(UroToday.com) The 2026 Advanced Prostate Cancer Consensus Conference (APCCC) meeting featured a management and prevention of frequent side effects and modifying the metabolism session, and a presentation by Dr. Fred Saad discussing what to expect from androgen receptor antagonist monotherapy in terms of side effects and health-related quality of life.
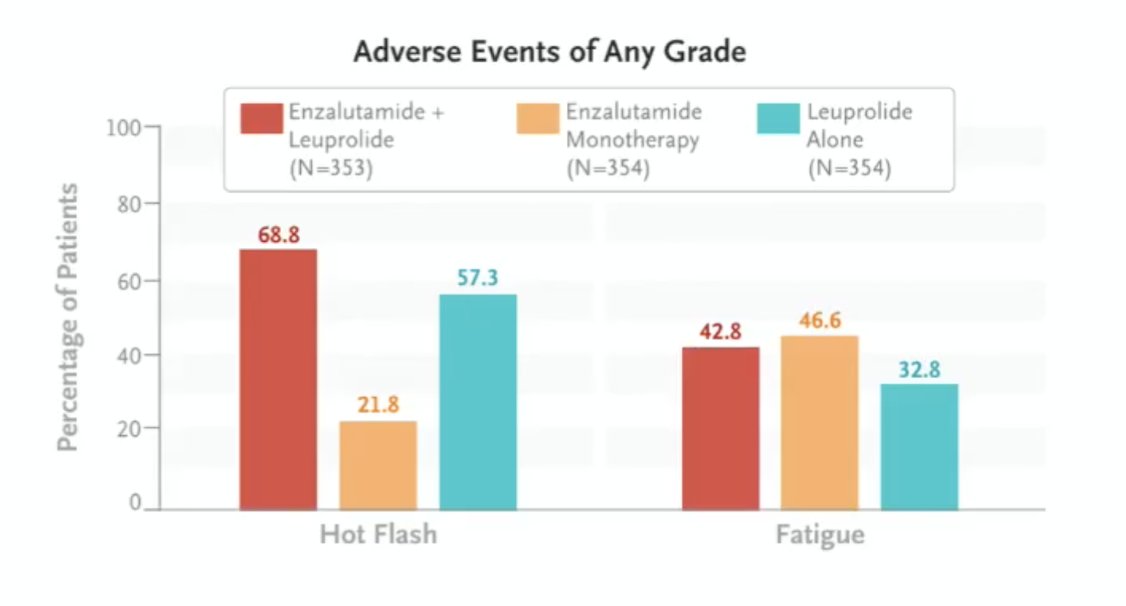
Dr. Saad started his presentation by asking: Should androgen receptor pathway inhibitor monotherapy even be considered? In the EMBARK trial,1 enzalutamide monotherapy versus leuprolide had no difference in overall survival (p = 0.23), but did improve metastasis-free survival (p = 0.017) and symptomatic progression-free survival (p = 0.0001). When assessing adverse events of any grade in EMBARK,2 enzalutamide monotherapy had the lowest incidence of hot flash (21.8%), but had no impact on improving fatigue (46.6%):
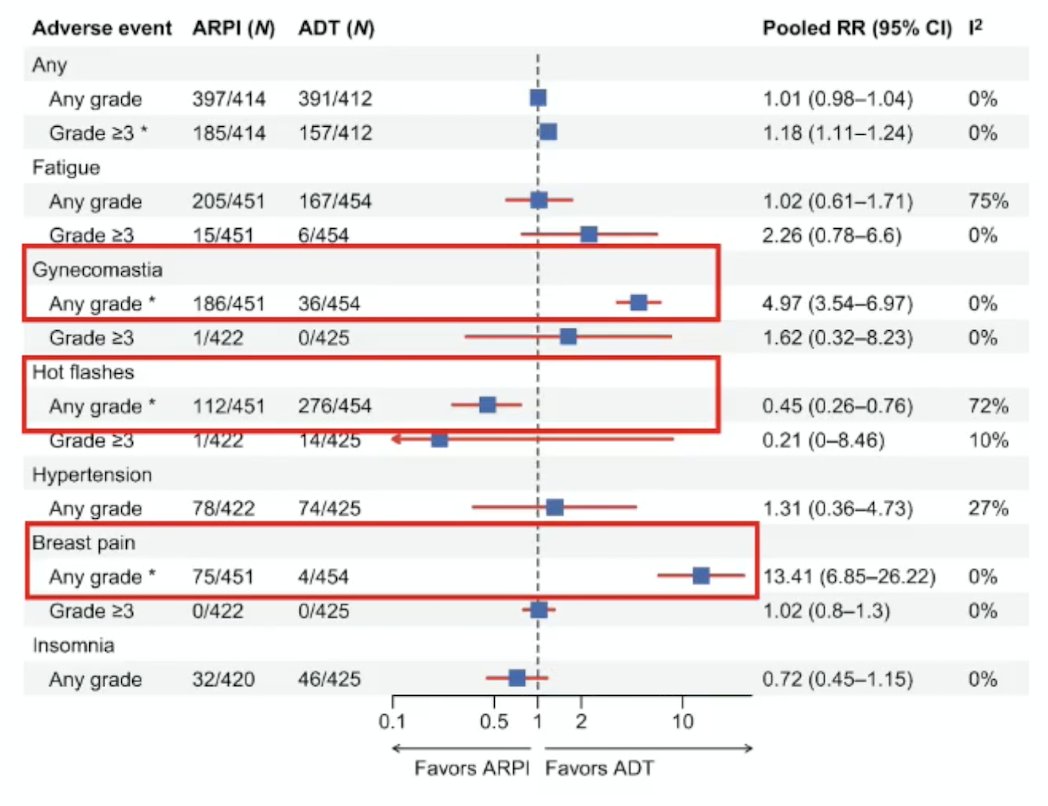
In a recent systematic review assessing androgen receptor pathway inhibitor monotherapy in prostate cancer, Fazekas et al.3 noted that compared with ADT alone, monotherapy may provide similar or slightly improved disease control in selected populations (ie, biochemical recurrence), but with no consistent overall survival advantage versus ADT. In mHSPC and mCRPC, combination therapy is the standard of care, and monotherapy is suboptimal. Additionally, there are quality-of-life trade-offs:
• Better sexual function and fewer hypogonadal symptoms versus ADT
