(UroToday.com) The 2026 Advanced Prostate Cancer Consensus Conference (APCCC) meeting featured a radioligand and radionuclide therapy in advanced prostate cancer session and a presentation by Dr. Louise Emmett discussing how to make the best use of Lutetium-PSMA radioligand therapy. Simply put: should we be using 177Lu-PSMA-617 in the mHSPC or mCRPC disease space?
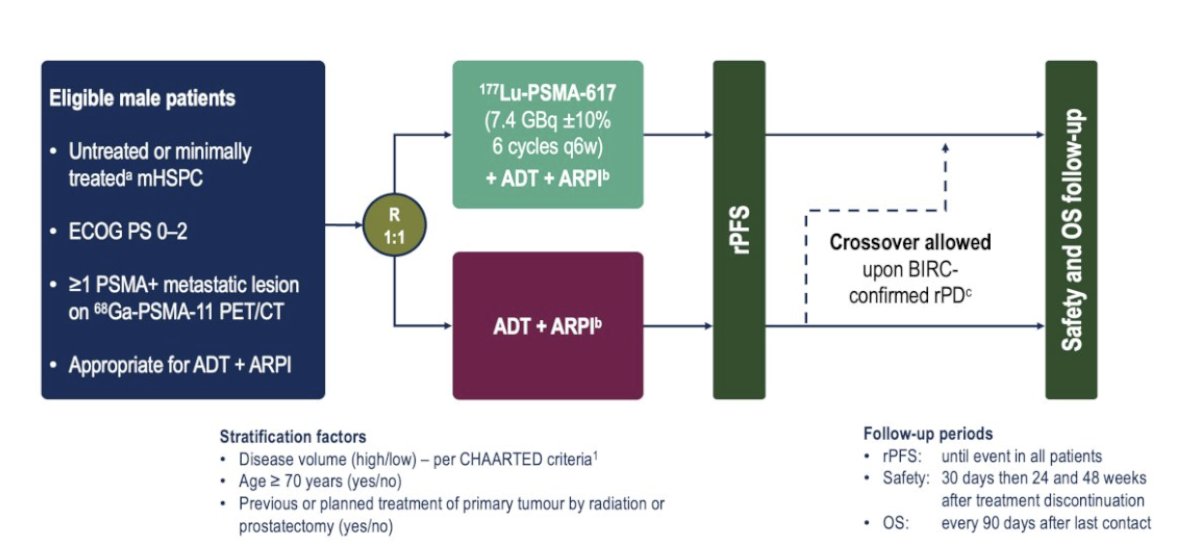
The PSMAddition trial randomized men with untreated or minimally treated mHSPC and ≥1 PSMA-positive metastatic lesion on 68Ga-PSMA-11 PET/CT to the experimental arm of 177Lu-PSMA 617 (7.4 GBq ±10% 6 cycles every 6 weeks) + ADT + androgen receptor pathway inhibitor versus the control arm of ADT + androgen receptor pathway inhibitor. Of note, crossover to the 177Lu-PSMA 617 arm was permitted upon radiographic progression:
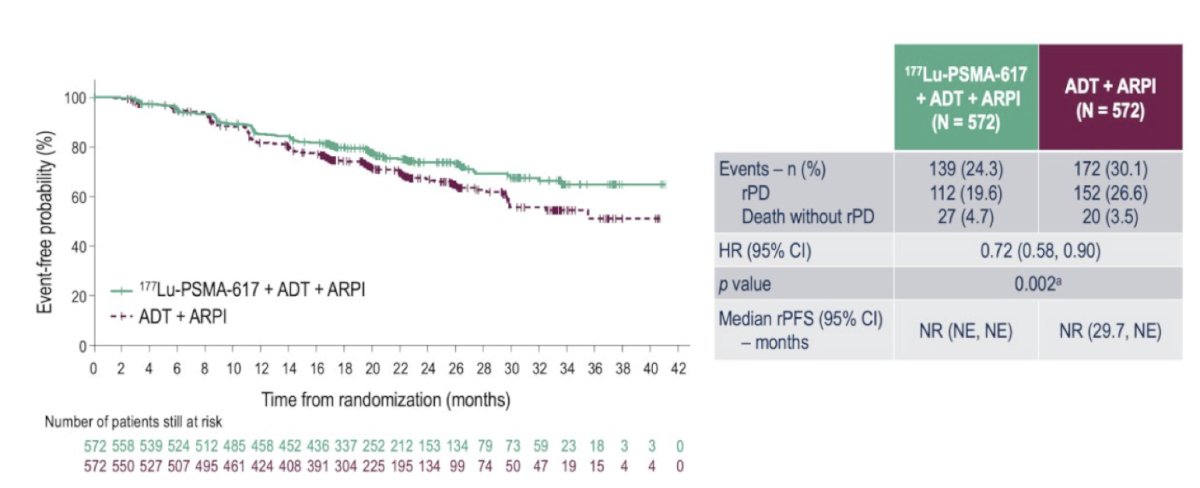
The study met its primary endpoint with radiographic progression-free survival significantly prolonged with the addition of 177Lu-PSMA-617 (HR 0.72, 95% CI 0.58-0.90; p = 0.002). The median radiographic progression-free survival has not been reached in either arm:
Beyond PSMAddition (ie, post-177Lu-PSMA-617), there are several key trials in the second-line radioligand therapy space:
- PSMAcTION: a phase 3 trial of 225Ac-PSMA-617 versus standard of care post 177Lu-PSMA-617
