(UroToday.com) The 2026 Advanced Prostate Cancer Consensus Conference (APCCC) meeting featured a management of metastatic hormone-sensitive prostate cancer (mHSPC) session and a presentation by Dr. Mika Matikainen discussing updates on de-escalation treatment strategies.
The rationale for de-escalation in HSPC is that modern HSPC management has shifted toward treatment intensification (ADT + androgen receptor pathway inhibitor ± docetaxel), improving overall survival but at the cost of cumulative toxicity (cardiovascular risk, fractures, fatigue, and cognitive effects). De-escalation aims to:
- Reduce long-term toxicity of androgen suppression (morbidity & mortality)
- Improve quality of life
- Potentially delay castration resistance (evolutionary pressure hypothesis)
- Personalize therapy based on depth of response (ie, PSA nadir)
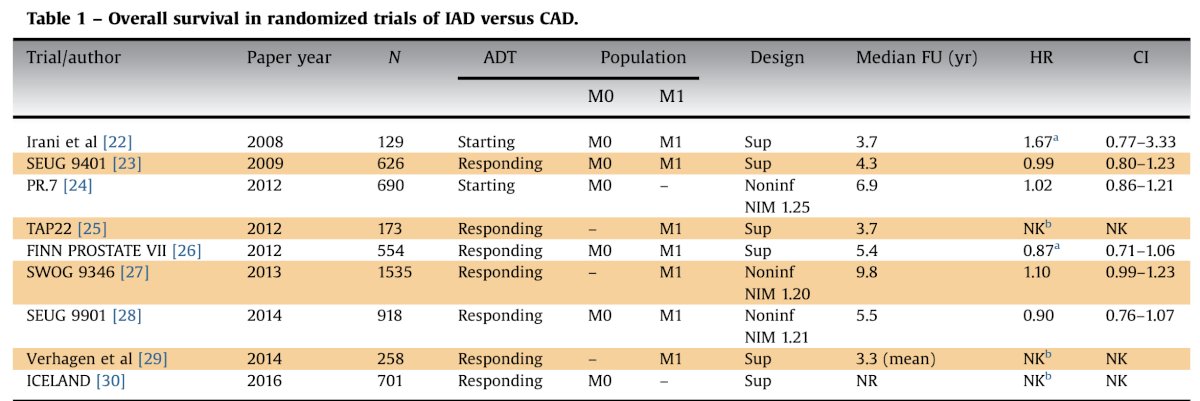
The following table summarizes the randomized studies comparing intermittent ADT versus continuous ADT (before the androgen receptor pathway inhibitor era), highlighting that intermittent ADT has not conclusively demonstrated an impact on disease progression or survival. The hazard ratios in metastatic disease indicate less favorable survival with intermittent ADT in M1 disease:1
