(UroToday.com) The 2026 Advanced Prostate Cancer Consensus Conference (APCCC) meeting featured a management of metastatic CRCP (mCRPC) session and a presentation by Dr. Elena Castro discussing which patients we should use an androgen receptor pathway inhibitor + PARP inhibitor. There are three key phase III androgen receptor pathway inhibitor + PARP inhibitor trials in the first line mCRPC setting: MAGNITUDE,1 TALAPRO-2,2 and PROpel.3
MAGNITUDE is a phase III, randomized, double-blind, placebo-controlled, multicenter trial that evaluated the combination of niraparib + abiraterone acetate + prednisone in mCRPC patients receiving first line treatment. Patients with a gene alteration (ATM, BRCA1/2, BRIP1, CDK12, CHEK2, FANCA, HDAC2, or PALB2) detected by ≥1 assay were assigned to the HRR+ cohort, whereas those with both assays negative were included in the HRR- cohort. Patients in the HRR+ and HRR- cohorts underwent 1:1 randomization to receive either reduced-dose niraparib 200 mg once daily (usual dose: 400 mg) and abiraterone acetate 1,000 mg once daily plus prednisone 5 mg twice daily or placebo + abiraterone + prednisone. Given the lower likelihood of clinical benefit with combination treatment in the HRR- cohort, a futility analysis was preplanned when approximately 200 patients had been enrolled, and approximately 125 composite endpoint events (the first of either PSA progression, radiographic progression, or death) had occurred. For the HRR+ cohort, primary and secondary endpoints were tested using a pre-specified strategy. The primary radiographic progression free survival endpoint was powered for and tested first in the BRCA1/2 subgroup, and if statistical significance was reached, the remainder of the HRR+ patients would be analyzed. Approximately 50% of HRR+ patients were specified to be BRCA1/2 positive. The trial design for MAGNITUDE is as follows:
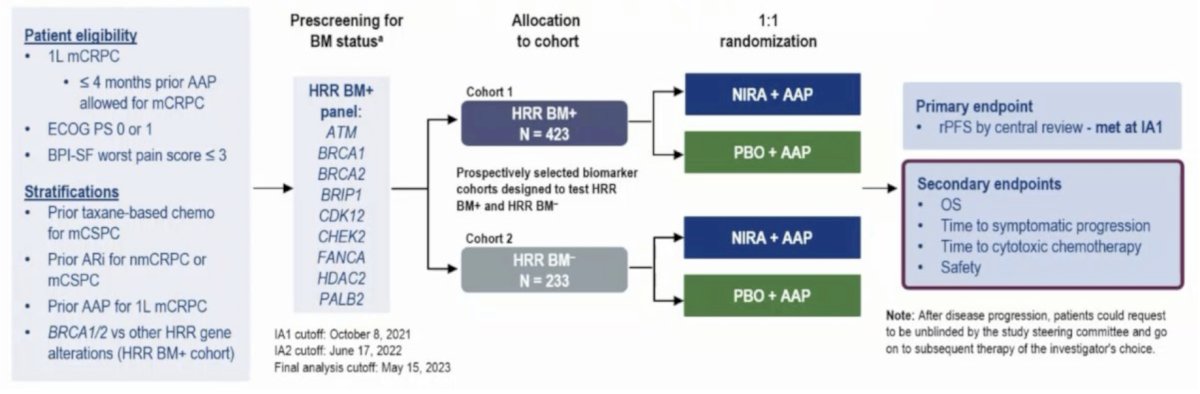
Results of the futility analysis in the HRR- cohort (n = 233) demonstrated no benefit for combination niraparib + abiraterone versus placebo + abiraterone.