- AcTFirst: a phase 3 trial of 225Ac-PSMA-617 versus standard of care (including 177Lu-PSMA-617)
- Other radionuclides: 212Pb-PSMA, 67Cu-PSMA, 225Ac-PSMA-tris poc, 225Ac-PSMA-I&T
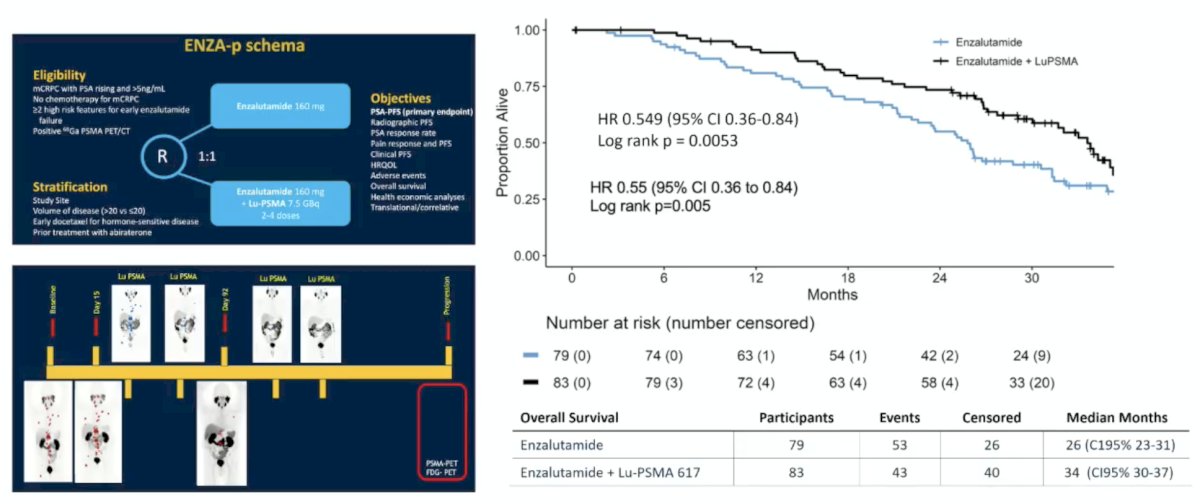
What about adding an androgen receptor pathway inhibitor? The ENZA-p trial1 assessed 177Lu-PSMA-617 + enzalutamide versus enzalutamide monotherapy. The impetus for this study is that enzalutamide has been shown to upregulate the expression of PSMA on subsequent imaging. ENZA-p included mCRPC patients not previously treated with chemotherapy or androgen receptor pathway inhibitors (prior abiraterone and/or docetaxel for hormone-sensitive disease were allowed), 68Ga-PSMA-positive disease on PET, and at least 2 risk factors associated with early progression on enzalutamide. In the enzalutamide + 177Lu-PSMA-617 arm, 81% of patients received four doses of 177Lu-PSMA-617. PSA50 and PSA90 improved with 177Lu-PSMA-617 + enzalutamide. Over a median follow-up of 20 months (IQR 18-21), PSA progression-free survival was longer with enzalutamide + 177Lu-PSMA-617 vs enzalutamide-alone (median 13 vs 7.8 months; HR 0.43, 95% CI 0.29-0.63, p < 0.001). There was also a trend towards improved radiographic progression-free survival favoring 177Lu-PSMA-617 (HR 0.68, 95% CI 0.45-1.03):
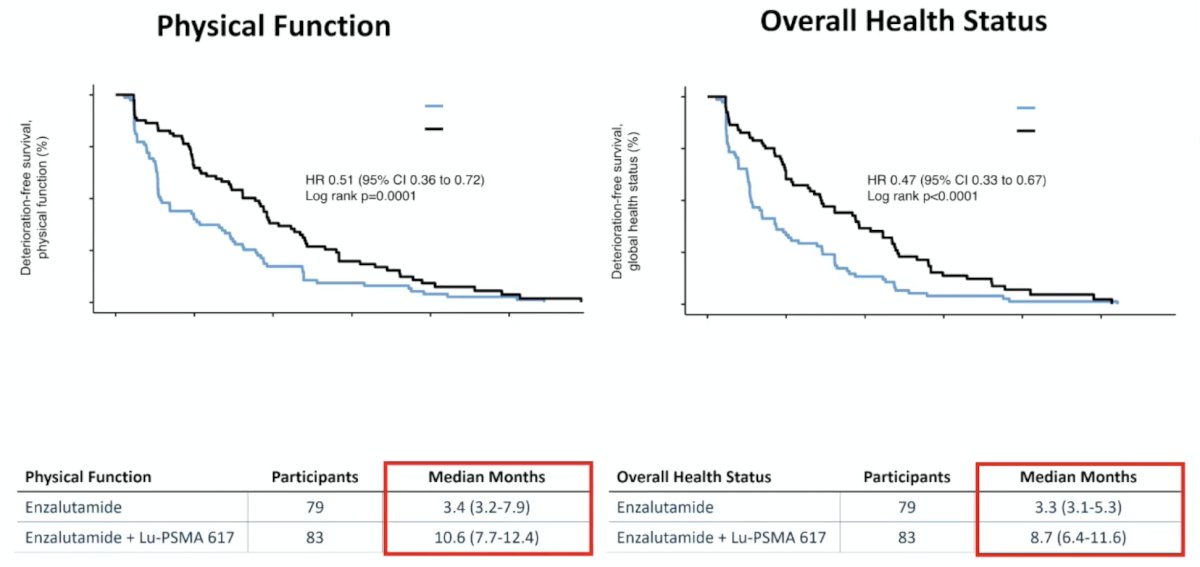
