(UroToday.com) The 2026 Advanced Prostate Cancer Consensus Conference (APCCC) meeting featured a radioligand and radionuclide therapy in advanced prostate cancer session and a presentation by Dr. Maha Hussain discussing emerging new therapies and what will likely be available in the next 2 years.
In 2026 and beyond, there are many treatment options for mCRPC. The following treatments have established a survival/progression-free survival improvement:
- Docetaxel
- Sipuleucel-T
- Cabazitaxel
- Abiraterone + Prednisone
- Enzalutamide
- Apalutamide
- Radium-223
- Olaparib
- Rucaparib
- LuPSMA
- Abiraterone + Olaparib
- Enzalutamide + Talazoparib
- Abiraterone + Niraparib
Additionally, a clinical benefit has been shown for pembrolizumab, and skeletal-related adverse events can be decreased with the addition of zoledronic acid and denosumab. Dr. Hussain emphasized that there are many clinical considerations for choosing therapy:
- Prior therapy in mHSPC, nmCRPC, mCRPC
- Performance status, symptoms, comorbidities, potential for tolerability
- Drug availability, cost, logistics
- Genomics
- Patient preferences
- Access to clinical trials
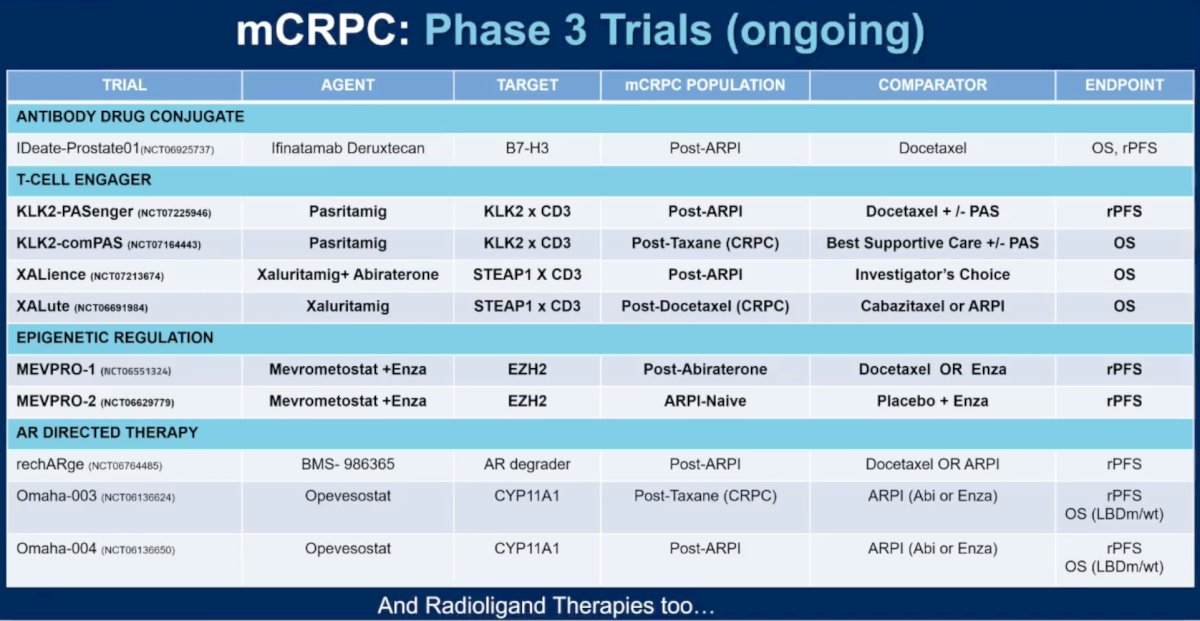