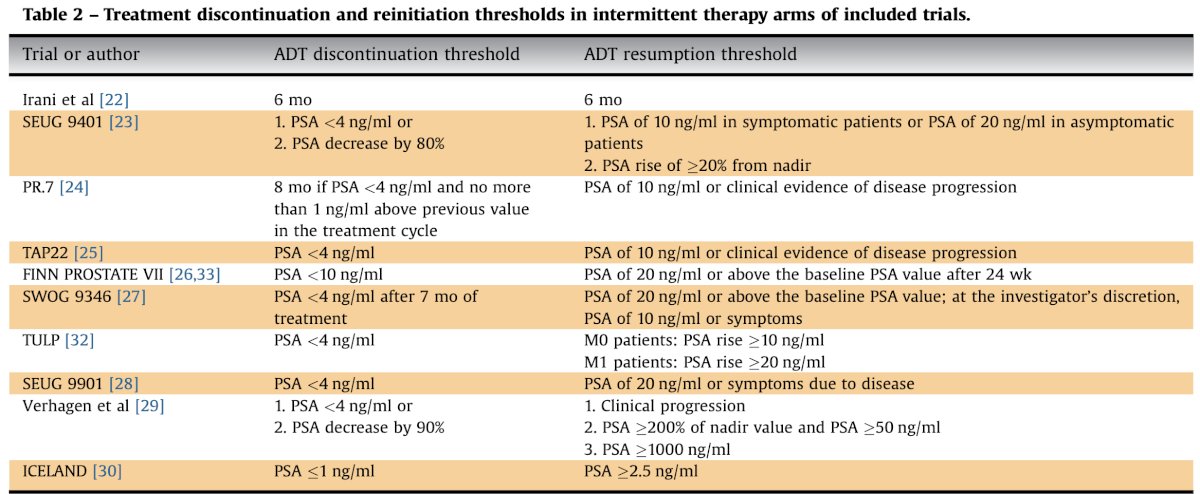
Additionally, the following table emphasizes treatment discontinuation and re-initiation thresholds in intermittent therapy arms in these trials:
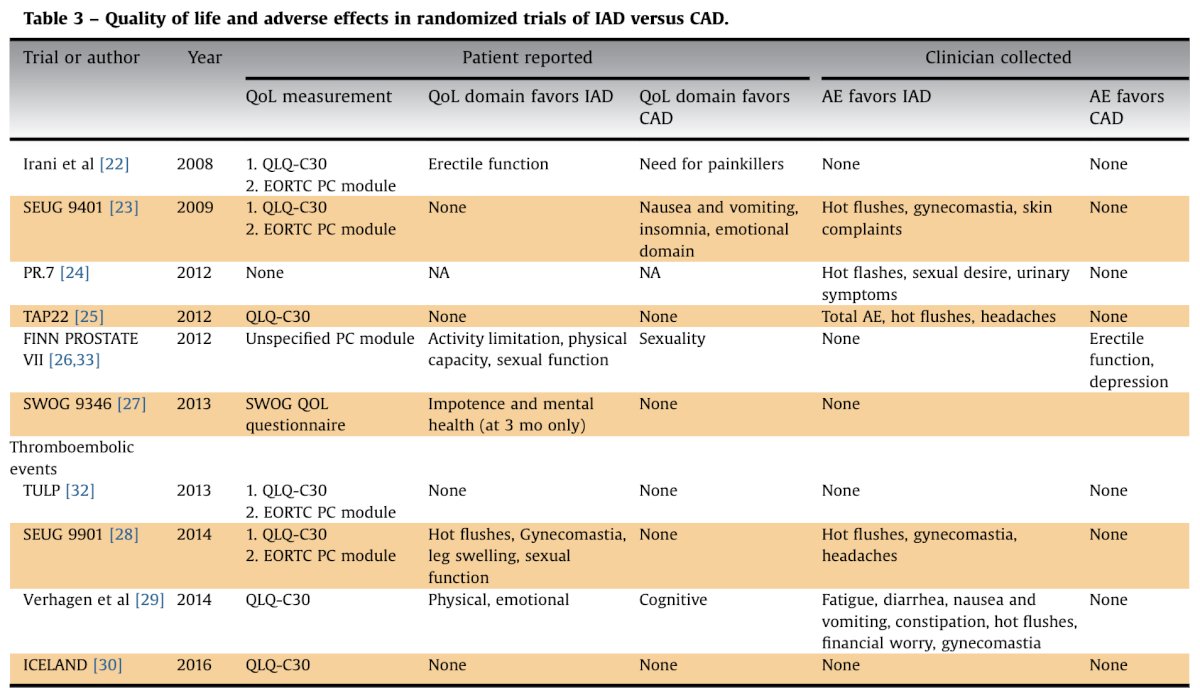
Taken together, there is a modest but temporary quality of life and symptom benefit generally favoring intermittent ADT:
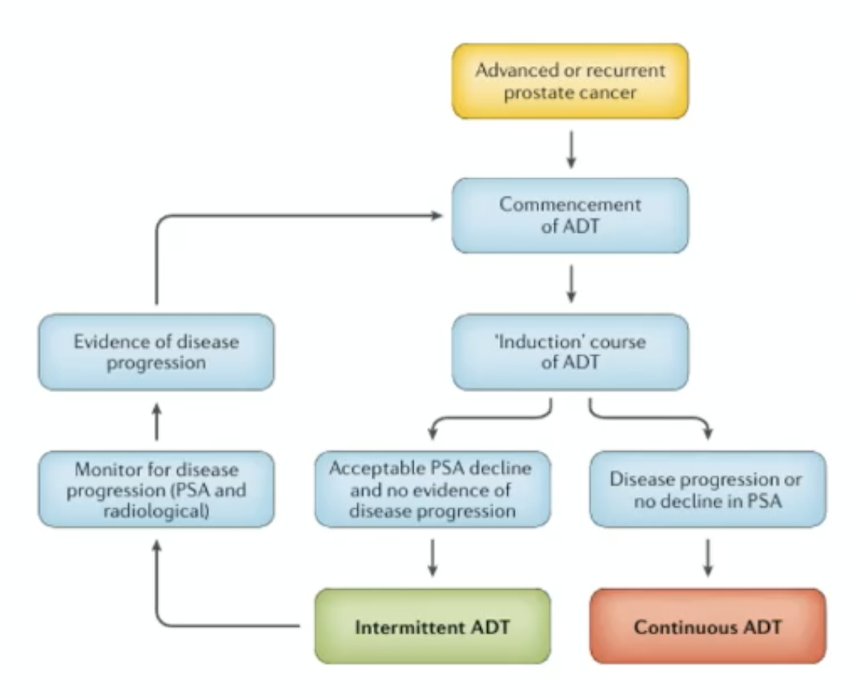
The historical evidence for intermittent ADT is that the classic strategy included cycles of ADT with off-treatment intervals. Based on this historical data, there was no clear overall survival inferiority versus continuous ADT, but with improved quality of life endpoints, and the largest study being SWOG 9346 in mHSPC. The clinical interpretation has been that acceptable patients are those who are highly selected, especially those with lower disease burden and good PSA response. However, intermittent ADT is still controversial in high-volume or aggressive disease. Key limitations of this historical data are that the trials pre-date androgen receptor pathway inhibitors (modern standard), and it is unclear about the applicability is unclear in the intensified therapy era.