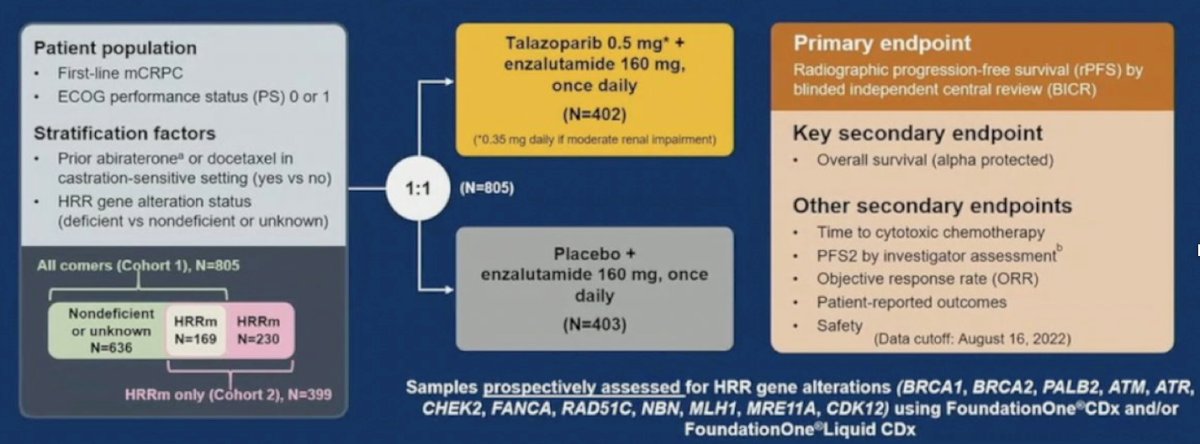
TALAPRO-2 is a phase III randomized, double-blind, placebo-controlled trial that randomized mCRPC patients 1:1 to talazoparib 0.5 mg once daily (reduced dose from standard of 1 mg) plus enzalutamide 160 mg once daily versus placebo + enzalutamide. Prior use of docetaxel and abiraterone in the mHSPC, but not in the mCRPC setting, was permitted. No prior use of an androgen receptor pathway inhibitor was permitted. This was a biomarker unselected cohort of ‘all comers’. The primary endpoint was radiographic progression free survival, assessed via blinded independent central review, and overall was a key secondary endpoint. The trial design for TALAPRO-2 is as follows:
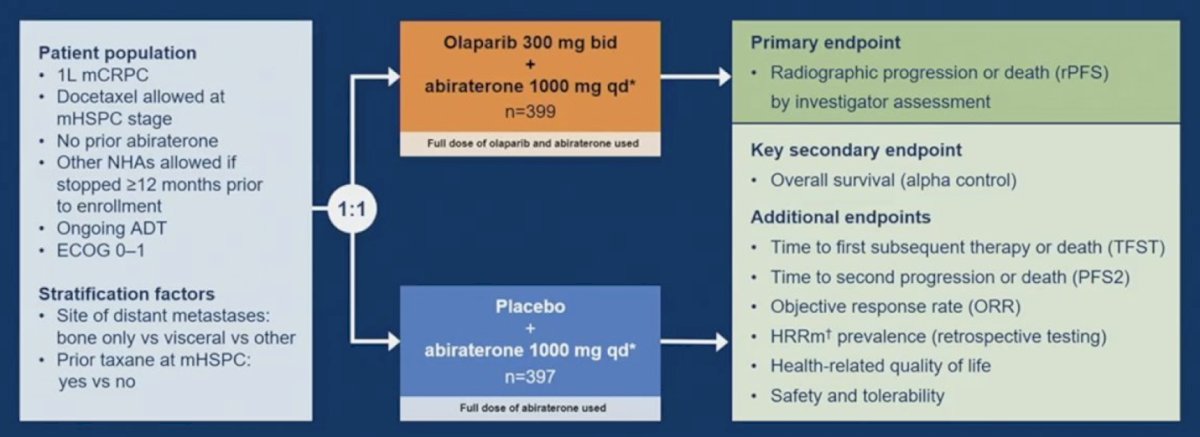
PROpel is a global, randomized, double-blind phase 3 trial of abiraterone and olaparib versus abiraterone and placebo in patients with mCRPC treated in the first-line setting. Patients in PROpel were enrolled irrespective of HRR mutational status, which was ascertained via ctDNA or tissue testing. Patients were