Currently, there are several pathway-targeted agents being evaluated, which include: (i) androgen receptor degraders, (ii) actinium-225, (iii) EZH2 inhibitors, (iv) PROTACs, (v) T cell engagers, and (vi) others. The following table highlights the ongoing mCRPC phase 3 trials:
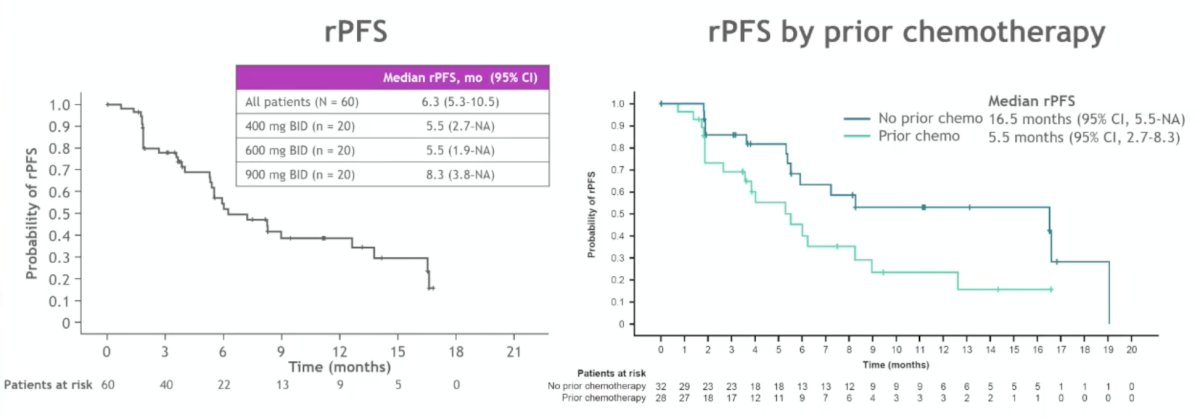
In a phase 1 multicenter trial assessing BMS-986365, patients were enrolled who had progressed on ADT, one or more androgen receptor pathway inhibitors, and taxane chemotherapy.1 There were 27 patients enrolled in the dose escalation portion of the trial, and 68 patients enrolled in the expansion cohort. In the expansion cohort, the median number of prior therapies was 4 (range: 2-11). Across the expansion cohort’s three highest doses (400-900 mg twice daily, n = 60), PSA50 was 32% (n = 19), including 50% (n = 10/20) at 900 mg. The median radiographic progression-free survival was 6.3 months (95% CI 5.3-12.6), including 8.3 months (95% CI 3.8-16.6 months) at 900 mg. Radiographic progression-free survival was longer in patients without versus with prior chemotherapy: 16.5 months (95% CI 5.5 -not evaluable) versus 5.5 months (95% CI 2.7-8.3), respectively:
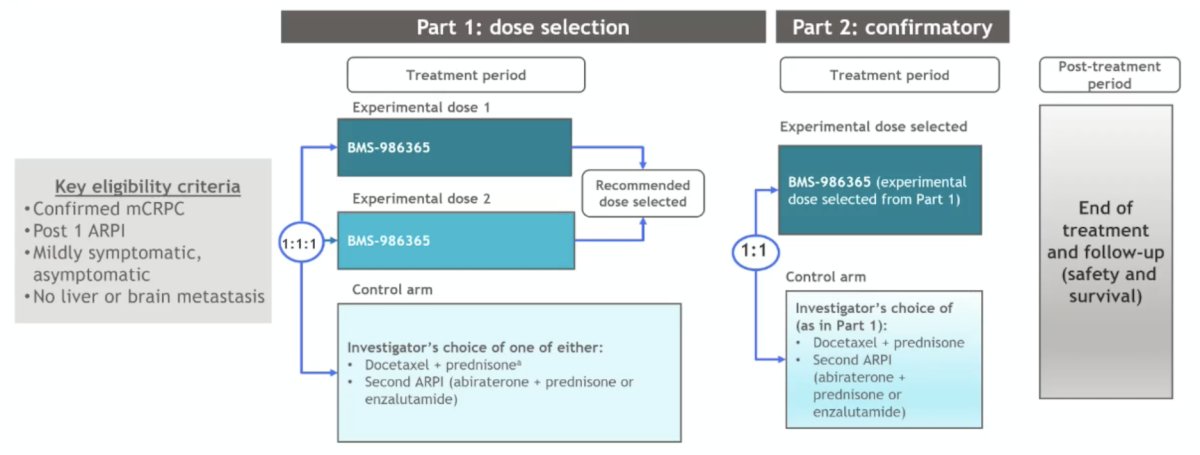
Currently, the rechARge phase 3 trial is enrolling 960 patients, randomizing patients 1:1:1 to two different doses of BMS-986365 or a control arm of the investigator’s choice of either docetaxel + prednisone/prednisolone or a secondary androgen receptor pathway inhibitor:
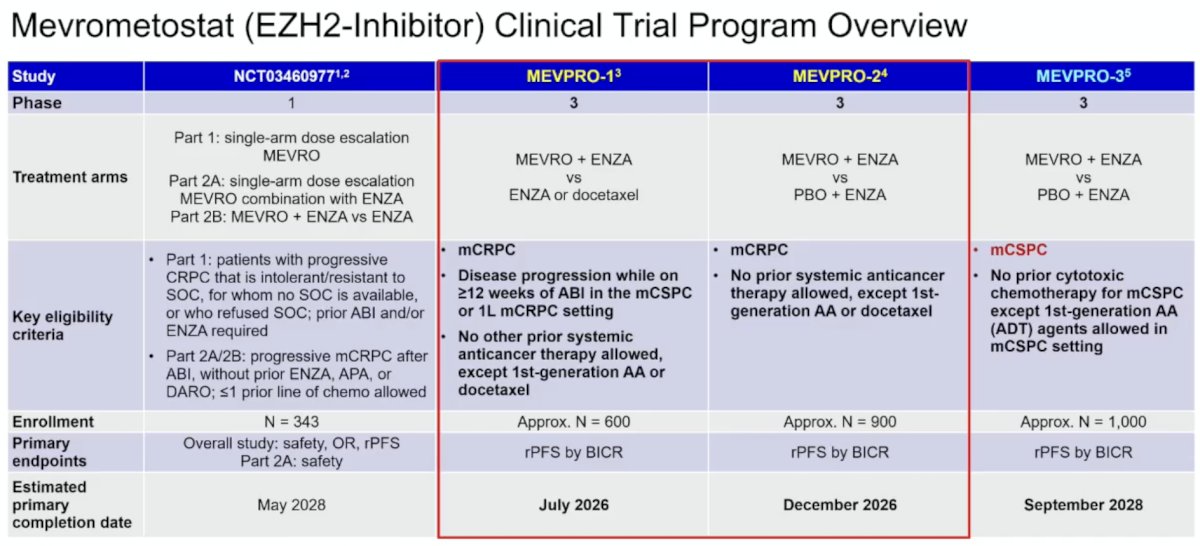
Mevrometostat is an EZH2 inhibitor with a robust clinical trial program overview:
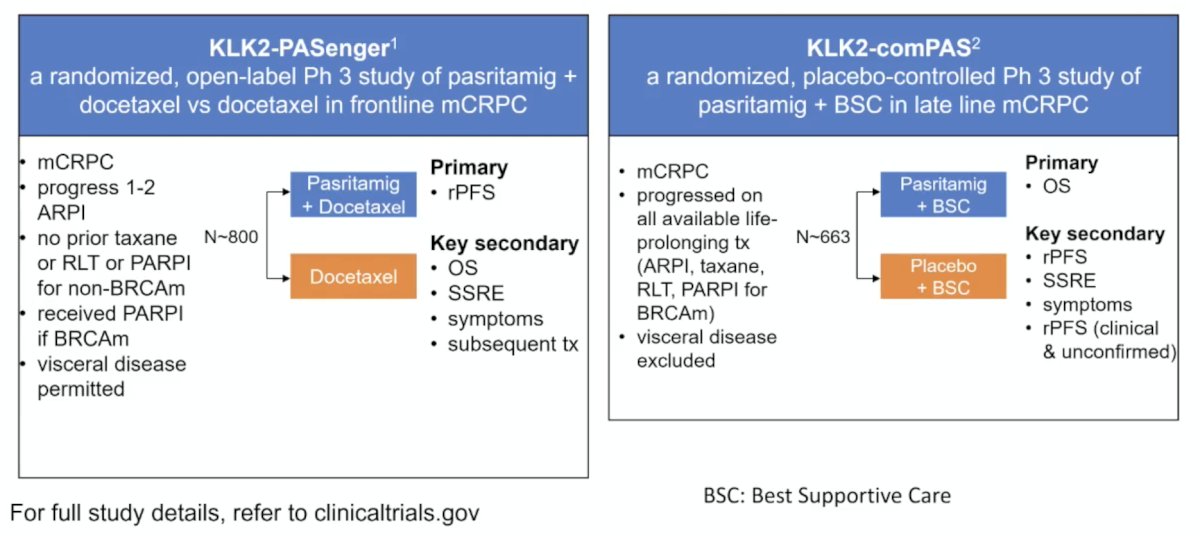
Dr. Hussain notes that there are two ongoing phase 3 studies with pasritamig in mCRPC. The first is KLK2-PASenger, a randomized, open-label phase 3 study of pasritamig + docetaxel versus docetaxel in first-line mCRPC. The second is KLK2-comPAS, a randomized, placebo-controlled phase 3 study of pasritamig + best standard of care in late-line mCRPC:
In 2026 and beyond, there are also many treatment options for mHSPC. The following treatments have established a survival and/or progression-free survival improvement:
- ADT + docetaxel
- ADT + abiraterone + prednisone
- ADT + androgen receptor pathway inhibitor: enzalutamide, apalutamide, darolutamide