Modern de-escalation concepts include response-adapted therapy, including PSA-based thresholds increasingly used to guide treatment interruption, continuation versus intensification modalities, and PSA remains the most validated biomarker for de-escalation decisions. For androgen receptor pathway inhibitor de-escalation, there are emerging strategies including:
- Androgen receptor pathway inhibitor interruption after deep PSA response
- Androgen receptor pathway inhibitor monotherapy (avoid ADT toxicity)
- Adaptive therapy approaches (experimental)
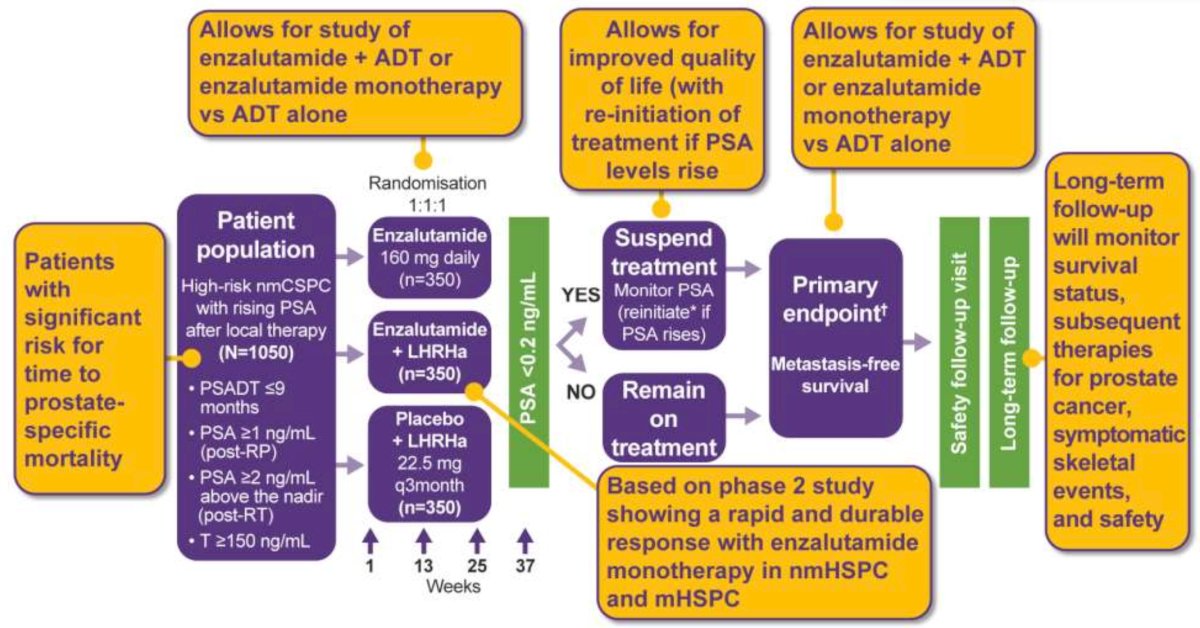
In the high-risk biochemical recurrence/non-metastatic HSPC disease space, EMBARK2 was a phase 3 trial that enrolled patients with a PSA ≥1 ng/ml after radical prostatectomy or ≥2 ng/ml above nadir after primary external beam radiotherapy, with a PSA doubling time of ≤9 months. Patients had no evidence of metastasis on conventional imaging, and baseline testosterone was ≥150 ng/dL. Hormone therapy ≥9 months prior to enrolment was permitted. Patients underwent stratified randomization (by PSA level, PSA doubling time, and prior hormonal therapy receipt) to one of three arms:
- Enzalutamide 160 mg (standard dose) + leuprolide (blinded arm)
- Placebo + leuprolide (blinded)
- Enzalutamide monotherapy (unblinded)
PSA was assessed at 36 weeks, and if patients had a PSA < 0.2 ng/mL, treatment was suspended at week 37, and PSA was monitored with treatment reinitiated if PSA increased again. If patients had a PSA > 0.2 ng/mL, treatment was continued. The primary endpoint was metastasis-free survival, assessed via blinded independent central review, in the enzalutamide + leuprolide versus leuprolide arms only. Key secondary endpoints included overall survival and safety outcomes. The trial design for EMBARK is as follows:
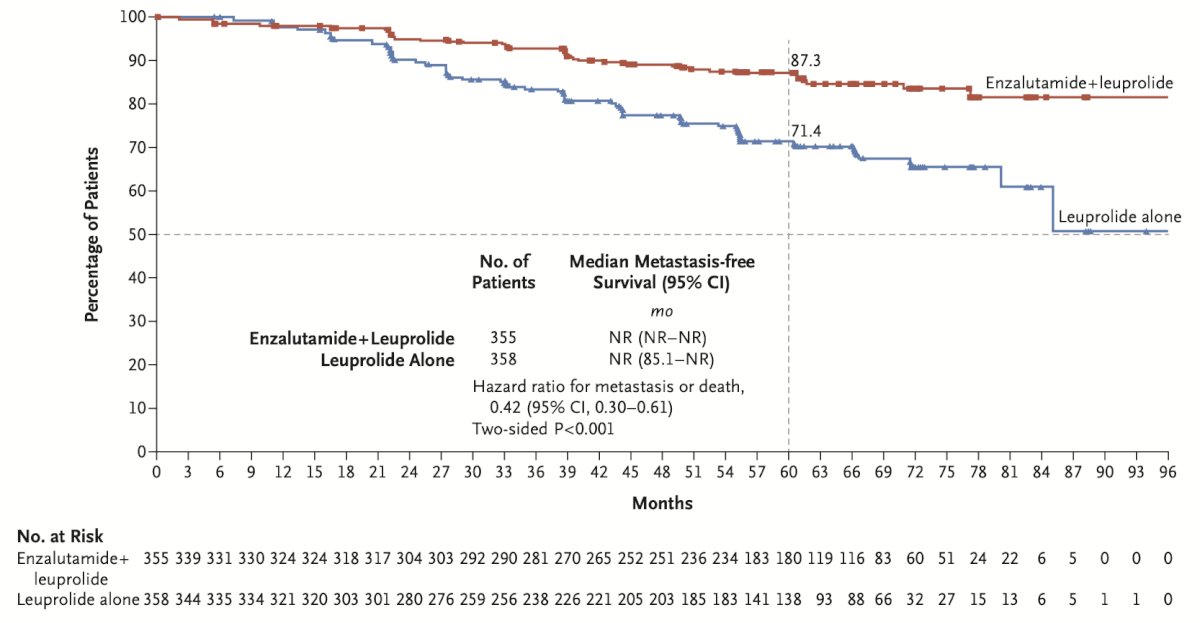