Health-related quality of life was rated by 154 of 162 participants (95%). With regards to deterioration-free survival, this favored enzalutamide + 177Lu-PSMA-617 for both physical function (HR 0.51, 95% CI 0.36 – 0.72) and overall health status (HR 0.47, 95% CI 0.33 – 0.67):
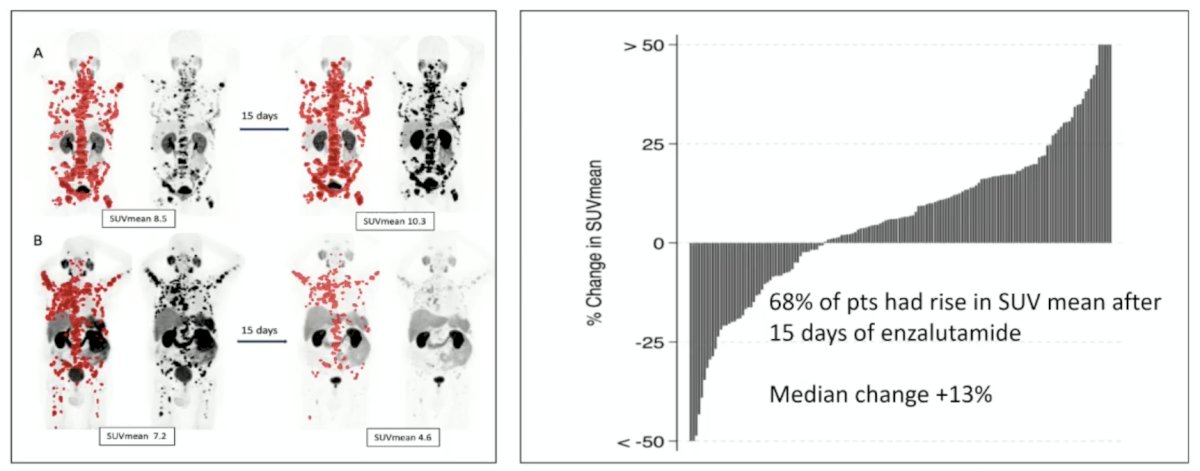
Published earlier in 2026, Emmett et al.2 evaluated the predictive value of early PSMA upregulation for the response to enzalutamide +/- 177Lu-PSMA-617 among patients in ENZA-p. Notably, 68% of patients had a rise in SUVmean after 15 days of enzalutamide:
PSA response with early PSMA expression change is highlighted in the following figure:
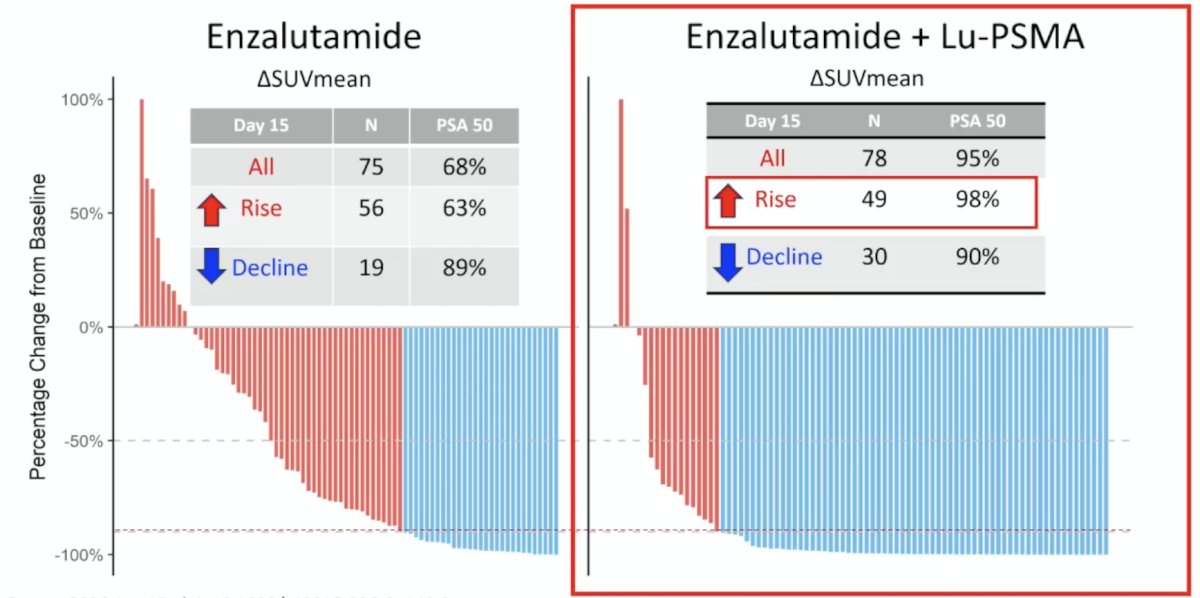
The median PSA progression-free survival with increasing SUV mean at day 15 was 5.8 (95% CI 4.0-8.7) versus 13.1 (95%CI 10.5-17.0) months for enzalutamide versus enzalutamide + 177Lu-PSMA-617 (HR 0.38, 95%CI 0.25-0.58). With decreasing SUV mean, the median PSA progression-free survival was 12.5 (95%CI 3.2-23.6) versus 13.3 (95%CI 9.6-22.2) months for enzalutamide versus enzalutamide + 177Lu-PSMA-617 (HR 0.80, 95%CI 0.42-1.53). The interaction between SUV mean increase or decrease, and treatment arm for PSA progression-free survival was p = 0.055. Thus, the addition of 177Lu-PSMA-617 to enzalutamide mitigated the short PSA progression-free survival in those with early PSMA SUV mean increase.