• Higher gynecomastia and breast pain
• Slightly higher grade ≥3 adverse events than ADT alone
Another advantage of androgen receptor antagonist monotherapy is bone health, with maintenance of total-body bone mineral density. This is compared to well-documented significant bone loss with ADT +/- androgen receptor pathway inhibitor.
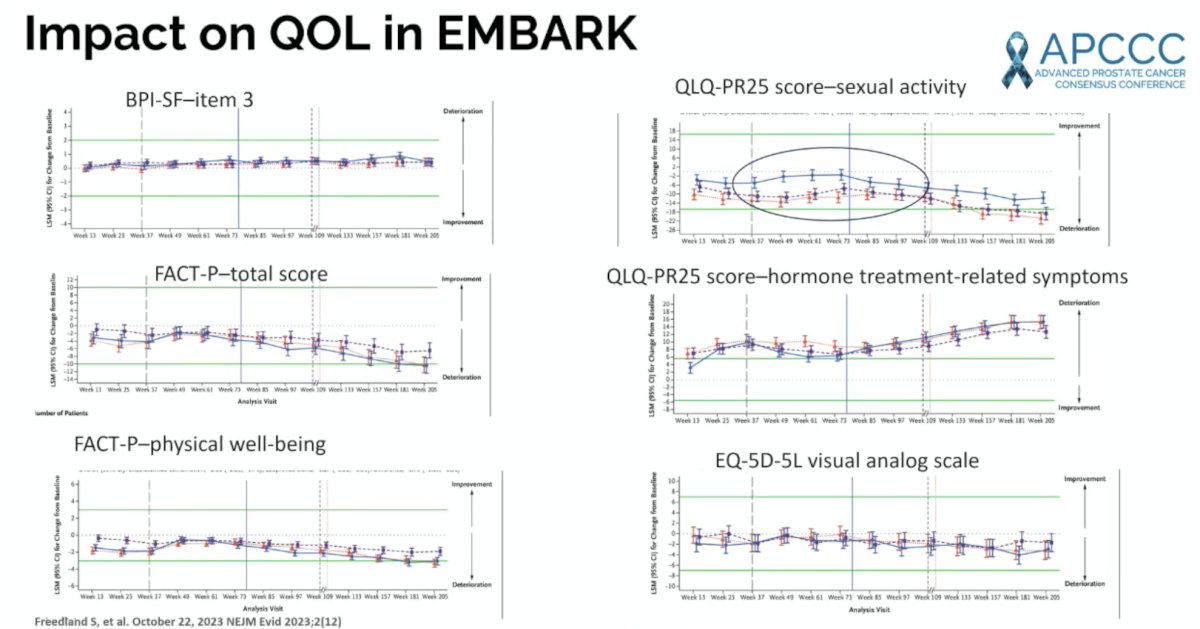
Dr. Saad notes that EMBARK quality of life outcomes generally favor enzalutamide monotherapy, particularly for the QLQ-PR25 score for the sexual activity domain:
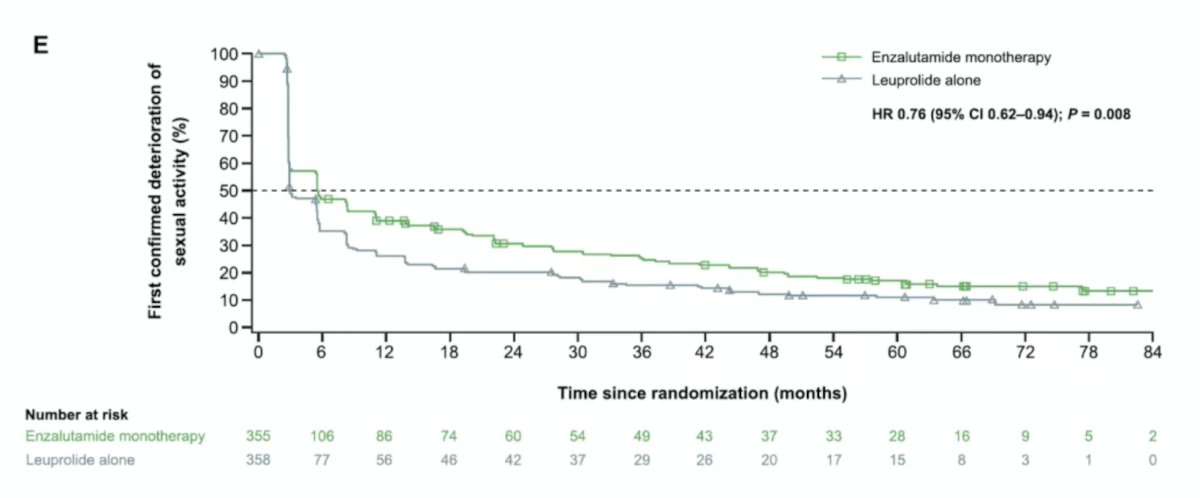
In a report on secondary outcomes of EMBARK for enzalutamide monotherapy,4 Shore et al. noted that the patient-reported outcome of time to deterioration in sexual function was significantly improved for enzalutamide monotherapy versus leuprolide (HR 0.76, 95% CI 0.62-0.94):
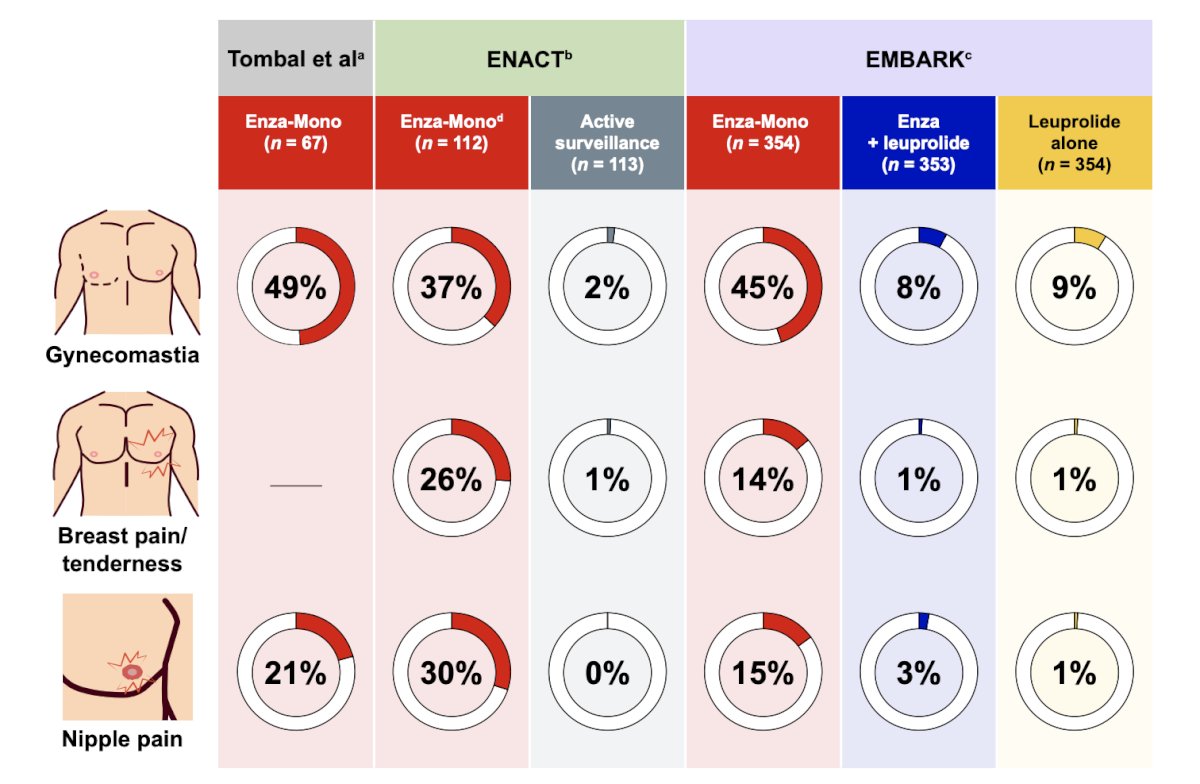
Dr. Saad cautioned that there are breast issues with androgen receptor pathway inhibitor monotherapy. In a recent publication addressing breast-related adverse events in patients with high-risk biochemically recurrent prostate cancer receiving enzalutamide monotherapy, Shore et al.5 highlighted that enzalutamide monotherapy was commonly associated with gynecomastia (37-49%), breast pain or tenderness (14-26%), and/or nipple pain (15-30%):
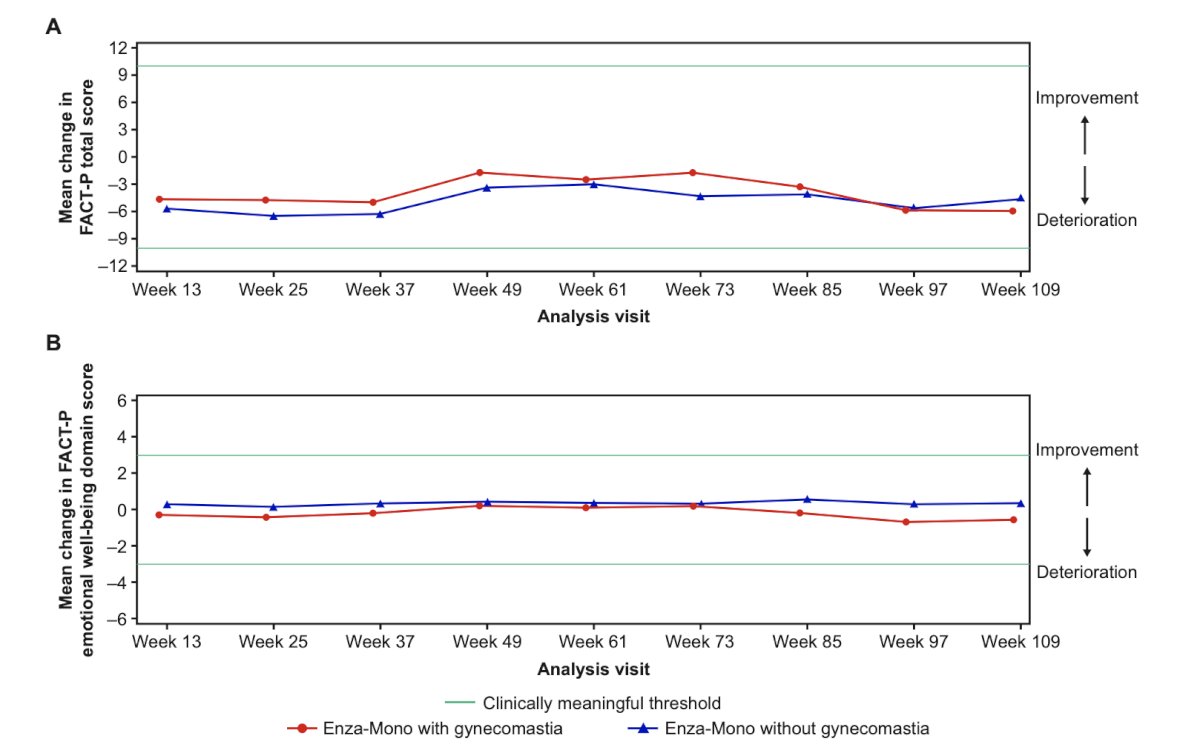
