(UroToday.com) The 2026 Advanced Prostate Cancer Consensus Conference (APCCC) meeting featured a monitoring session and a presentation by Dr. Gunhild von Amsberg discussing monitoring in metastatic castration resistant prostate cancer (mCRPC).
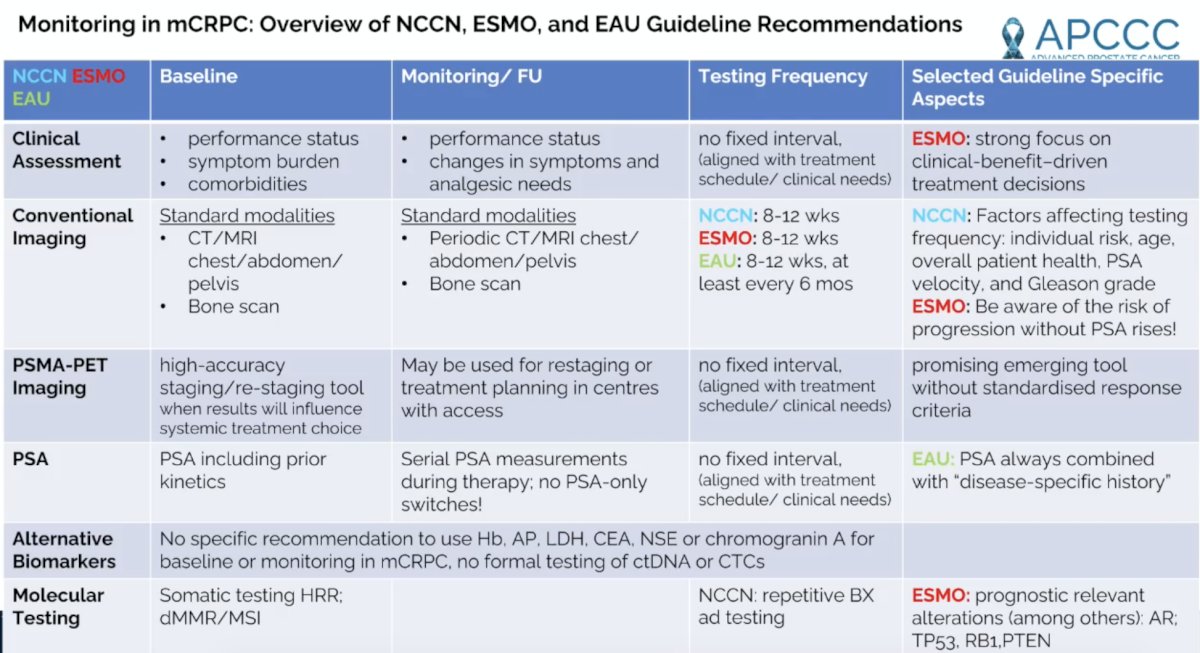
Dr. von Amsberg started her presentation by providing a table summarizing monitoring recommendations in mCRPC based on the NCCN, ESMO, and EAU guidelines:
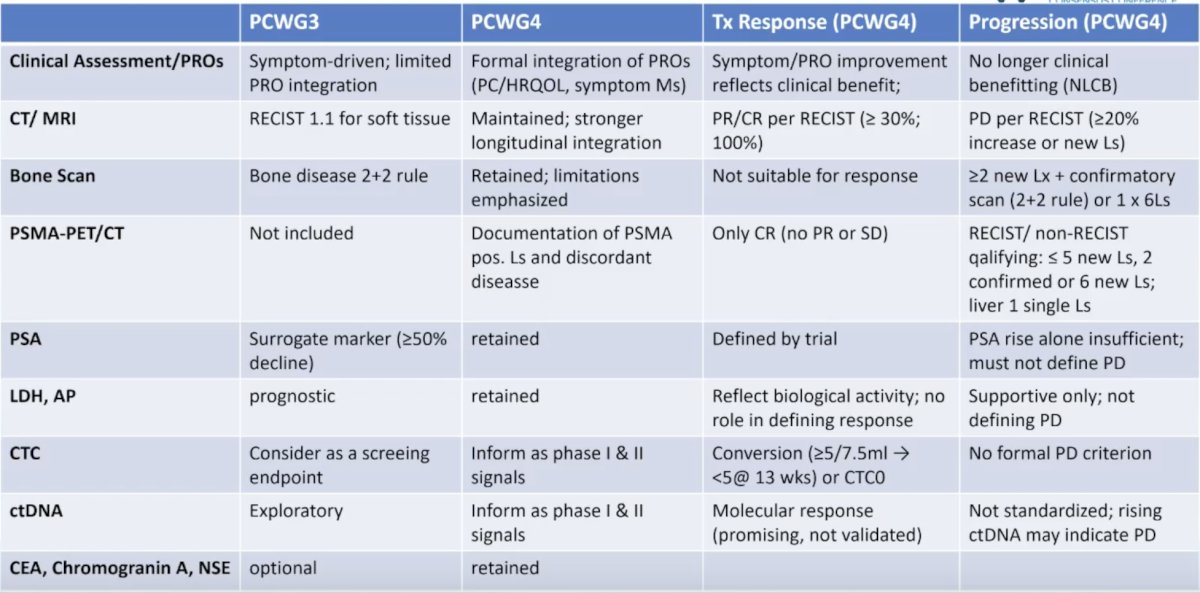
There are also a number of recommendations based on PCWG3 and more recently PCWG4, including for: clinical assessment/patient reported outcomes, CT/MRI, bone scan, PSMA PET/CT, PSA, LDH, ALP, CTCs, ctDNA, and CEA, Chromogranin A, NSE:
Unfortunately, there are limitations of conventional imaging monitoring approaches:
- Bone scan:
• Limited specificity (indirect imaging of osteoplastic activity)
• Flare-up phenomenon
• Delayed progression call/need for confirmation (PCWG3/4: 2+2 rule)
• Underestimation of disease burden (heterogeneous/ osteolytic lesions) - CT scan:
• Limited utility in bone: requires substantial changes in bone density
• No CT scan-specific criteria for assessing bone treatment response
• RECIST 1.1: bone metastases defined as non-measurable disease - PSA:
• Limited sensitivity (PSA-negative progression in up to ~ 30% in mCRPC)
• Biological discordance (poor reflection of heterogeneity/dedifferentiation)
• Therapy-dependent variability
• Not a stand-alone endpoint (no recommendation to change treatment in the guidelines based on PSA alone)
Next-generation imaging includes PSMA PET/CT and whole body MRI. These imaging modalities offer superior sensitivity for detecting metastatic disease compared with conventional imaging and identify biologically active lesions (ie, enabling targeted biopsy). Further, next-generation imaging facilitates treatment selection; however, the prognosis of patients with metastases detected solely by next-generation imaging remains unclear. For PSMA-PET/CT, expression provides high-resolution functional and molecular characterization and quantification of tumor burden, enabling personalized treatment selection. PSMA PET/CT demonstrates superior sensitivity versus whole body MRI for detecting lymph node metastases. However, PSMA PET/CT may underestimate aggressive, dedifferentiated disease due to loss of PSMA. Whole body MRI provides a quantitative assessment of tumor burden and treatment response, particularly in bone metastases. It enables response monitoring (fat fraction; ΔADC) and may aid in identifying aggressive variants (AVPC/NEPC) through assessment of cellularity and bone marrow replacement.