- ADT + docetaxel + abiraterone + prednisone or darolutamide or enzalutamide
- ADT + abiraterone + prednisone + niraparib (AMPLITUDE trial2) (US FDA approved in December 2025 for BRCA2-mutated mHSPC)
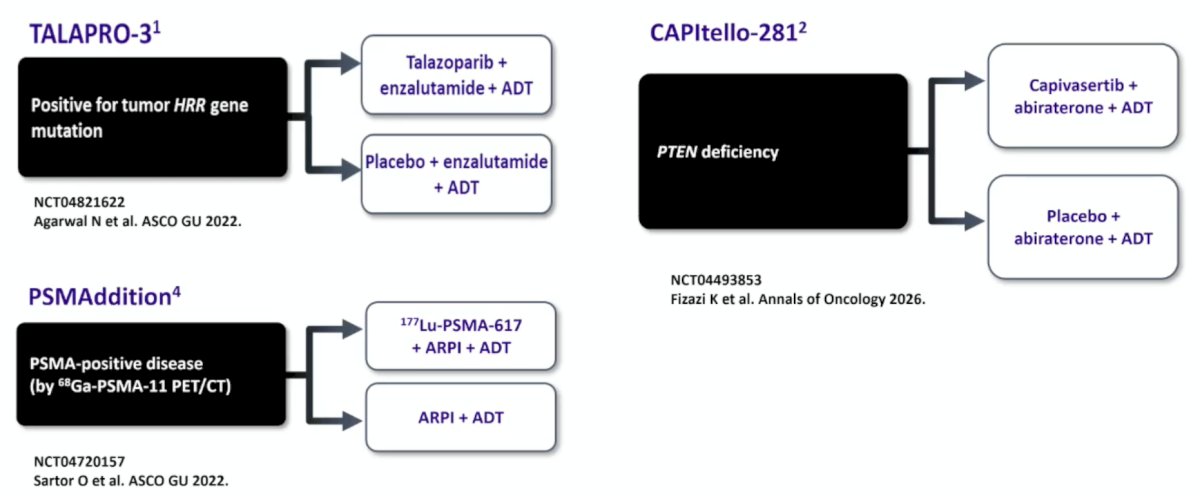
In mHSPC, there are 3 ongoing biomarker-based phase 3 trials: TALAPRO-3, PSMAddition, and CAPItello-281:
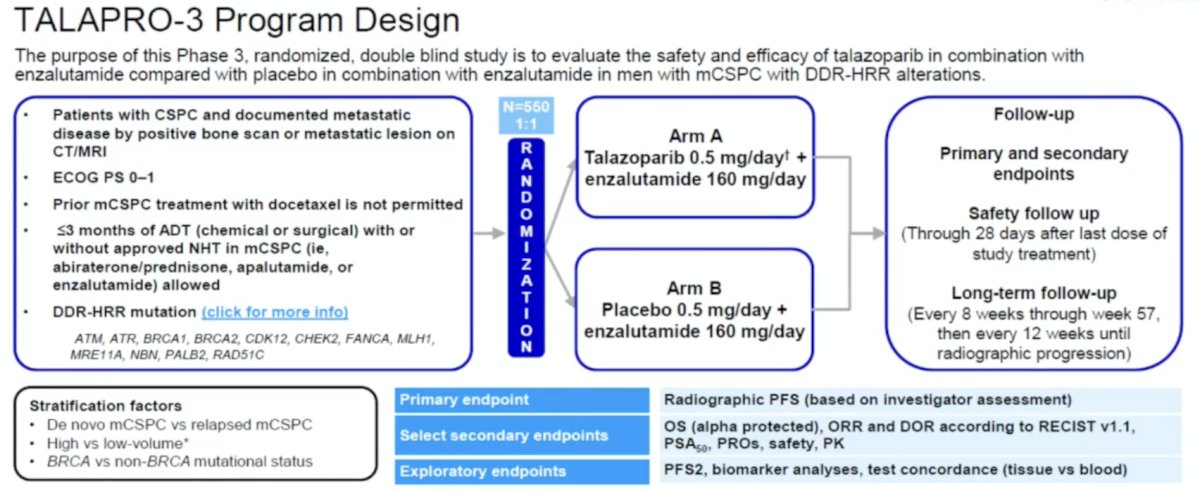
TALAPRO-3 previously reported improved radiographic progression-free survival in HRR mutation patients, with overall survival data pending:
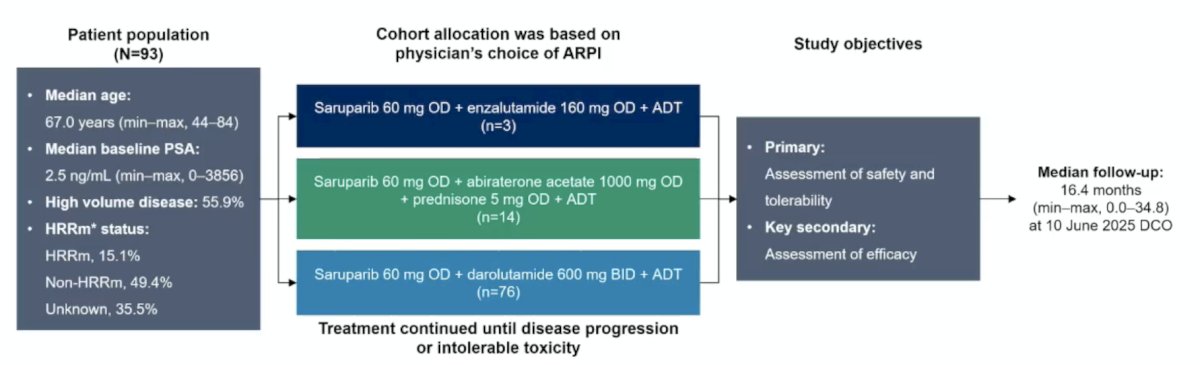
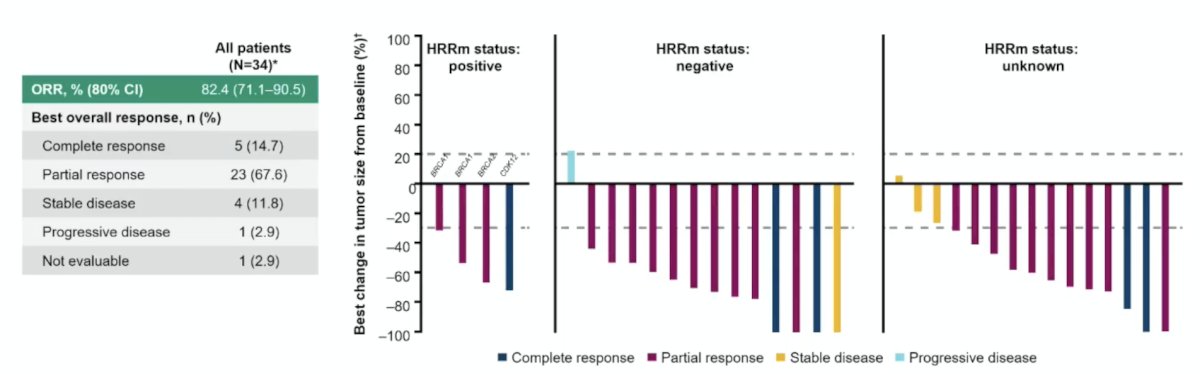
Saruparib is a selective PARP1 inhibitor, and interim results from PETRANHA previously demonstrated high rates of undetectable PSA in mHSPC regardless of HRR mutation status. The current analysis provides updated efficacy and safety data. In this study, patients received oral saruparib 60 mg once daily combined with the physician’s choice of ARPI (enzalutamide, abiraterone acetate, or darolutamide) plus ADT. Up to six months of prior ADT was permitted. Prior chemotherapy for metastatic prostate cancer was not allowed. The study design is shown below.