randomized 1:1 to receive abiraterone (1,000 mg once daily) plus prednisone/prednisolone with either full dose olaparib (300 mg twice daily) or placebo. Prior abiraterone use was not permitted, but other androgen receptor pathway inhibitor use was permitted if discontinued ≥12 months prior to study enrollment. The primary endpoint was imaging-based progression-free survival, by investigator assessment. The trial design for PROpel is as follows:
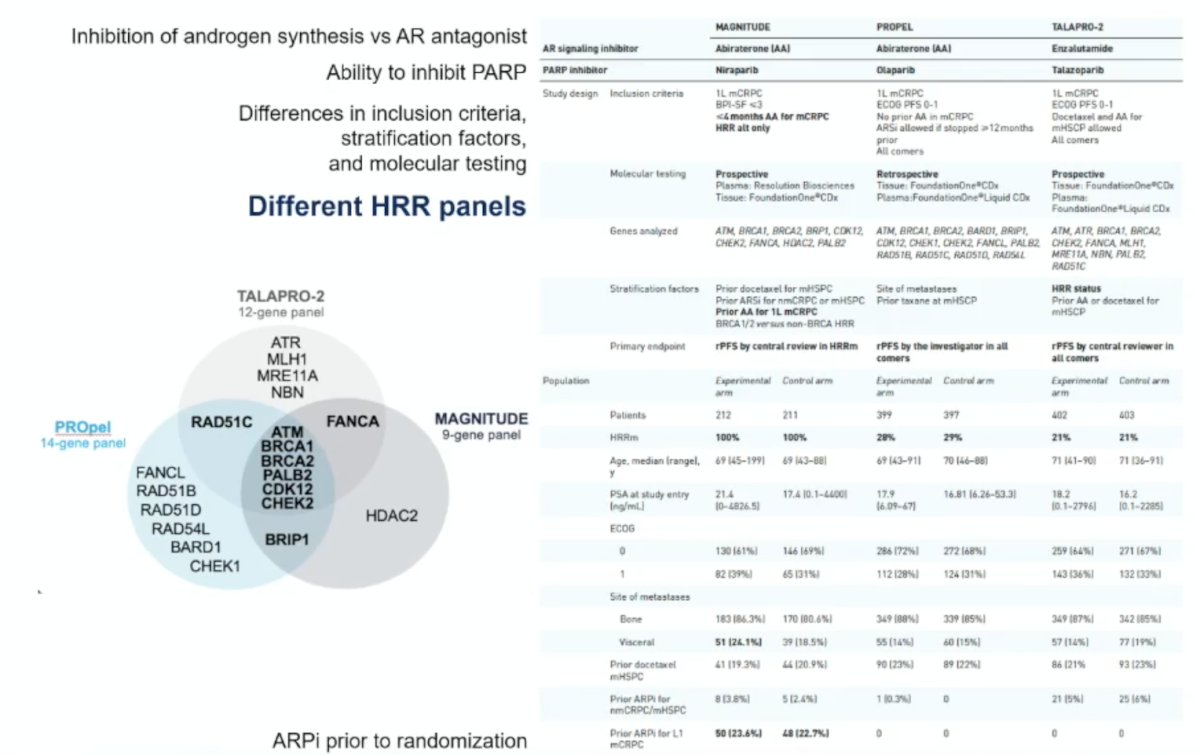
The following table summarizes key aspects of the three trials:
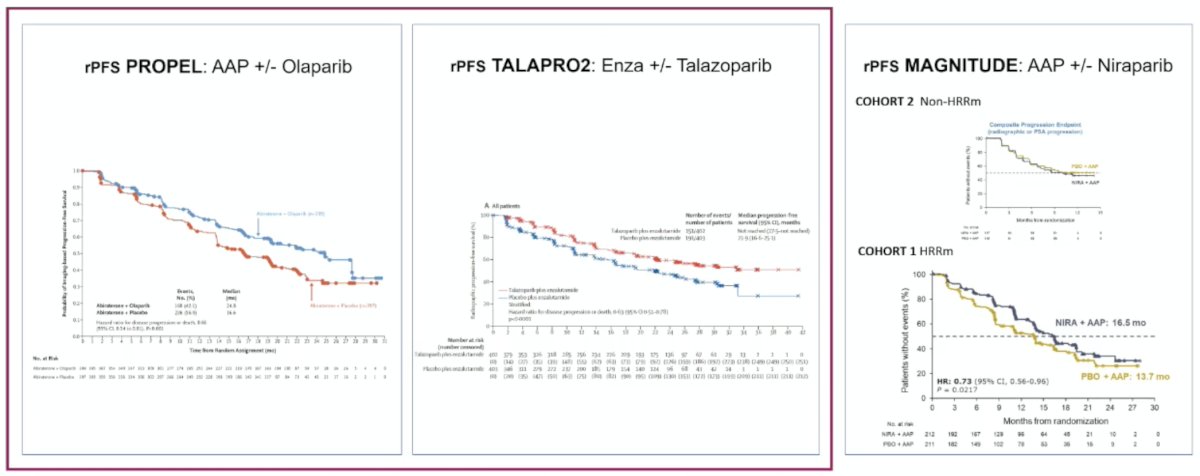
The following figure demonstrates the radiographic progression free survival benefit reported in patients unselected for HRR alterations across the 3 trials:
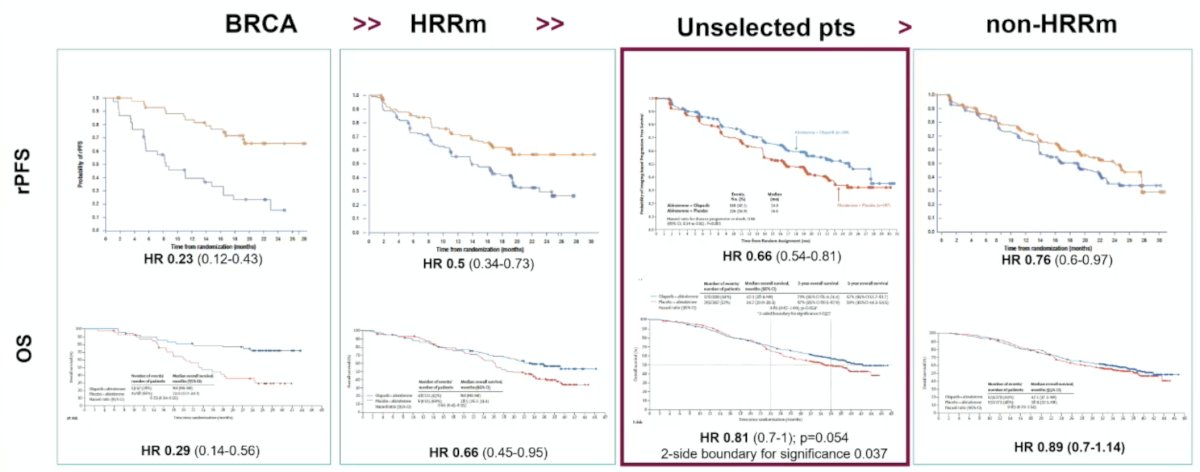
The PROpel trial demonstrated the hierarchical benefit aligned appropriately with biology:
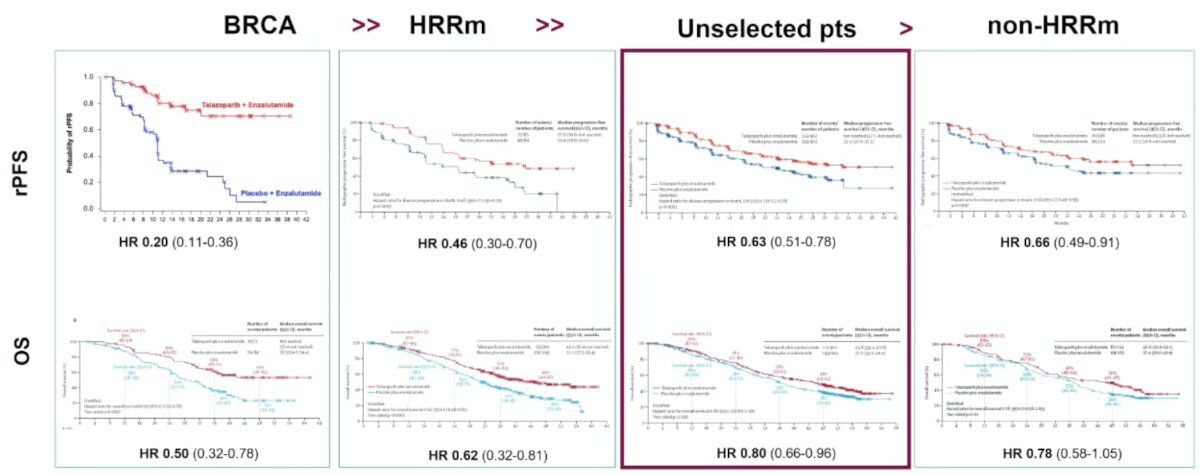
This hierarchical benefit was also observed in the TALAPRO-2 trial:
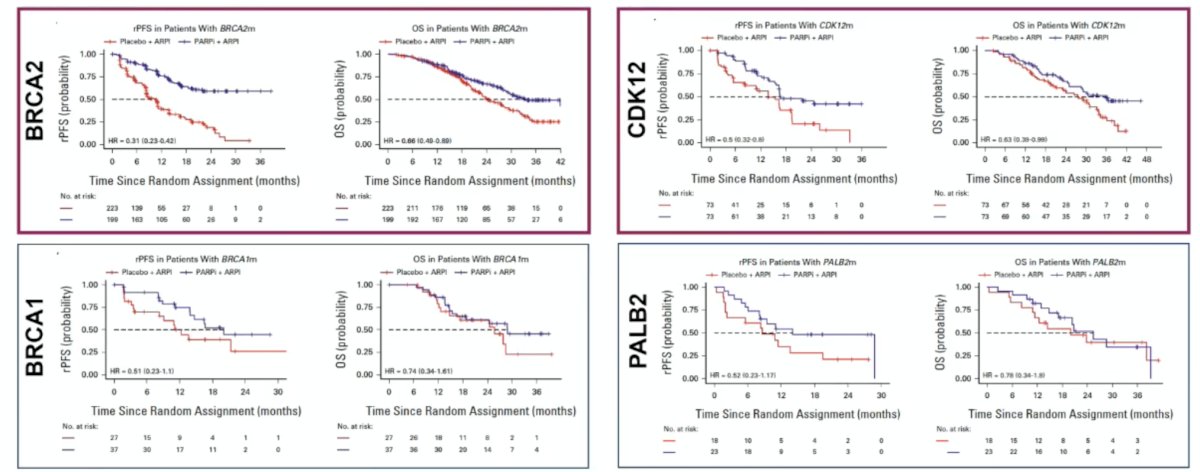