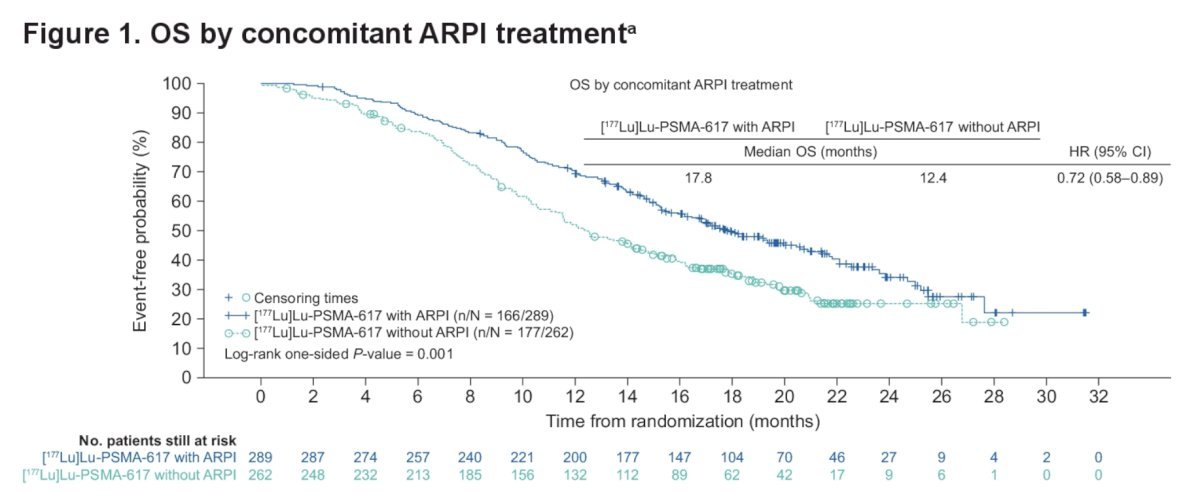
Presented at ASCO GU 2025, Dr. Omid Yazdanpanah discussed a secondary analysis of the VISION trial assessing the efficacy of 177Lu-PSMA-617 with or without androgen receptor pathway inhibitors for the treatment of mCRPC. A statistically significant difference in median overall survival was observed in patients treated with concomitant androgen receptor pathway inhibitors versus those without (17.8 versus 12.4 months; HR 0.72; 95% CI 0.58–0.89; nominal p = 0.001):
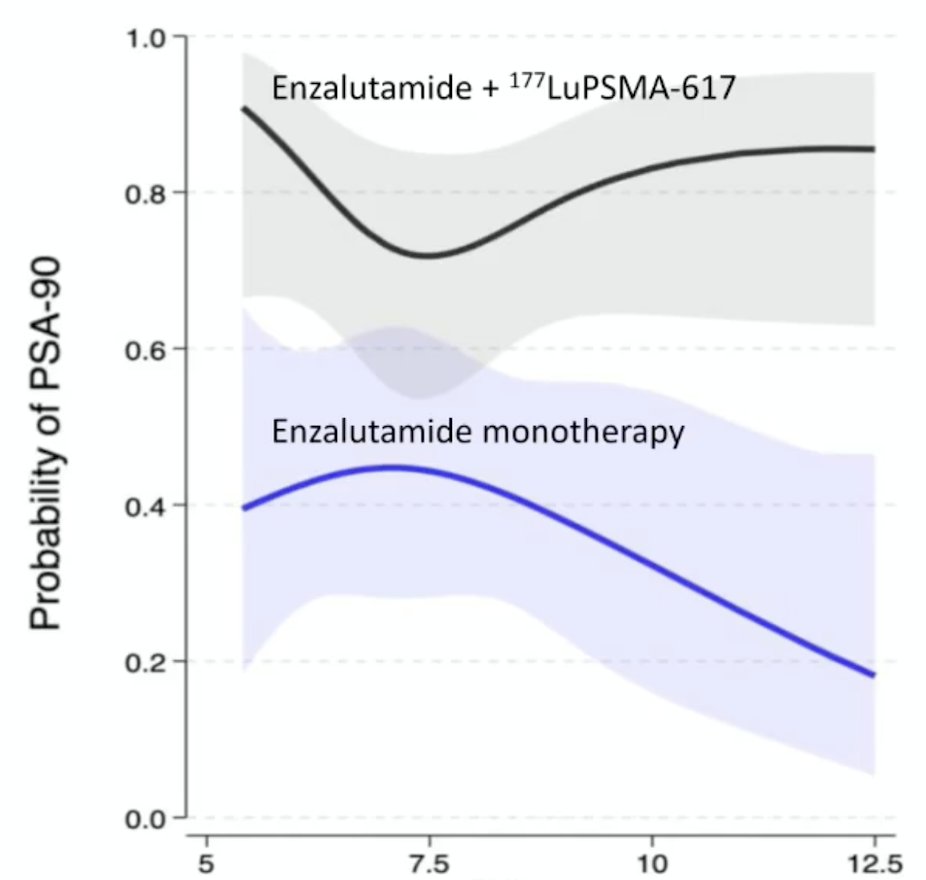
Dr. Emmett notes that enzalutamide and 177Lu-PSMA-617 likely have complementary co-targeting. Baseline SUVmean stratifies treatment response to enzalutamide: in the enzalutamide monotherapy arm, baseline SUVmean >7.7 had a PSA90 RR of 27%; baseline SUVmean < 7.7 PSA90 had a RR of 47%:
In 2023, Dr. Emmett and colleagues reported results of their study evaluating progression-free survival and overall survival based on treatment interval adjustment utilizing 177LuPSMA 24-hour SPECT/CT and early PSA response.4 There were 125 men treated with 6 times weekly 177LuPSMA-I&T doses (median 3 