Among response-evaluable patients (34 of 93), the objective response rate (ORR) was 82.4%, including 14.7% complete responses. The confirmed undetectable PSA rate at any time was 69.9%, and the confirmed 52-week undetectable PSA rate was 76.7%:
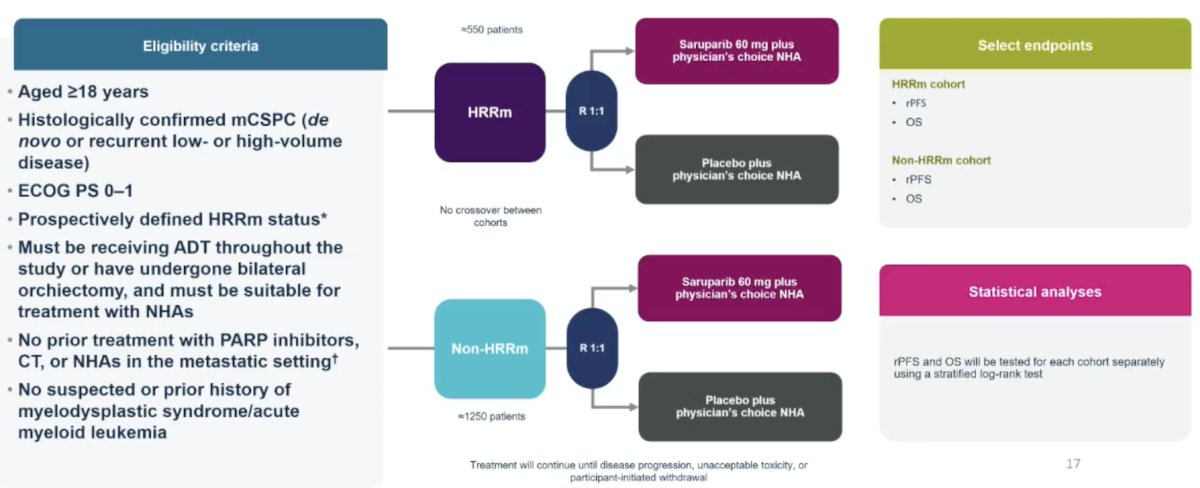
Finally, EvoPAR-Prostate01 is a phase 3 trial, 2-cohort, 2-arm, randomized, double-blind, placebo-controlled, multicenter global study. Key eligibility criteria include (i) age ≥18 years, (ii) histologically confirmed mHSPC (de novo or recurrent low- or high-volume disease), (iii) ECOG PS 0-1, and (iv) confirmed, prospectively defined HRR gene mutation status (defined by the presence/absence of pathogenic/likely pathogenic mutations in ≥1 of the genes BRCA1, BRCA2, ATM, CDK12, PALB2, RAD51B, RAD51C, RAD51D, and BARD1). Participants must be receiving ADT throughout the study or have undergone bilateral orchiectomy, and must be suitable for treatment with androgen receptor pathway inhibitors. Participants are allocated to either the HRR mutation or non-HRR mutation cohort based on prospective testing of both tumor tissue and circulating tumor DNA. Participants are randomized 1:1 to receive saruparib plus the physician’s choice of androgen receptor pathway inhibitor or placebo plus the physician’s choice of androgen receptor pathway inhibitor:
Dr. Hussain concluded her presentation discussing emerging new therapies and what will likely be available in the next 2 years with the following take-home points:
- There has been tremendous progress in managing mHSPC and mCRPC with significant improvement in overall survival over the past 20 + years:
- Overall survival: mHSPC 2.5 versus 5 + years; mCRPC 9 months versus 3 + years
- Metastatic prostate cancer continues to be a complex “smart cancer” with marked inter- and intra-patient heterogeneity. Therapy development must focus on:
- Totality of disease biology: Comprehensive molecular understanding of disease states, mechanisms of resistance, and progression
- Multi-targeted therapy approaches: aiming at “cytotoxic impact.”
- Moving effective therapy to earlier disease states has a better “return on investment”, however, the question is: How will this impact response to the same in-class agents in the mCRPC? What are the resistance mechanisms?
- Well-designed research and clinical trials are needed to address focused questions regarding the evolving biology of metastatic prostate cancer, mechanisms of progression, and optimal therapy sequencing
Presented by: Maha Hussain, MD, FACP, FASCO, Genevieve Teuton Professor of Medicine, Division of Hematology Oncology, Department of Medicine, Deputy Director, Robert H. Lurie Comprehensive Cancer Center, Northwestern University, Feinberg School of Medicine, Chicago, IL
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 Advanced Prostate Cancer Consensus Conference (APCCC), Lugano, Switzerland, Thurs, April 30 – Sat, May 2, 2026.
Related content: AR Degraders, T-Cell Engagers, and EZH2 Inhibitors in Prostate Cancer Pipeline - Maha Hussain
- Rathkopf DE, Patel MR, Choudhury AD, et al. Safety and clinical activity of BMS-986365 (CC-94676), a dual androgen receptor ligand-directed degraded and antagonist, in heavily pretreated patients with metastatic castration-resistant prostate cancer. Ann Oncol. 2025 Jan;36(1):76-88.
- Attard G, Agarwal N, Graff JN, et al. Niraparib and abiraterone acetate plus prednisone for HRR-deficient metastatic castration-sensitive prostate cancer: A randomized phase 3 trial. Nat Med. 2025 Dec;31(12):4109-4118.