Dr. Castro then discussed an FDA pooled analysis from 2024 that assessed the impact of PARP inhibitors on patients with non-BRCA HRR alterations,4 noting that the benefit from PARP inhibitors appeared greatest for patients with BRCA1, BRCA2, CDK12, and PALB2 mutations:
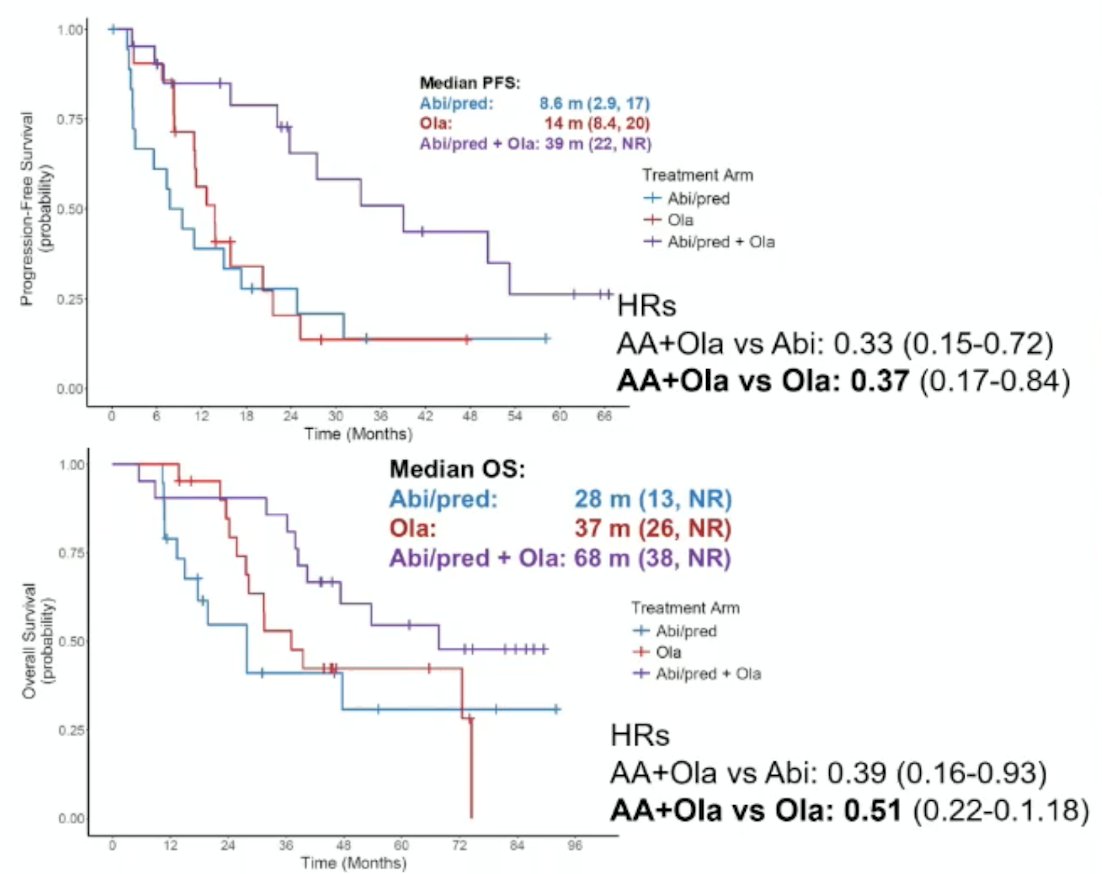
Dr. Castro also discussed the BRCAAway trial,5 which was a multi-center, open-label, randomized, phase 2 trial. Eligible patients had progressive mCRPC with HRR mutations and no prior exposure to PARP inhibitors or abiraterone. Patients with HRR mutations in BRCA1/2 and/or ATM alterations were randomized 1:1:1 to:
- Arm 1: abiraterone 1000 mg QD + prednisone 5 mg BID (abiraterone + prednisone)
- Arm 2: olaparib 300 mg BID (olaparib)
- Arm 3: abiraterone/prednisone + olaparib (abiraterone + prednisone + olaparib)
With regards to progression free survival, the hazard ratio for abiraterone + prednisone + olaparib versus abiraterone + prednisone was 0.33 (95% CI 0.15-0.72) and for abiraterone + prednisone + olaparib versus olaparib was 0.37 (95% CI 0.17-0.84). Over a median follow-up of 46.2 months, Arm 