cycles, IQR 2-4) at a median dose of 8.0 GBq (95% CI 7.5-8.0). Following dose 2 (week 6), a composite PSA and 177LuPSMA 24-hour SPECT/CT imaging response determined ongoing management:
- Response Group 1 (marked reduction in PSA/imaging partial response): break in treatment until subsequent PSA rise, then re-treatment
- Response Group 2 (stable or reduced PSA and/or imaging stable disease): 6-weekly treatments until six doses, or no longer clinically benefiting
- Response Group 3 (rise in PSA and/or imaging progressive disease): recommend for alternative treatment
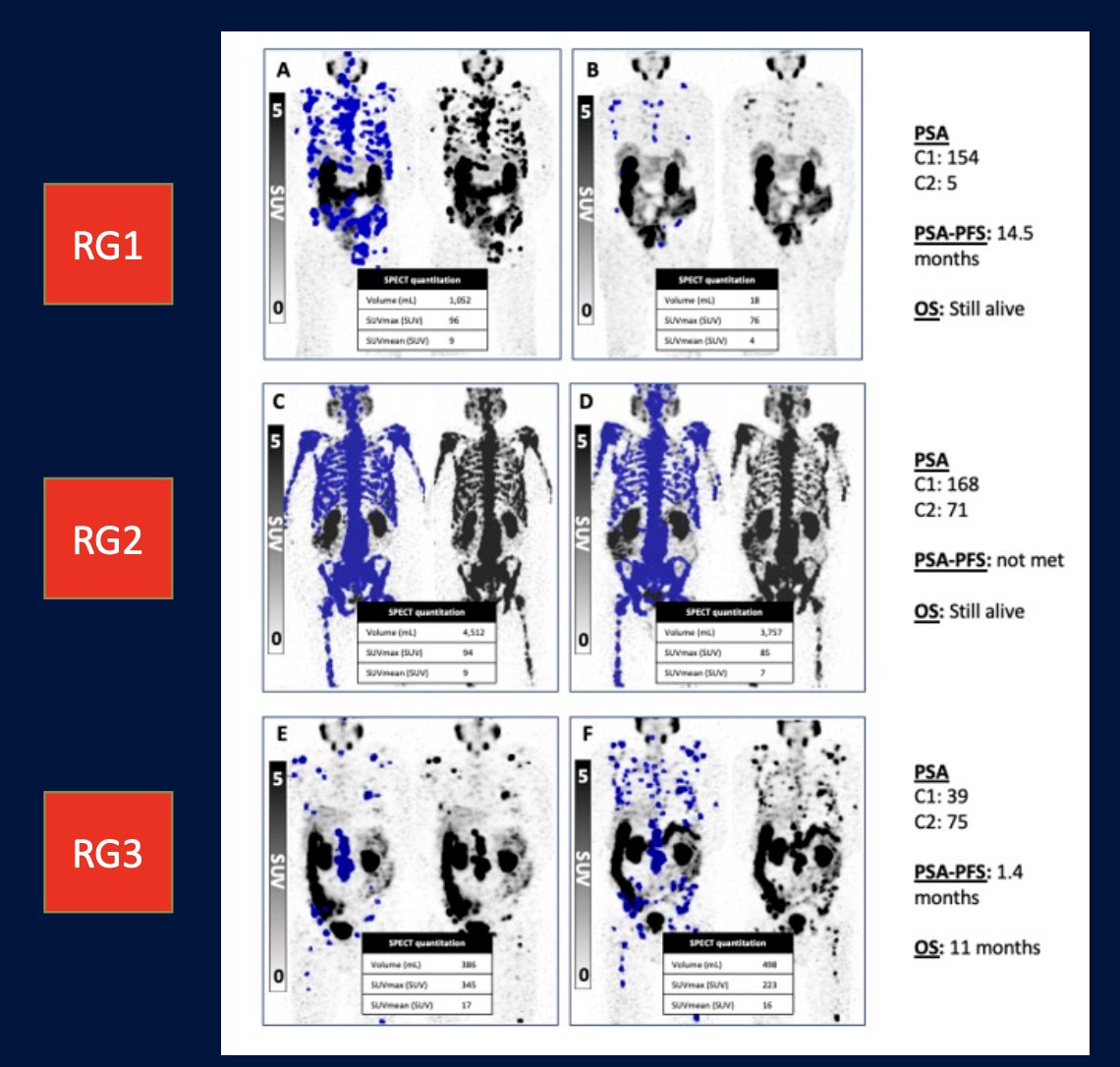
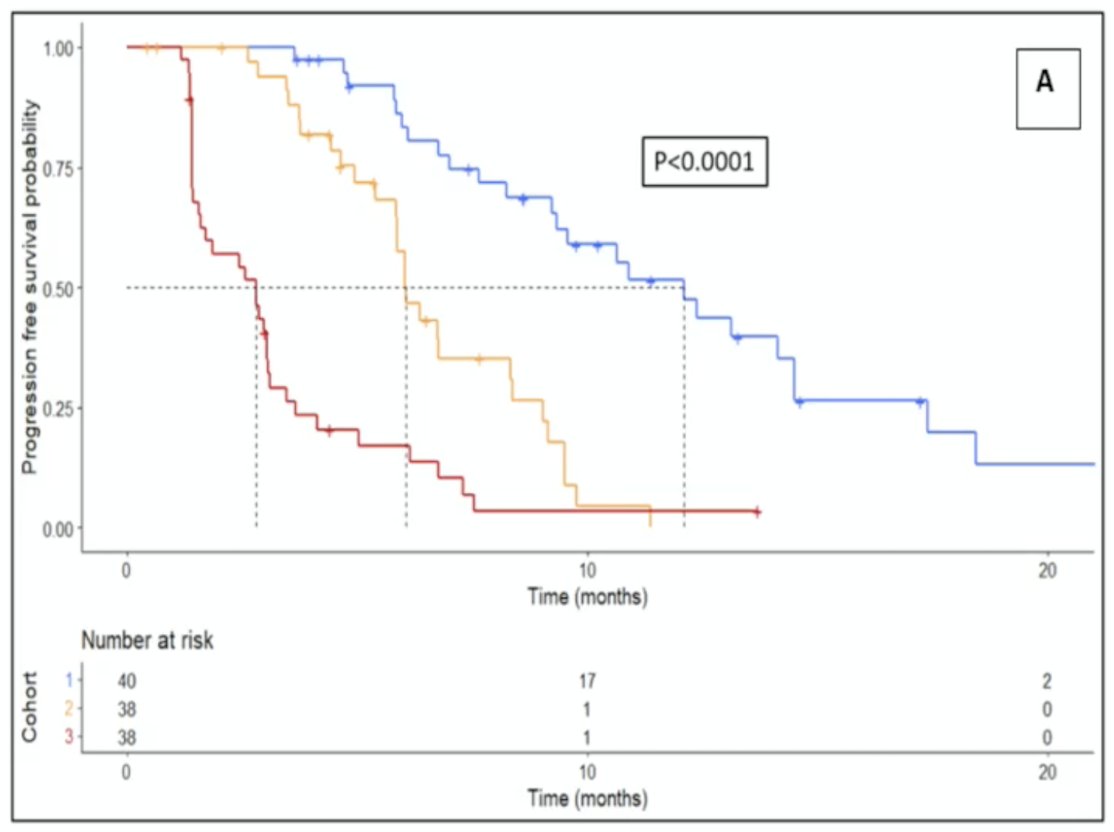
The results were as follows:
- Response Group 1: progression-free survival 12.3 months, overall survival 22 months, treatment break for 6 months
- Response Group 2: progression-free survival 6.2 months, overall survival 15 months, no treatment break
- Response Group 3: progression-free survival 2.8 months, overall survival 11 months, early more to alternative treatment
Taken together, re-treatment with 177Lu-PSMA-617 at PSA rise after treatment pause had a PSA50 response rate range of 37-73%.
