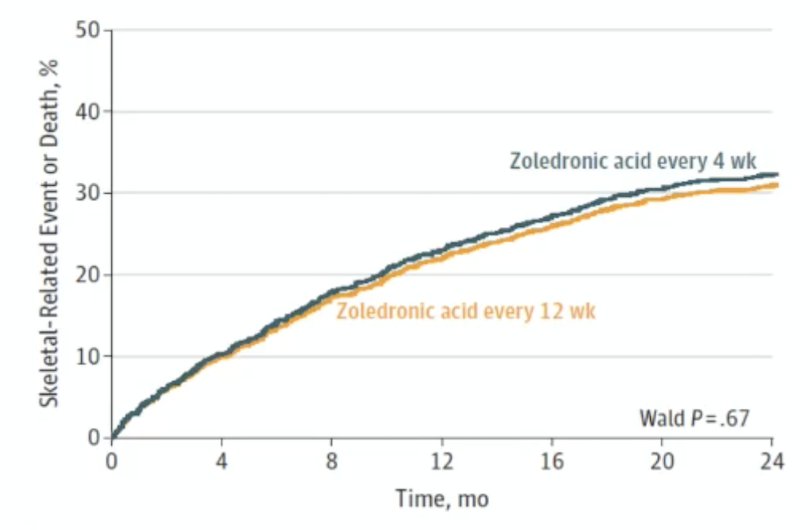
How long should the intervals between treatment with zoledronic acid be for men with bone metastatic cancer? The CALGB 70604 trial randomized 1,822 patients with metastatic breast cancer, prostate cancer, or multiple myeloma to either 4 weeks (n = 911) of zoledronic acid versus every 12 weeks (n = 911) for two years.2 There were 29.5% of patients in the 4-week group that had a symptomatic skeletal event and 28.6% in the 12-week group (p = 0.67), suggesting that a longer interval of treatment may be an acceptable treatment option:
Dr. Smith noted the following limitations associated with the CALGB 70604 trial:
- There can be no assumption of constancy, a requirement for valid inference for non-inferiority studies
- There have been substantial changes in standards of care, event rate, and survival
- Included some patients (men with HSPC) with no potential for benefit
- Skeletal-related event definitions differed from prior studies
- The primary analysis was a 24-month event rate, but only 43% completed the study at 2 years (median follow-up was only 14 months)
- Non-inferiority margin included a clinically important difference
- The longer dosing interval did not improve safety/tolerability
Regarding mHSPC, there have been two studies that reported that early zoledronic acid does not improve clinical outcomes for these patients: CALGB/ALLIANCE 902023 (assessing skeletal-related event-free survival) and STAMPEDE4 (assessing failure-free survival):
![Regarding mHSPC, there have been two studies that reported that early zoledronic acid does not improve clinical outcomes for these patients: CALGB/ALLIANCE 90202 [3] (assessing skeletal-related event-free survival) and STAMPEDE4 (assessing failure-free survival):](/images/com-doc-importer/262-apccc-2026/apccc-2026-bone-protection-in-patients-with-hspc-starting-on-long-term-adt-and-in-patients-with-mcrpc/image-6.jpg)
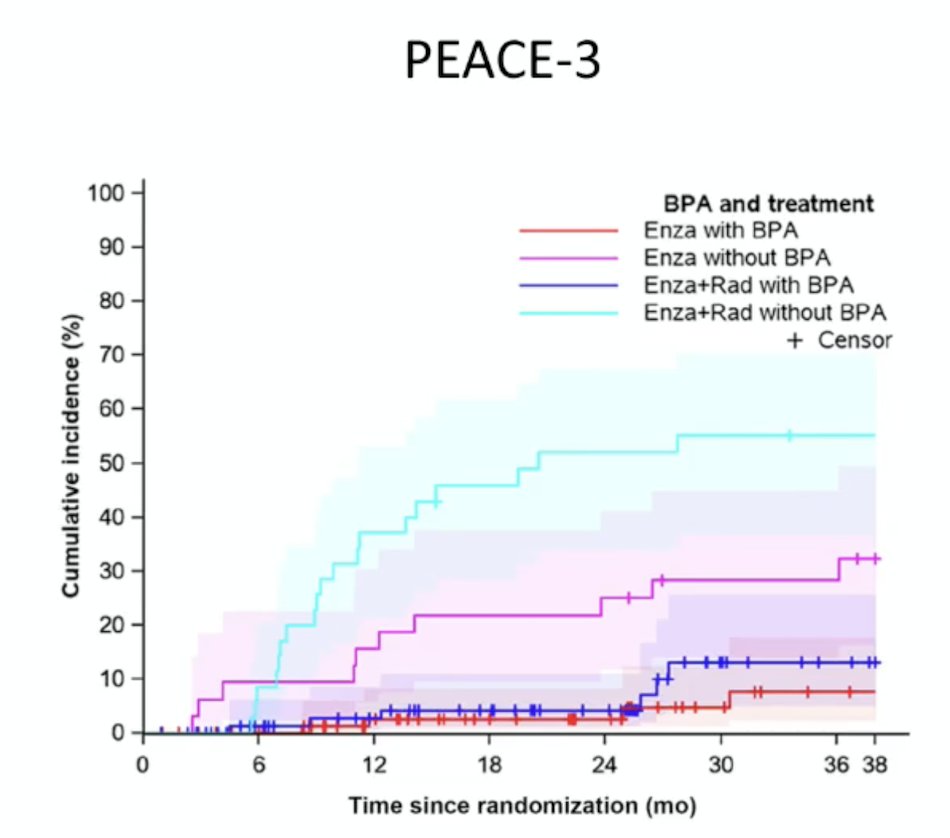
Finally, based on the ERA-223 trial, men enrolled in the PEACE-3 trial5 evaluating radium-223 + enzalutamide versus enzalutamide alone were eventually mandated to receive a bone protective agent to decrease the risk of fractures:
Dr. Smith concluded his presentation discussing bone protection in patients with hormone-sensitive prostate cancer starting on long-term ADT and in patients with mCRPC with the following take-home points:
- For men with mHSPC and bone metastases: denosumab or zoledronic acid in the dose/schedule approved for osteoporosis
- For most men with mCRPC and bone metastases:
- Denosumab or zoledronic acid at the dose/schedule for skeletal-related event prevention
- Optimal schedule of osteoclast-targeted therapy is undefined
- For men initiating radium-223: denosumab or zoledronic acid at dose/schedule for skeletal-related event prevention
- For men discontinuing denosumab: consider zoledronic acid to prevent rebound
Presented by: Matthew Smith, MD, PhD, Massachusetts General Hospital Cancer Center, Boston, MA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 Advanced Prostate Cancer Consensus Conference (APCCC), Lugano, Switzerland, Thurs, April 30 – Sat, May 2, 2026.
References:- Smith MR, Egerdie B, Hernandez Toriz N, et al. Denosumab in men receiving androgen-deprivation therapy for prostate cancer. N Engl J Med. 2009 Aug 20;361(8):745-755.
- Himelstein AL, Foster JC, Khatcheressian JL, et al. Effect of longer-interval vs standard dosing of zoledronic acid on skeletal events in patients with bone metastases: A randomized clinical trial. JAMA 2017;317(1):48-58.
- Smith MR, Halabi S, Ryan CJ, et al. Randomized controlled trial of early zoledronic acid in men with castration-sensitive prostate cancer and bone metastases: Results of CALGB 90202 (Alliance). J Clin Oncol 2014;32(11):1143-1150.
- James ND, Sydes MR, Clarke NW, et al. Addition of docetaxel, zoledronic acid, or both to first-line long-term hormone therapy in prostate cancer (STAMPEDE): Survival results from an adaptive, multi-arm, multi-stage, platform randomized controlled trial. Lancet. 2016 Mar 19;387(10024):1163-1177.
- Tombal B, Choudhury A, Saad F, et al. Enzalutamide plus radium-223 in metastatic castration-resistant prostate cancer: results of the EORTC 1333/PEACE-3 trial. Ann Oncol. 2025 Sep;36(9):1058-1067.