3 had the longest median overall survival of 68 months (95% CI: 38–not reached), compared to Arm 1 median of 28 months (95% CI: 13– not reached), with a HR of 0.39 (95% CI 0.16–0.93), and compared to Arm 2 median of 37 months (95% CI 26– not reached), with a HR of 0.51 (95% CI 0.22–1.18):
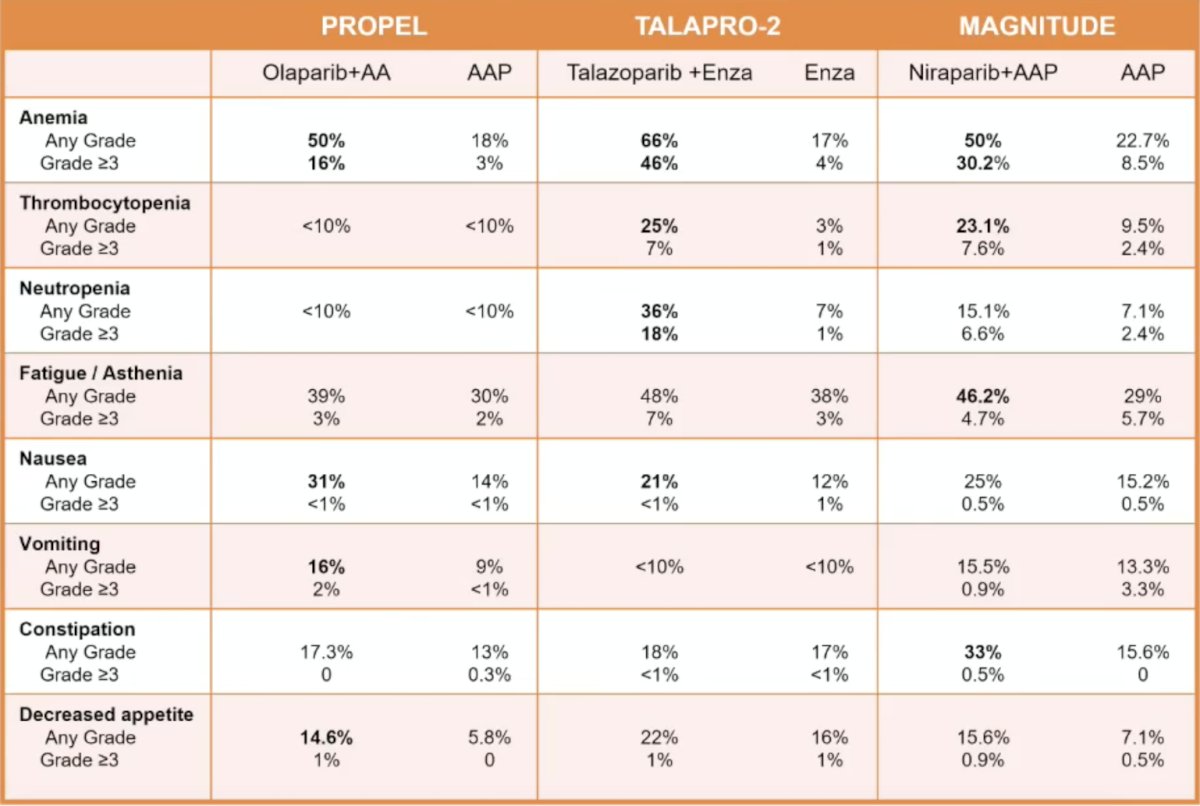
There were no differences in toxicity by HRR status, with the following table highlighting the increased toxicity with androgen receptor pathway inhibitor + PARP inhibitor versus androgen receptor pathway inhibitor:
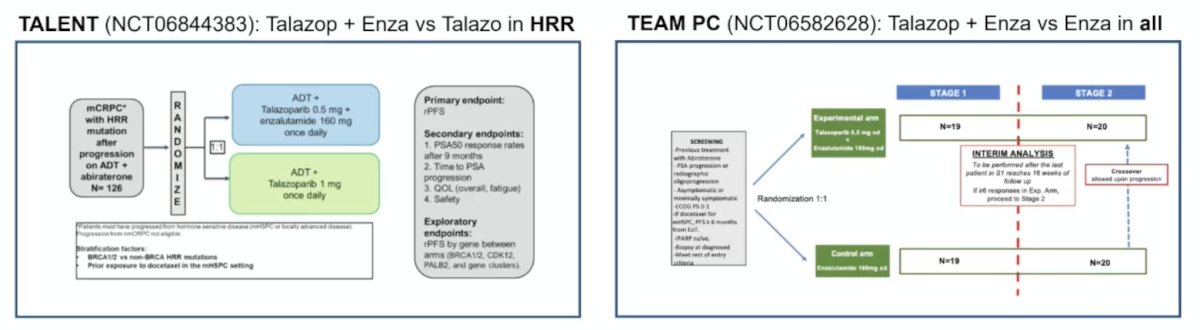
In situations of androgen receptor pathway inhibitor + PARP inhibitor after progression on an androgen receptor pathway inhibitor, there are two trials in this disease space:
- TALENT: talazoparib + enzalutamide versus talazoparib in HRR mutation patients
- TEAM PC: talazoparib + enzalutamide versus enzalutamide in all patients
The following figure illustrates androgen receptor pathway inhibitor + PARP inhibitor approvals stratified by country and mutation status:

Dr. Castro concluded her presentation discussing which patients we should use an androgen receptor pathway inhibitor + PARP inhibitor summarizing these patients stratified by each mutation:
- BRCA 1/2:
- Consistent radiographic progression free survival (and overall survival) benefit from androgen receptor pathway inhibitor + PARP inhibitor as first line mCRPC
- Strong evidence for BRCA2, limited evidence for BRCA1 due to low prevalence
- In androgen receptor pathway inhibitor naïve, androgen receptor pathway inhibitor + PARP inhibitor combination is likely superior to PARP inhibitor monotherapy
- Unknown benefit of androgen receptor pathway inhibitor + PARP inhibitor after progression on androgen receptor pathway inhibitor
- PARP inhibitor (+/- androgen receptor pathway inhibitor) are the only therapy that have improved outcomes in this subgroup of patients
- PALB2: The benefit is likely similar to BRCA, but there is limited evidence due to low prevalence
- CDK12:
- Likely to benefit from androgen receptor pathway inhibitor + PARP inhibitor in mCRPC
- Unknown benefit of androgen receptor pathway inhibitor + PARP inhibitor after progression on androgen receptor pathway inhibitor
- ATM, CHEK2:
- Unlikely to benefit from androgen receptor pathway inhibitor + PARP inhibitor in mCRPC
- Other therapies may be prioritized
- No HRR alterations:
- Androgen receptor pathway inhibitor + PARP inhibitor: radiographic progression free survival benefit, no overall survival benefit in mCRPC
- Unknown benefit of androgen receptor pathway inhibitor + PARP inhibitor after progression on androgen receptor pathway inhibitor
- Other therapies may be prioritized and these patients should be evaluated on a case by case basis
Presented by: Elena Castro, MD, PhD, Hospital Universitario 12 de Octubre, Madrid, Spain
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 Advanced Prostate Cancer Consensus Conference (APCCC), Lugano, Switzerland, Thurs, April 30 – Sat, May 2, 2026.
References:
- Chi KN, Rathkopf D, Smith MR, et al. Niraparib and abiraterone acetate for metastatic castration-resistant prostate cancer. J Clin Oncol. 2023 Jun 20;41(18):3339-3351.
- Agarwal N, Azad AA, Carles J, et al. Talazoparib plus enzalutamide in men with first-line metastatic castration-resistant prostate cancer (TALAPRO-2): A randomized, placebo-controlled, phase 3 trial. Lancet. 2023 Jul 22;402(10398):291-303.
- Saad F, Clarke NW, Oya M, et al. Olaparib plus abiraterone versus placebo plus abiraterone in metastatic castration-resistant prostate cancer (PROpel): final prespecified overall survival results of a randomized, double-blind, phase 3 trial. Lancet Oncol. 2023 Oct;24(10):1094-1108.
- Fallah J, Xu J, Weinstock C, et al. Efficacy of Poly(ADP-ribose) Polymerase Inhibitors by Individual Genes in Homologous Recombination Repair Gene-Mutated Metastatic Castration-Resistant Prostate Cancer: A US Food and Drug Administration Pooled Analysis. J Clin Oncol. 2024 May 10;42(14):1687-1698.
- Hussain M, Kocherginsky M, Agarwal N, et al. Abiraterone, olaparib, or abiraterone + olaparib in first-line metastatic castration-resistant prostate cancer with DNA repair defects (BRCAAway). Clin Cancer Res. 2024 Oct 1;30(19):4318-4328.