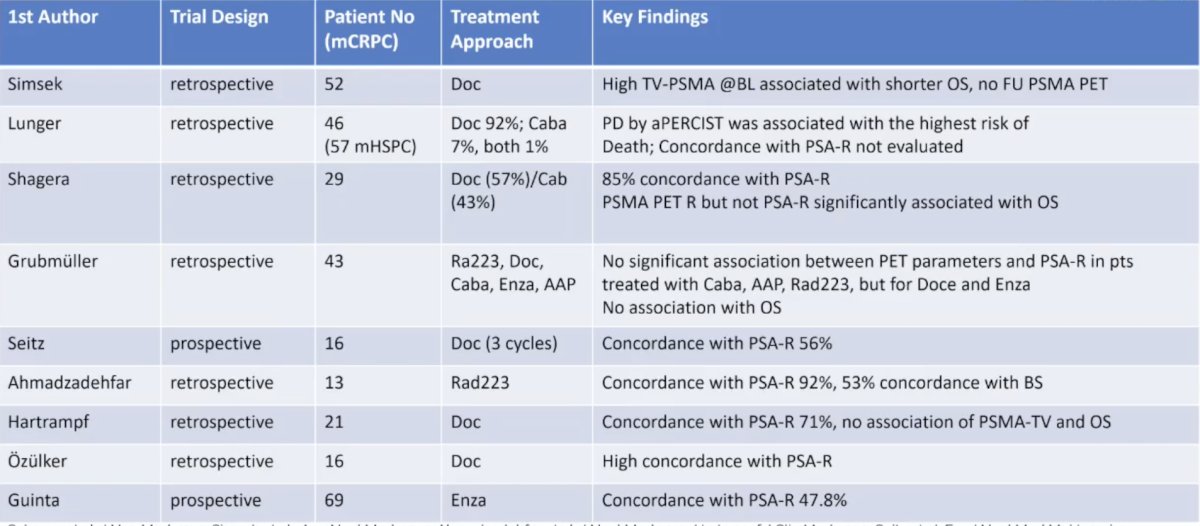
The following table comprises the evidence for PSMA PET/CT for response prediction and monitoring in mCRPC:
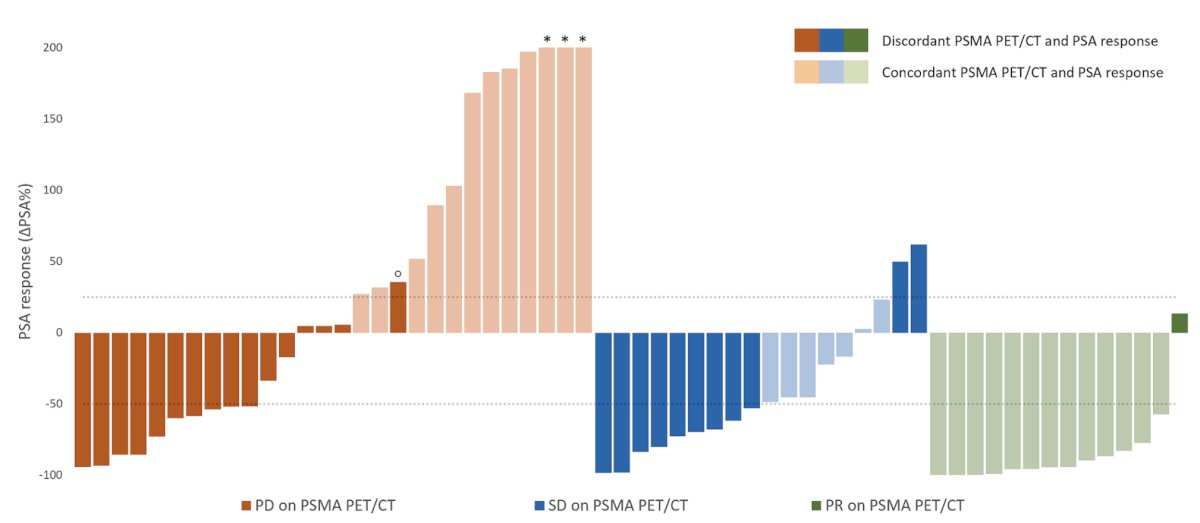
Dr. von Amsberg notes that there is emerging evidence that PSMA PET/CT surpasses PSA for survival prediction in mCRPC. In 2024, Kleiburg et al.1 performed a study that aimed to assess the efficacy of PSMA PET/CT at specific time points for evaluating treatment response and predicting survival in 60 mCRPC patients compared to PSA. PSMA PET/CT and PSA response were