At a median follow-up of 5 years, the combination of enzalutamide + leuprolide versus leuprolide alone demonstrated a significant improvement in metastasis-free survival (HR 0.42, 95% CI 0.31 – 0.61, p < 0.0001). The median metastasis-free survival was not reached in either arm to date:
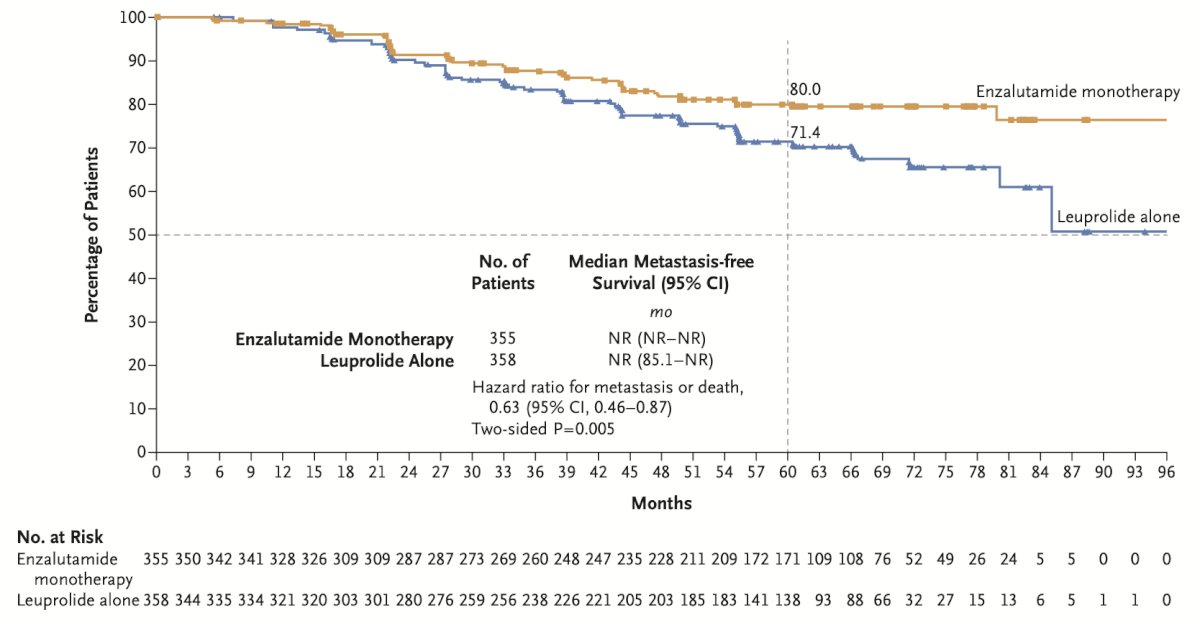
Comparisons between the enzalutamide monotherapy and leuprolide monotherapy arms were also performed. This demonstrated prolonged metastasis-free survival in the enzalutamide-only arm, with a HR of 0.63 (95% CI 0.46 – 0.87, p = 0.0049):
The following points highlight the treatment suspension and outcomes in the EMBARK trial:
- Combination group: 90.9% of patients had treatment suspended for a median of 18.0 months, with 37.4% not requiring retreatment for over 24 months
- Leuprolide-alone group: 67.8% of patients had treatment suspended for a median of 16.6 months, with 27.9% not requiring retreatment for over 24 months
- Monotherapy group: 85.9% of patients had treatment suspended for a median of 9.4 months, with 14.8% not requiring retreatment for over 24 months
- There was no substantial difference in the time to decline in FACT-P total scores in the combination group and the monotherapy group, as compared with the leuprolide-alone group, which indicates that adverse events did not affect the overall quality of life
In an EMBARK post-hoc analysis assessing the impact of treatment suspension on health-related quality of life, Freedland et al. [3] found that improved metastasis-free survival was achieved without negatively affecting global health-related quality of life during treatment or after treatment suspension, with a gradual improvement in hormonal treatment-related symptoms after treatment suspension:
![In an EMBARK post-hoc analysis assessing the impact of treatment suspension on health-related quality of life, Freedland et al. [3] found that improved metastasis-free survival was achieved without negatively affecting global health-related quality of life during treatment or after treatment suspension, with a gradual improvement in hormonal treatment-related symptoms after treatment suspension:](/images/com-doc-importer/262-apccc-2026/apccc-2026-update-on-de-escalation-strategies-in-mhspc-in-which-patients-and-when-can-we-stop-the-treatment/image-7.jpg)
Dr. Matikainen provided the following summary points for the EMBARK trial:
- There was an improvement in metastasis-free survival: combination 87.3% versus 71.4% ADT alone
- Enzalutamide monotherapy was also superior to ADT
- There was no major quality of life detriment despite intensification
- This is the first phase III evidence supporting: (i) intermittent, PSA adapted systemic therapy; (ii) therapy “holidays” with androgen receptor pathway inhibitor-based regimens
- This established the paradigm: treat, suppress PSA, stop, restart
With regards to mHSPC, the current status is that standard of care is continuous intensified therapy (ADT + androgen receptor pathway inhibitor +/- docetaxel); thus, de-escalation is not standard of care, but is being actively investigated. Evidence suggests that intermittent ADT has no overall survival difference, but may have a slight inferiority signal in high-volume disease. Currently, there is a strong interest in de-escalation for low-volume/oligometastatic disease and among those who are deep PSA responders. Ongoing and recent clinical trials in mHSPC include:
- Intermittent/response-guided strategies
- Adaptive/biomarker-driven de-escalation
- EMBARK-related paradigm expansion
The following table highlights ADT and androgen receptor pathway inhibitor-sparing approaches in ongoing and recent mHSPC studies:
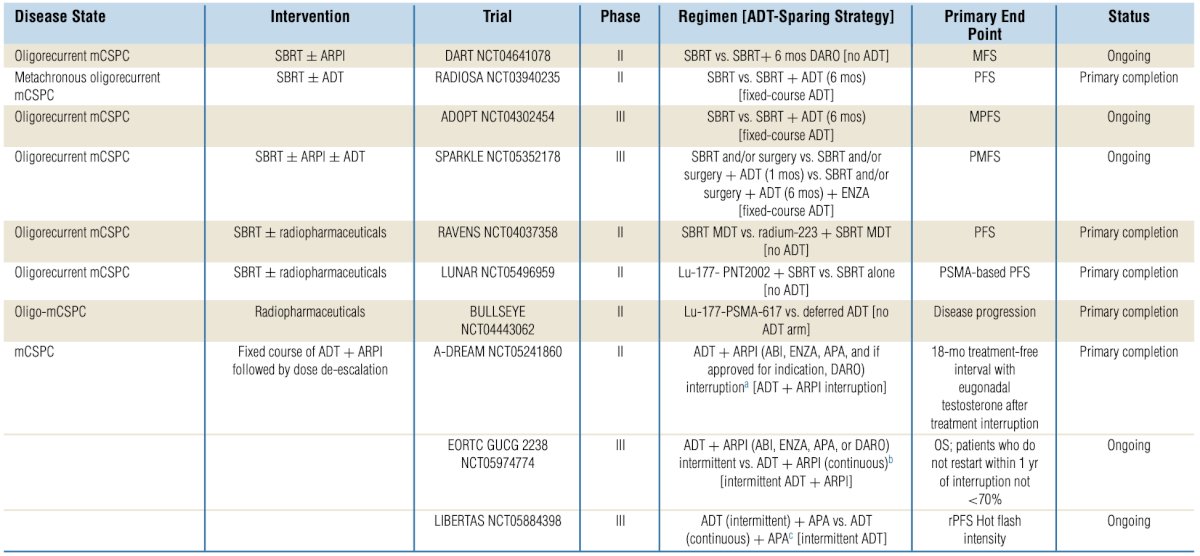