However, gynecomastia did not affect the health-related quality of life (FACTP total score) or psychological well-being (FACT-P emotional well-being score) of patients who received enzalutamide monotherapy in EMBARK. Specifically, over the first 2 years of study in the subgroup with ongoing treatment suspension (from week 37 up to and including week 109), there was no clinically meaningful deterioration in mean FACT-P total score (defined as a >=10 point decrease) or emotional well-being score (defined as a >=3 point decrease) in patients who did or did not experience gynecomastia:
Fatigue is common among advanced prostate cancer patients, and Dr. Saad provided the following management strategies for managing fatigue:
- Physical Activity: Regular, moderate exercise, which is one of the most effective ways to manage cancer-related fatigue
- Energy Conservation: Pacing activities, breaking tasks into smaller steps, and using tools to assist with daily tasks
- Lifestyle Adjustments: Regular naps, a healthy, nutritious diet, and staying hydrated (1.5–2 liters of water daily) are recommended
- Clinician Consultation: Check for underlying causes such as anemia
- Switching Medication: If bothersome, consider lowering the dose or switching androgen receptor pathway inhibitors
Gynecomastia is an adverse effect of androgen receptor pathway inhibitor monotherapy in 30-50% of cases. Prevention is the most effective strategy, which can be done with (i) prophylactic breast irradiation (8–12 Gy single fraction), which reduces the incidence and severity of gynecomastia (well-established, low toxicity); or (ii) tamoxifen prophylaxis with low-dose tamoxifen, which is highly effective and often more effective than radiation. Treatment of established symptoms includes:
- Tamoxifen: most effective for pain relief and size reduction
- Radiotherapy: less effective once gynecomastia is established, but may help with pain
- Surgical removal is most effective if bothersome
Dr. Saad’s clinical approach is to discuss these side effects with the patient upfront, consider prophylaxis in men prioritizing quality of life, and to treat early if symptomatic.
Dr. Saad concluded his presentation discussing what to expect from androgen receptor antagonist monotherapy in terms of side effects and health-related quality of life with the following take-home points:
- Androgen receptor pathway inhibitor monotherapy is less effective than ADT + androgen receptor pathway inhibitor but appears to be at least as effective as ADT
- Generally, well tolerated, with most adverse events being grade 1–2
- Common adverse events include:
- Gynecomastia and breast pain (notably higher versus ADT)
- Fatigue (common, usually mild)
- Hypertension (class effect)
- Hot flashes (less frequent than with ADT)
- Gastrointestinal symptoms (mild)
- Compared with ADT ± androgen receptor pathway inhibitor:
- Less metabolic toxicity (especially bone loss), sexual dysfunction, and severe fatigue
- Higher gynecomastia/breast tenderness
- Manageable/favorable safety profile with less systemic toxicity than ADT, but no advantage (or disadvantage) in overall quality of life
Presented by: Fred Saad, CQ, MD, FRCS, FCAHS, Professor, Department of Surgery, Raymond Garneau Chair in Prostate Cancer, Director of Prostate Cancer Research, Director of GU Oncology, Université de Montréal, University of Montreal Hospital Centers, CRCHUM, Montréal, QC
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 Advanced Prostate Cancer Consensus Conference (APCCC), Lugano, Switzerland, Thurs, April 30 – Sat, May 2, 2026.
- Freedland SJ, de Almeida Luz M, De Giorgi U, et al. Improved Outcomes with Enzalutamide in Biochemically Recurrent Prostate Cancer. N Engl J Med 2023 Oct 19;389(16):1453-1465.
- Freedland SJ, Gleave M, De Giorgi U, et al. Enzalutamide and Quality of Life in Biochemically Recurrent Prostate Cancer. NEJM Evid. 2023 Dec;2(12):EVIDoa2300251.
- Fazekas T, Miszczyk M, Giesen A, et al. Androgen receptor pathway inhibitor monotherapy in prostate cancer: Safety, oncologic outcomes, and quality of life: A systematic review and meta-analysis. Eur Urol Focus. 2026 Jan;12(1):109-130.
- Shore ND, De Giorgi U, Tutrone RF, et al. Enzalutamide monotherapy for the treatment of prostate cancer with high-risk biochemical recurrence: EMBARK secondary end points. J Urol. 2026 Apr;215(4):396-407.
- Shore ND, Freedland SJ, Horvath LG, et al. Strategies to mitigate breast-related adverse events in patients with high-risk biochemically recurrent prostate cancer receiving enzalutamide monotherapy: Perspectives and challenges. Eur Urol Focus. 2026 Jan;12(1):131-143.