discordant in 47 % of patients, and PSMA PET/CT response was worse in 89 % of these cases:
Overall response on PSMA PET/CT independently predicted overall survival (progression versus non-progression: HR 4.05, p < 0.001), outperforming PSA response (progression versus non-progression: HR 2.53, p = 0.010) and other PSMA PET/CT parameters:
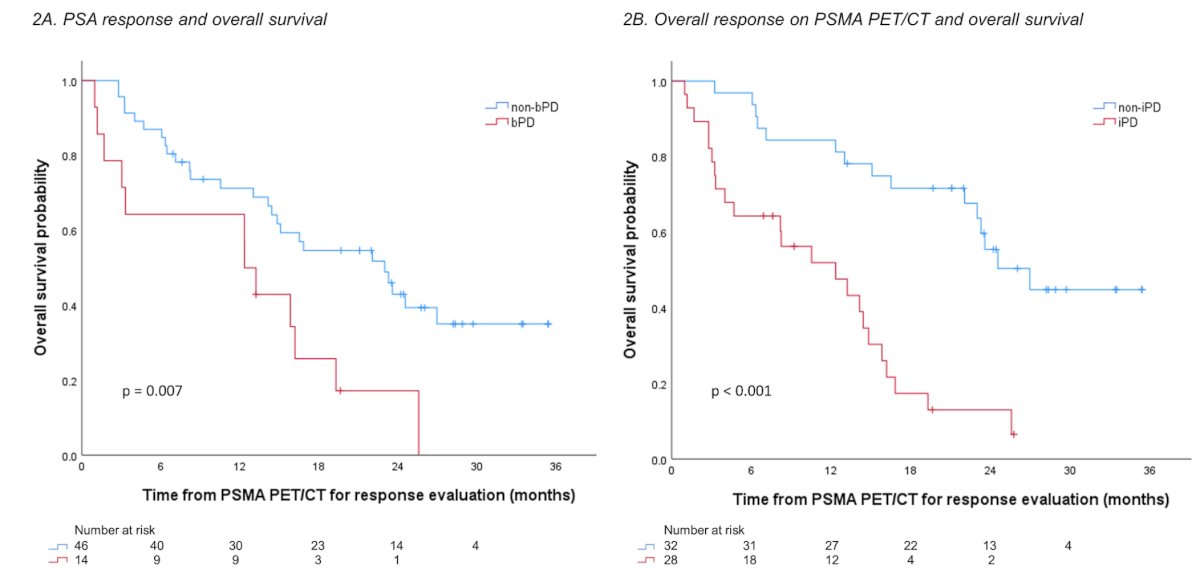
Among patients with a PSA50 response, 31% showed progressive disease on PSMA PET/CT, correlating with higher mortality risk (progression versus non-progression: HR 4.38, p = 0.008).