The following figure shows the ADT and androgen receptor pathway inhibitor dose de-escalation approaches in ongoing mHSPC studies:4
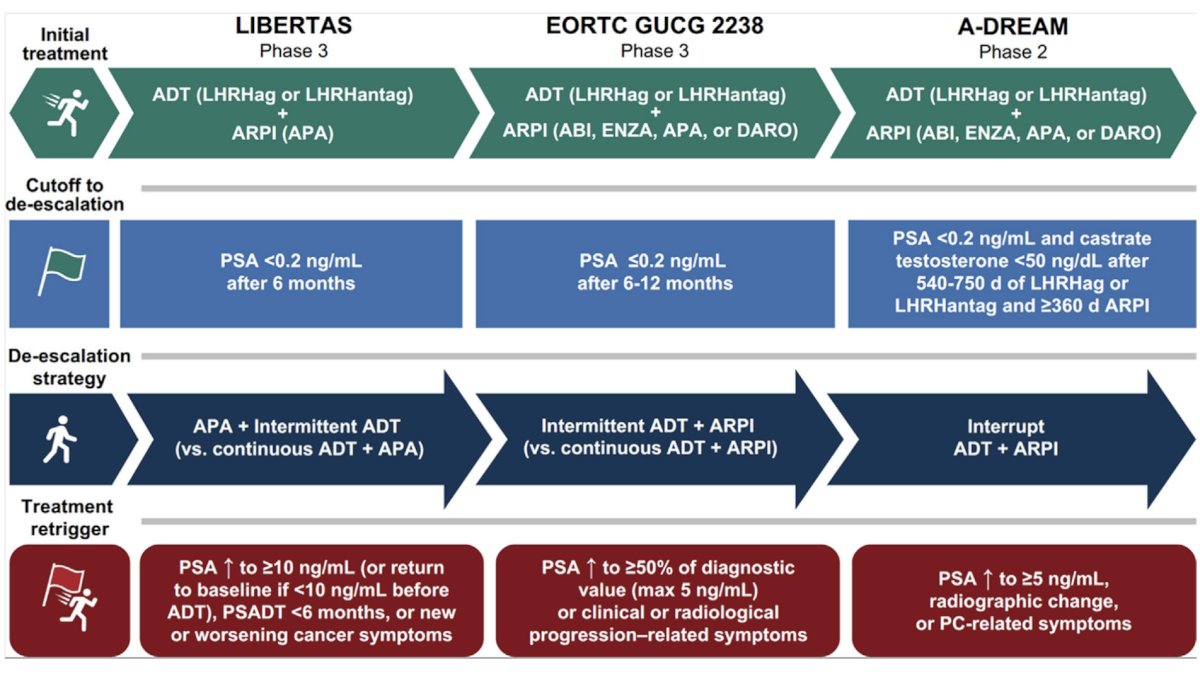
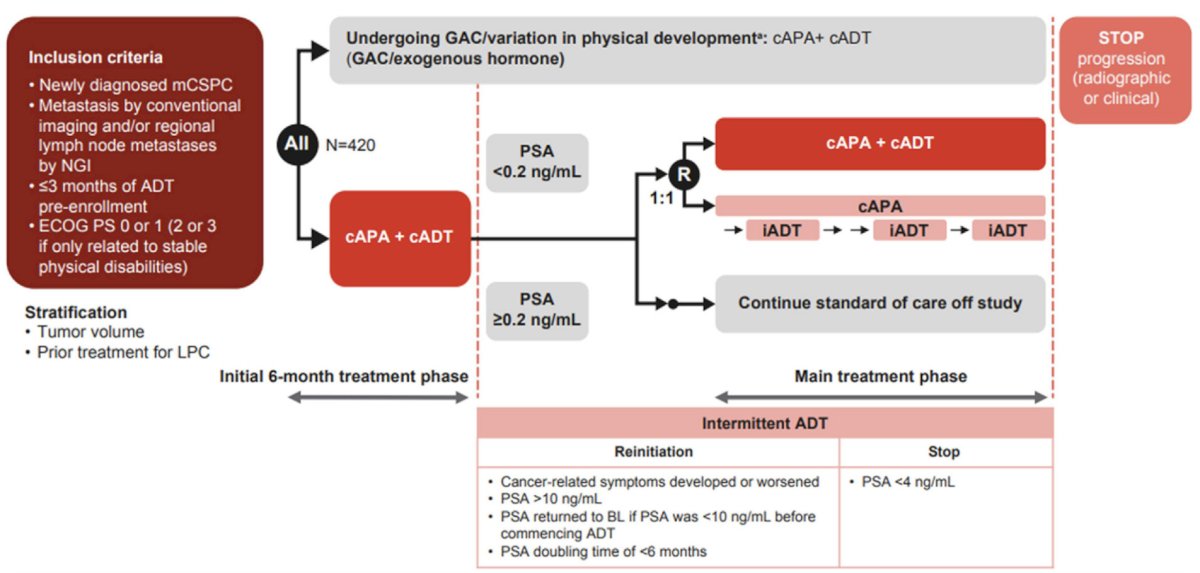
LIBERTAS is a prospective, open-label, randomized study, enrolling patients with mHSPC. Patients had metastasis by conventional imaging and/or regional lymph node metastases by next-generation imaging, ≤3 months of ADT pre-enrolment, and ECOG performance status 0 or 1 (2 or 3 if only related to stable physical disabilities). Patients received 6 months of apalutamide (240 mg/d) + continuous ADT, and patients with confirmed PSA <0.2 ng/mL were randomized 1:1 to apalutamide + intermittent ADT or apalutamide + continuous ADT in the main treatment phase:
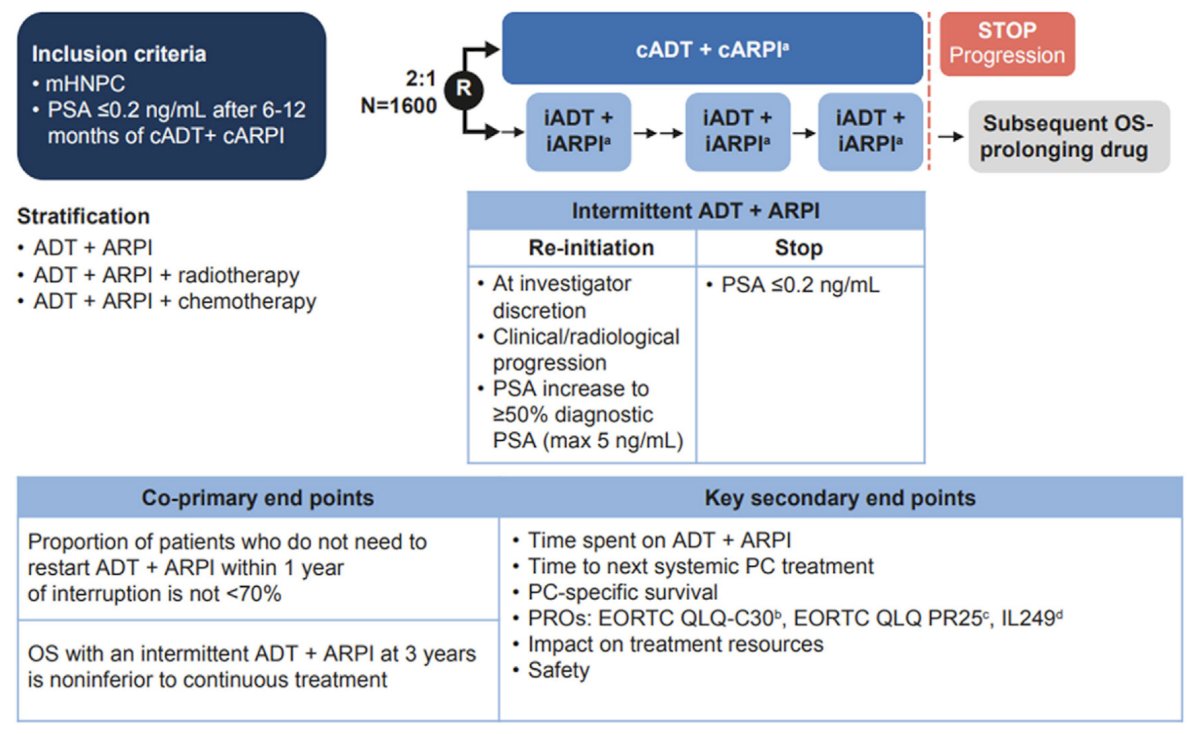
The EORTC GUCC 2238 trial is an academic-led, open-label, pragmatic, randomized phase III study to investigate whether intermittent androgen blockade can be safely administered to mHSPC patients who reached a PSA ≤ 0.2 ng/mL at 6 to 12 months of continuous maximal androgen blockade, as compared to continuing maximal androgen blockade. The co-primary endpoints are:
- The proportion of patients who do not need to restart their maximal androgen blockade within one year of interruption is not less than 70%, and
- Overall survival using an intermittent androgen blockade regimen at three years is non-inferior to continuous treatment
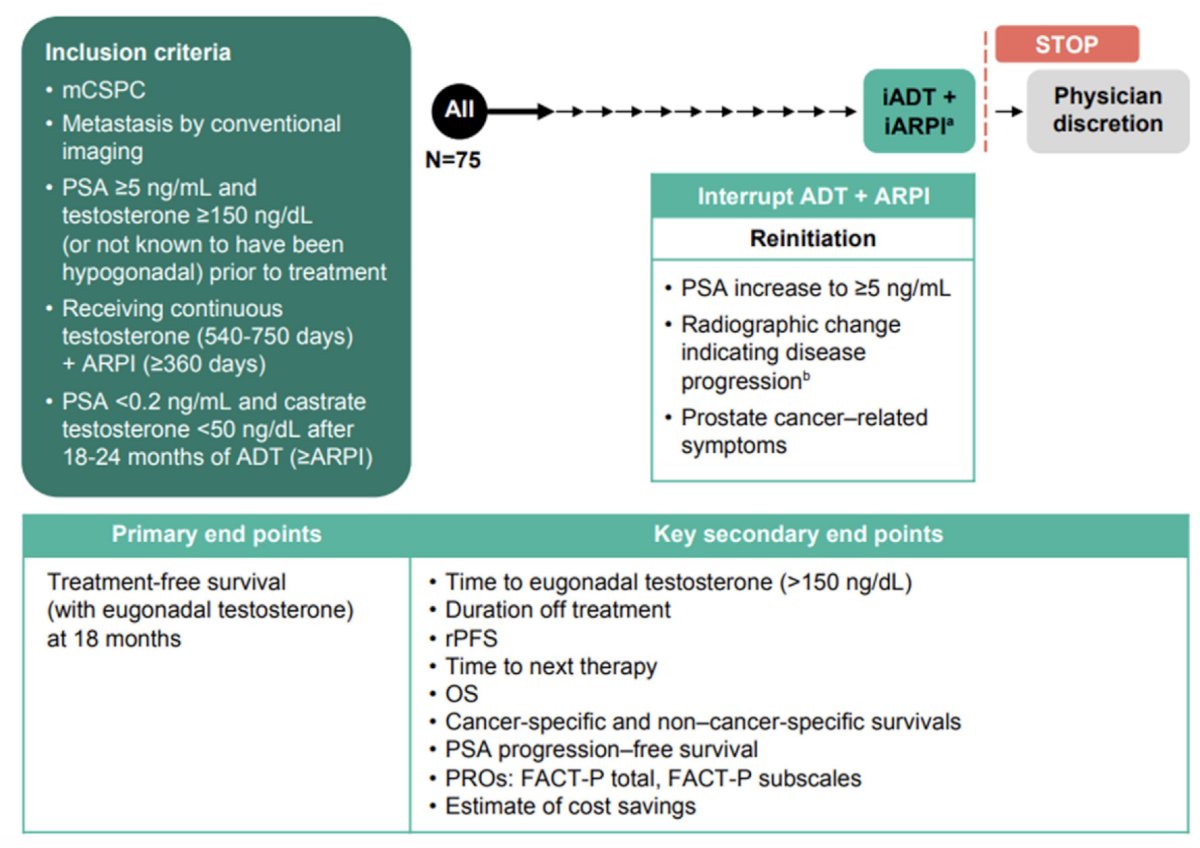
A-DREAM is a single-arm phase II trial of mHSPC patients receiving ADT + androgen receptor pathway inhibitor who achieve a serum PSA level <0.2 ng/ml (stable/decreasing) following 18–24 months of ADT and ≥12 months of an androgen receptor pathway inhibitor. Patients will have both ADT and androgen receptor pathway inhibitor discontinued and will have PSA and testosterone levels re-evaluated every three months, with scans and quality of life assessments performed every 6 months (every 3 months if PSA is rising). Triggers for treatment re-initiation include the occurrence of either:
- PSA ≥5 ng/ml
- Radiographic changes
- Prostate cancer-related symptoms
The primary study outcome is 18-month eugonadal treatment-free survival:
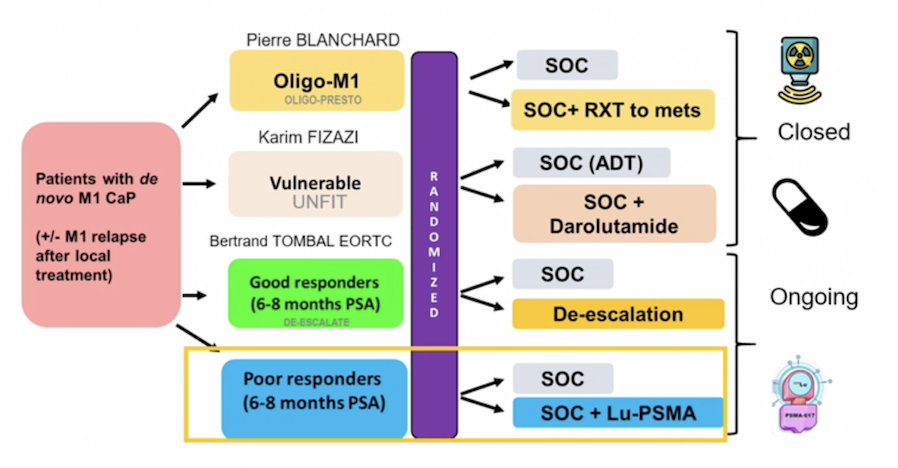
PEACE-6 is an important adaptive/biomarker-driven de-escalation trial among patients with oligometastatic disease. The purpose of PEACE 6 in de novo mHSPC is to search for the best treatment strategy for these patients. Patients with oligometastatic disease will be randomized to standard of care versus standard of care + radiotherapy to the metastatic lesions. Unfit, vulnerable patients will be randomized to standard of care (ADT) versus standard of care + darolutamide. Good responders (after 6-8 months of PSA response) will be randomized to standard of care versus de-escalation approaches. Finally, poor responders (after 6-8 months of poor PSA response) will be randomized to standard of care versus standard of care + Lu-PSMA therapy:
Generally, potential candidates for stopping (de-escalating) treatment include:
- Exceptional responders: responders achieving an undetectable PSA level at 6-7 months exhibit a more favorable prognosis compared to those with elevated PSA levels
- Patient factors: individuals experiencing treatment-related toxicity and elderly individuals with life-limiting comorbidities
- Disease factors: metachronous low-volume disease, lower Gleason score, and longer PSA doubling time
Currently, there are several unresolved questions regarding de-escalation strategies, and there is a need for studies:
- What is the optimal PSA threshold for stopping/restarting therapy?
- What is the role of PSMA PET in defining disease burden?
- Can an androgen receptor pathway inhibitor monotherapy replace ADT in the long term?