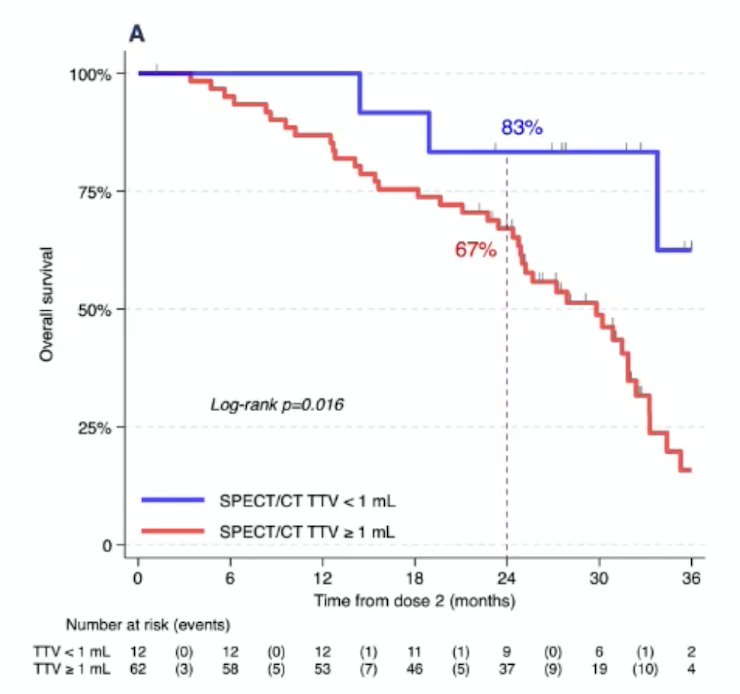
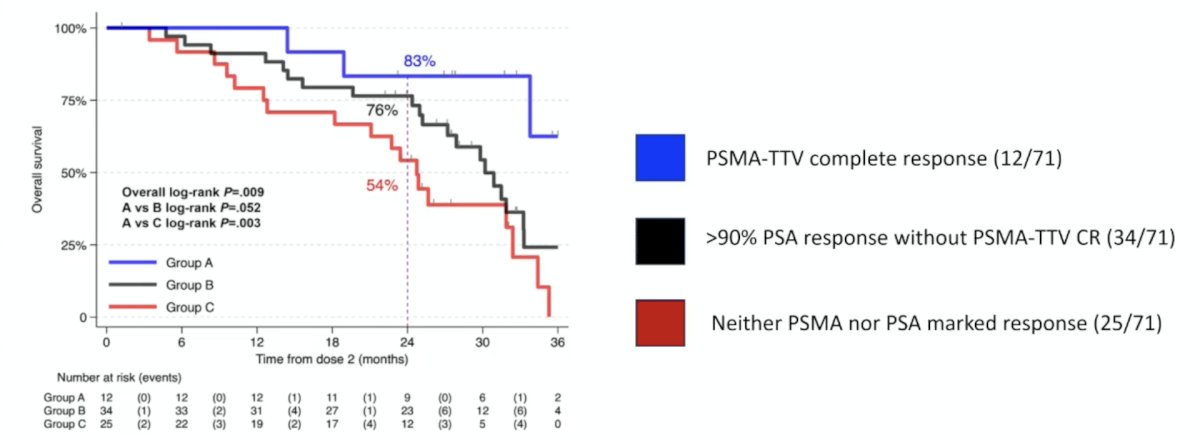
In a recently published analysis from ENZA-p, Ayati et al.5 aimed to predict overall survival after enzalutamide + 177Lu-PSMA-617 using quantitative parameters at 177Lu-PSMA-617 SPECT/CT at 6 weeks, as well as PSA response. The 2-year survival rate with total tumor volume complete response was 83% (95% CI 48, 96), versus 67% (95% CI 54, 77) without total tumor volume complete response (HR 0.26, 95% CI 0.08-0.85; log-rank p = 0.02):
The 2-year survival rate was 76% (95% CI 58, 87) with deep PSA response without total tumor volume complete response (log-rank p = 0.05 versus total tumor volume complete response) and 54% (95% CI 33, 71) with neither deep PSA response nor total tumor volume complete response (log-rank p = 0.003 versus total tumor volume complete response):
Finally, Dr. Emmett discussed three key trials in progress. The FLEX-MRT trial is an investigator-initiated prospective phase 2, open-label, randomized, controlled, parallel group, single-center trial. The aim is to assess the 2-year survival rate in mCRPC patients treated with a flexible dosing schedule of 177Lu-PSMA radiopharmaceutical therapy up to 12 cycles in comparison to the fixed dosing schedule of 6 cycles. Patients with progressive mCRPC post-androgen receptor pathway inhibitor and post-taxane-based chemotherapy are eligible by PSMA PET VISION trial criteria. The overview of the study design is as follows:
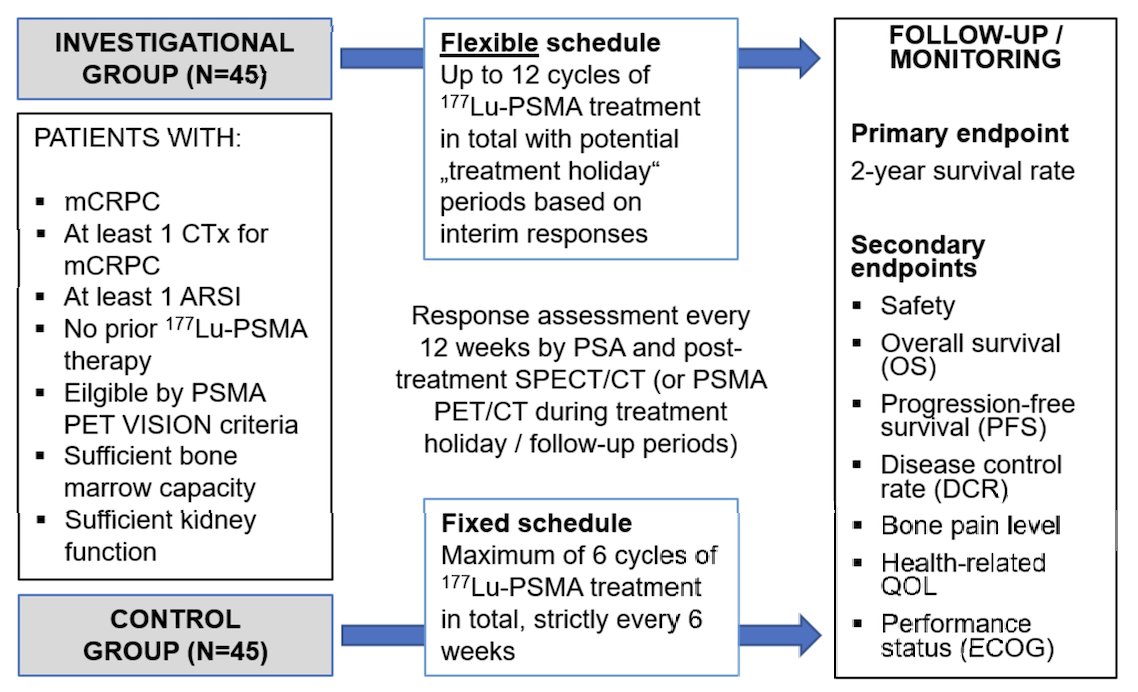
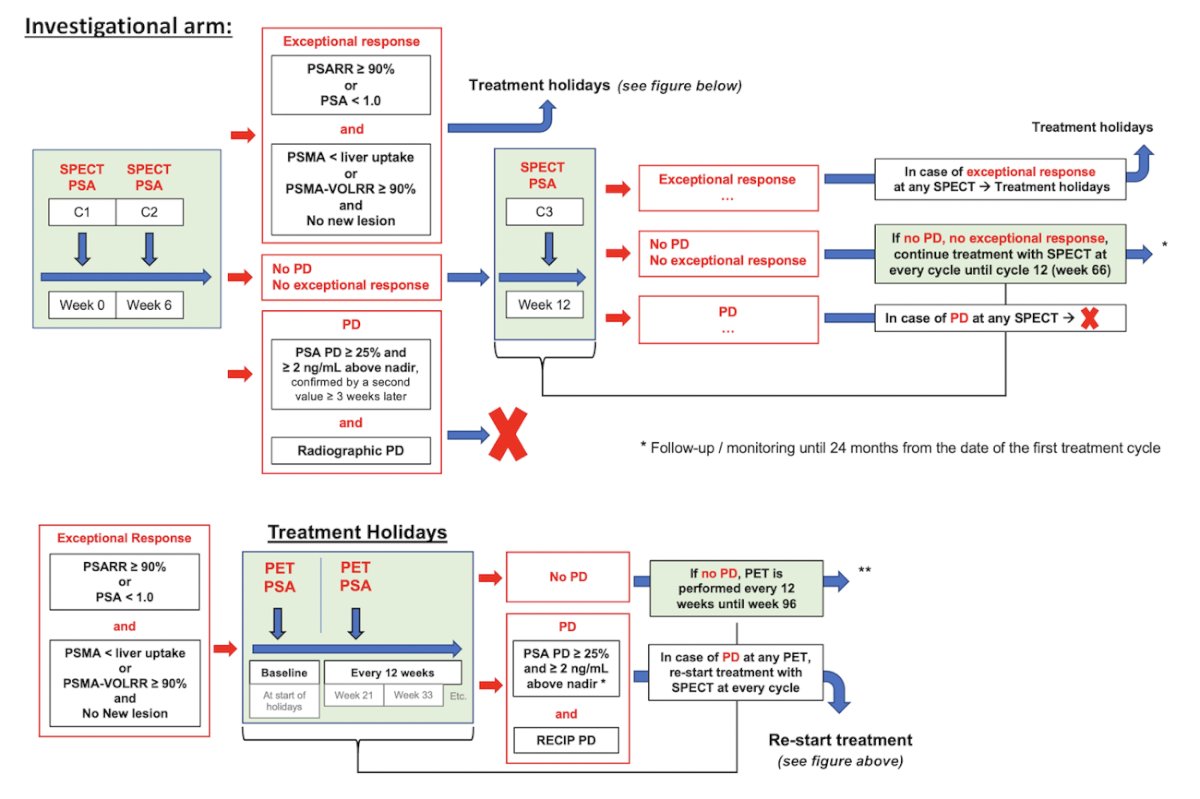
Imaging response to radiopharmaceutical therapy is assessed using 177Lu-PSMA-617 SPECT/CT after each cycle and PSMA PET/CT during treatment holidays (every 12 weeks), respectively. In the investigational arm, radiopharmaceutical therapy will be re-started after a treatment holiday if the patient experiences a ≥25% PSA progression and an imaging progression according to the RECIP:
The primary endpoint is the 2-year survival rate calculated from the date of the first cycle of radiopharmaceutical therapy.
The OPTIMAL-PSMA randomized phase II trial aims to determine the safety and efficacy of a dosing regimen comprised of an intense induction followed by a maintenance period of 177Lu-PSMA-597 therapy, compared to standard of care 6 doses weekly in men with mCRPC. Part A in the figure below visually demonstrates the induction sequence (Days 1, 3, and 15) followed by extended-interval maintenance dosing. In contrast, the control arm receives standard 7.4 GBq dosing every 6 weeks for six cycles:
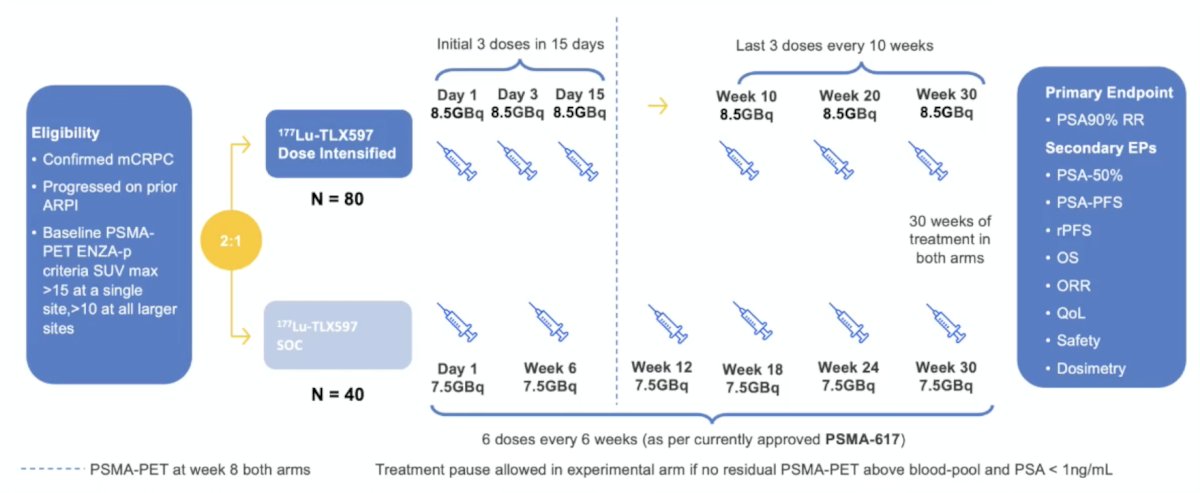
The primary endpoint is PSA50 response.