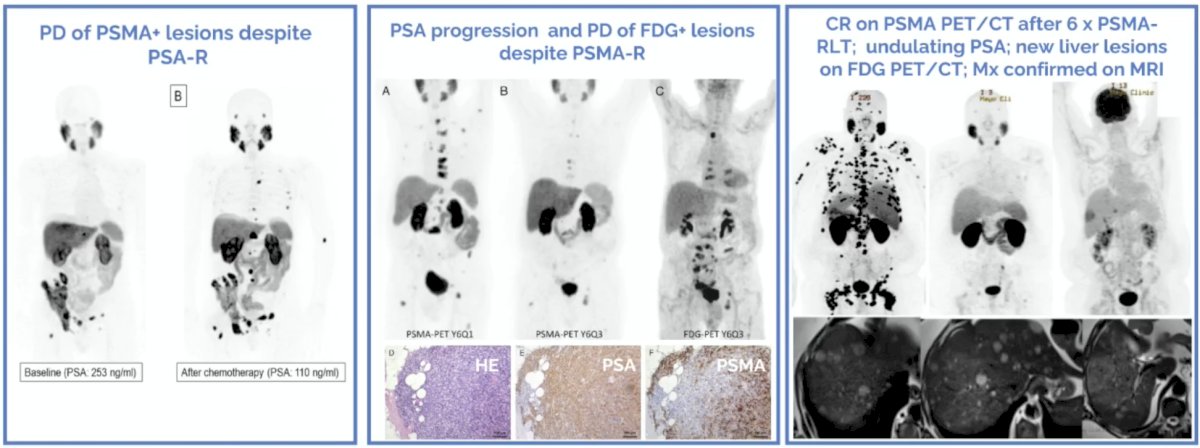
Dr. von Amsberg emphasized that up to 30% of mCRPC patients experience PSA negative progression, and up to ~15-20% of mCRPC patients develop PSMA-low or PSMA-negative disease:
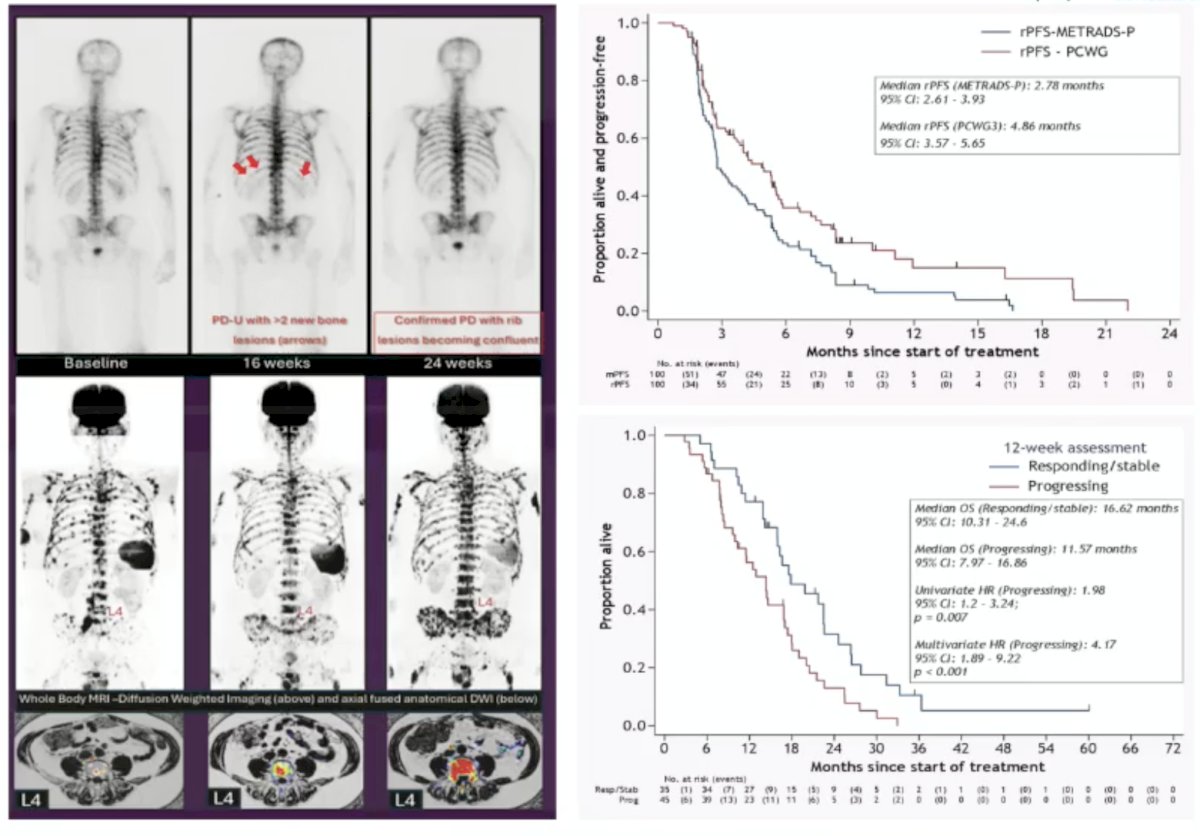
Dr. von Amsberg then discussed whole body MRI, which identifies substantial progression missed by conventional imaging: 43% versus CT and 75% versus bone scan in the PROSPECT interim analysis. Of note, 2/3 of patients achieving a PSA50 response showed progression on whole body MRI. Presented at ASCO 2024, Tunariu et al. assessed discordance between PSA and conventional imaging with whole-body MRI. This study found that whole body MRI detected earlier progression (radiographic progression-free survival by PCWG3) and had prognostic relevance in that progressive disease at 12 weeks is associated with worse overall survival:
Next, Dr. von Amsberg discussed the serum markers NSE, chromogranin A, and CEA. Elevated neuroendocrine markers (NSE and chromogranin A) may be associated with aggressive variant prostate cancer, but lack diagnostic specificity. Increased NSE is associated with poor prognosis in advanced prostate cancer/mCRPC and worse cancer-specific survival for patients treated with an androgen receptor pathway inhibitor. An increasing NSE may indicate PSMA–FDG mismatch and disease heterogeneity, but has limited accuracy for neuroendocrine prostate cancer identification. Increased chromogranin A is associated with worse outcomes in mCRPC (worse progression-free and overall survival), with a stronger prognostic impact in later-line therapy.