- What is the impact on time to castration resistance and overall survival in mHSPC?
- What are biomarkers beyond PSA (genomic, ctDNA)?
Dr. Matikainen concluded his presentation discussing updates on de-escalation treatment strategies with the following take-home points:
- Intermittent ADT remains a valid option in selected patients with a quality of life benefit and comparable survival in older trials
- EMBARK introduces a modern de-escalation model: androgen receptor pathway inhibitor-based therapy, and PSA guided treatment suspension
- De-escalation is transitioning from empirical intermittent ADT to a biomarker-driven model (PSA thresholds, other biomarkers)
- There are multiple ongoing trials testing:
- Androgen receptor pathway inhibitor interruption
- Response-adapted therapy
- Personalized intensification/de-intensification
Presented by: Mika P. Matikainen, DMedSc, Helsinki University Hospital, Helsinki, Finland
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 Advanced Prostate Cancer Consensus Conference (APCCC), Lugano, Switzerland, Thurs, April 30 – Sat, May 2, 2026.
References:- Shevach J, Sydes MR, Hussain M. Revisiting intermittent therapy in metastatic prostate cancer: Can less be more in the “New World Order”? Eur Urol Focus. 2019 Mar;5(2):125-133.
- Freedland SJ, de Almeida Luz M, De Giorgi U, et al. Improved Outcomes with Enzalutamide in Biochemically Recurrent Prostate Cancer. N Engl J Med 2023 Oct 19;389(16):1453-1465.
- Freedland SJ, De Giorgi U, Rannikko A, et al. Impact of treatment suspension on health-related quality of life in the EMBARK trial: A post hoc analysis. EClinicalMedicine. 2025 Aug 14:87:103429.
- Morgans AK, Sentana-Lledo D, Wildgust M, et al. Advances in androgen deprivation therapy-sparing strategies: Ongoing studies in metastatic castration-sensitive prostate cancer. Clin Genitourin Cancer. 2026 Mar 9;102536.