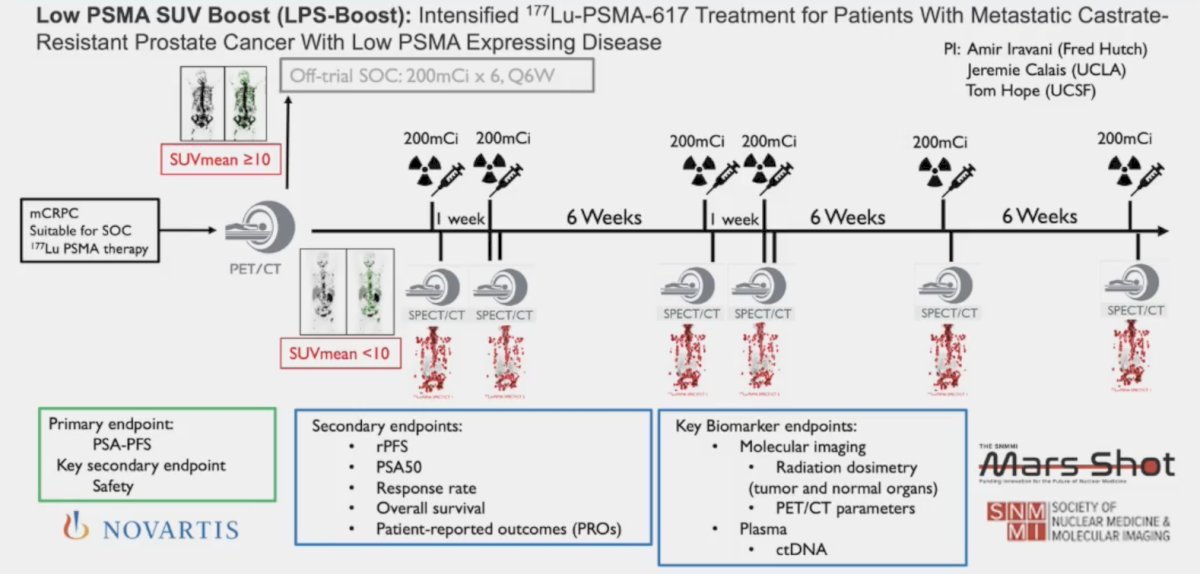
As part of intensifying treatment up front, Dr. Emmett also highlighted biomarker-modulated PSMA theranostics (NCT0656299), whereby low PSMA mCRPC patients are treatment intensified with 177Lu-PSMA-617:
Dr. Emmett concluded her presentation discussing how to make the best use of Lutetium-PSMA radioligand therapy with the following take-home points:
- Rapid change with 177Lu-PSMA-617 is likely moving earlier to mHSPC and alpha PSMA moving into the mCRPC space
- Consider the addition of an adjunctive androgen receptor pathway inhibitor to 177Lu-PSMA-617 in mCRPC – there is good rationale, but we need evidence
- Adaptive dosing using on treatment biomarkers with treatment pause in marked responders is appealing to patients and may reduce toxicity with a good chance of PSA response at re-challenge
- Early dose intensification may deepen treatment responses – toxicity is unknown – but trials are in progress
Presented by: Louise Emmett, MD, MBChB, FRACP, FAANMS, Professor, Director of Theranostics and Nuclear Medicine, St. Vincent’s Hospital Sydney, University of New South Wales, Sydney, Australia
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 Advanced Prostate Cancer Consensus Conference (APCCC), Lugano, Switzerland, Thurs, April 30 – Sat, May 2, 2026.
Related content: Adaptive Dosing of Lutetium PSMA Based on Imaging and PSA Response - Louise Emmett
- Emmett L, Subramaniam S, Crumbaker M, et a. [177Lu]Lu-PSMA-617 plus enzalutamide in patients with metastatic castration-resistant prostate cancer (ENZA-p): An open-label, multicentre, randomized, phase 2 trial. Lancet Oncol. 2024 May;25(5):563-571.
- Emmett L, Swiha M, Papa N, et al. Predictive value of early PSMA upregulation for the response to enzalutamide +/- 177Lu-PSMA-617 in poor-risk, metastatic, castration-resistant prostate cancer: Substudy of the randomized, phase 2 ENZA-p trial. Nat Cancer. 2026 Apr;7(4):622-630.
- Emmett L, Papa N, Subramaniam S, et al. Prognostic and predictive value of baseline PSMA-PET total tumour volume and SUVmean in metastatic castration-resistant prostate cancer in ENZA-p (ANZUP1901): A substudy from a multicentre, open-label, randomized, phase 2 trial. Lancet Oncol. 2025 Sep;26(9):1168-1177.
- Emmett L, John N, Pathmanandavel S, et al. Patient outcomes following a response biomarker-guided approach to treatment using 177Lu-PSMA-I&T in men with metastatic castrate-resistant prostate cancer (Re-SPECT). Ther Adv Med Oncol. 2023 Mar 1:15:17588359231156392.
- Ayati N, Papa N, Crumbaker M, et al. 177Lu-PSMA-617 SPECT/CT for early prediction of overall survival in participants with metastatic castration-resistant prostate cancer. Radiology. 2026 Apr;319(1):e252672.