A high baseline chromogranin A (≥3× upper limit of normal) and early increased chromogranin A for patients treated with an androgen receptor pathway inhibitor are linked to early progression and treatment resistance. Increased CEA in CRPC is associated with aggressive clinical behavior (liver metastases) and significantly shorter overall survival, which is also seen with PSMA radioligand therapy. An increased CEA is also associated with a distinct genomic profile (ie, increased TP53 SNVs and decreased AR-SNVs), partially overlapping but not identical to AR variant prostate cancer.
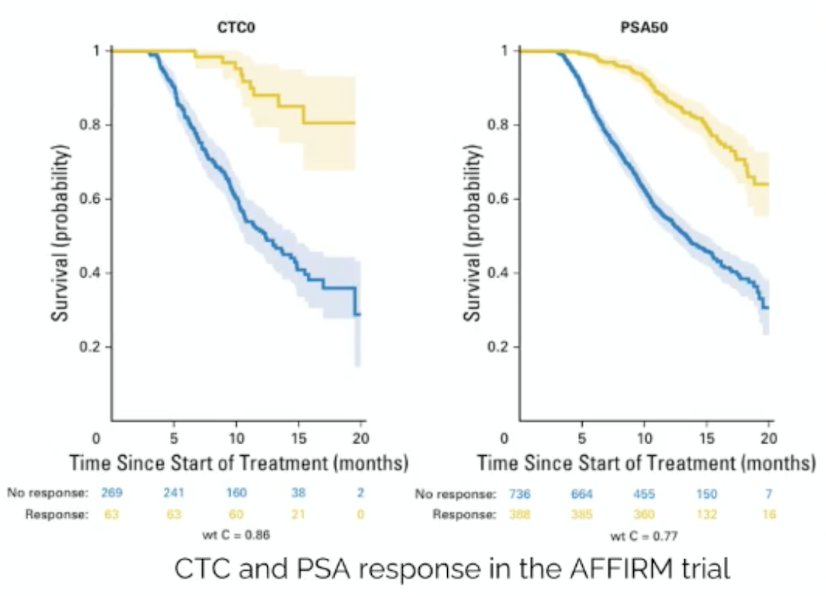
Finally, Dr. von Amsberg discussed CTCs in mCRPC. CTC count (≥5/7.5 mL) is a validated prognostic biomarker in mCRPC, consistently associated with shorter overall survival, and early on-treatment changes in CTC number closely track clinical outcomes. CTC-based response endpoints (conversion ≥5→<5 or CTC0) show stronger associations with overall survival than PSA-based endpoints, and combined CTC/LDH metrics demonstrate robust patient-level surrogacy, but not trial-level surrogacy. CELLSEARCH-enumerated CTCs are FDA-qualified (limited context of use) as a biomarker endpoint for early evaluation of drug activity in mCRPC, functioning as a single-factor response biomarker rather than a validated surrogate for overall survival. The following Kaplan-Meier curves show CTC and PSA response in the AFFIRM trial:
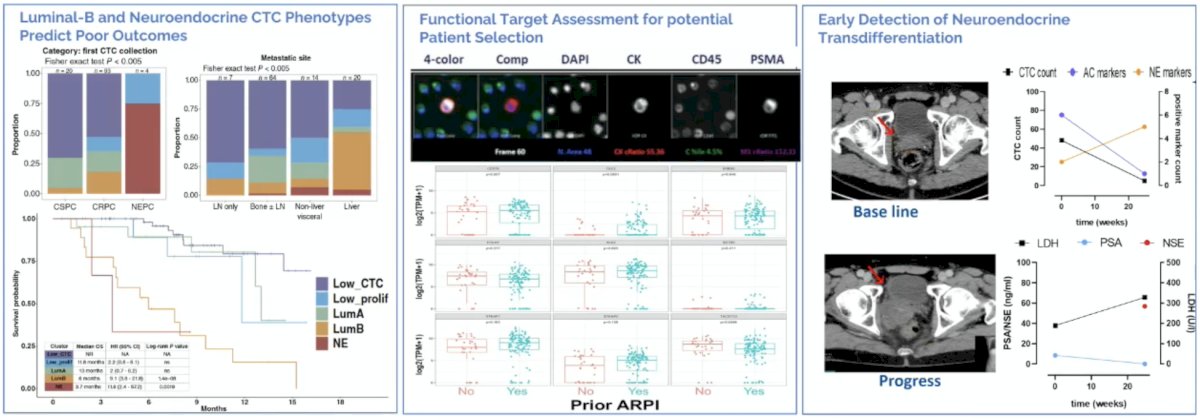
CTCs in mCRPC provide both prognostic and predictive value. Phenotypic CTC profiling captures inter- and intra-patient heterogeneity (AR signaling, EMT, proliferation), and surface-marker profiling reveals pronounced heterogeneity across mCRPC. Functional target assessment enables real-time, protein-level evaluation of therapeutic targets and demonstrates dynamic modulation of target expression. Furthermore, clinical utility supports patient selection, early detection of target escape, and recognition of lineage transitions:
Dr. von Amsberg concluded her presentation discussing monitoring mCRPC with the following take-home points:
- Modern imaging reveals progression that would otherwise remain occult
- Prospective trials must establish whether this improves outcomes
- Conventional imaging remains the standard; however, next-generation imaging should be integrated into clinical trials and considered when it is likely to change management
- PSA alone is insufficient in mCRPC: we should avoid PSA-only treatment switches and remain alert to PSA-negative progression
- Transition to biomarker-driven disease monitoring: With evolving therapies and tumor biology, integration of liquid biopsy is essential
Presented by: Gunhild von Amsberg, Professor, University Cancer Center Hamburg and Martini-Klinik, Hamburg, Germany
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 Advanced Prostate Cancer Consensus Conference (APCCC), Lugano, Switzerland, Thurs, April 30 – Sat, May 2, 2026.
Reference:- Kleibrug F, de Geus-Oei LF, Luelmo SAC, et al. PSMA PET/CT for treatment response evaluation at predefined time points is superior to PSA response for predicting survival in metastatic castration-resistant prostate cancer patients. Eur J Radiol. 2024 Dec:181:111774.