(UroToday.com) The 2026 Advanced Prostate Cancer Consensus Conference (APCCC) meeting featured a management of metastatic hormone sensitive prostate cancer (mHSPC) session and a presentation by Dr. Maria De Santis discussing practical recommendations for nutrition in patients starting on long term systemic therapies. There are several challenges for patients when starting long term ADT, including an overwhelming stream of often conflicting or unclear recommendations in view of a paucity of high level evidence. Also, there is a potential financial burden of supplements, alternative approaches, and specialized diets that may or may not offer real benefit. Thus, the goals of this presentation are to:
- Provide an overview of evidence and guideline recommendations
- Provide practical advice
The reason this topic matters is that ADT causes increased fat mass, increased metabolic risk (diabetes mellitus, cardiovascular disease), decreased muscle mass (sarcopenia), and decreased insulin resistance. Nutrition is part of standard oncology care, with the goal of maintaining nutritional status in order to preserve muscle mass, improve treatment tolerance and quality of life, and focus not just on weight but also on body composition.
In terms of nutritional screening and assessment, weight and BMI alone can be misleading. Body composition predicts outcomes better than weight, as not all weight gain or weight loss is healthy. Even overweight patients can be malnourished. Dr. De Santis notes that we should screen regularly for weight change, BMI, intake history, functional status, and consider body composition tools. In order to keep an energy balance, it is important to avoid overfeeding (fat gain) and underfeeding (muscle loss). There should be a matched food intake to a patient’s activity level and clinical condition, given that energy balance influences outcomes and survivorship.
Protein is central to muscle preservation, supporting muscle mass, recovery, and function. However, nutrition alone is not enough, thus patients must exercise to stimulate muscle anabolism and improve insulin sensitivity. The best combination is protein + resistance exercise, with a recommended protein intake of 0.8-1.2 g/kg. There are important key differences between mean protein and vegetarian protein:
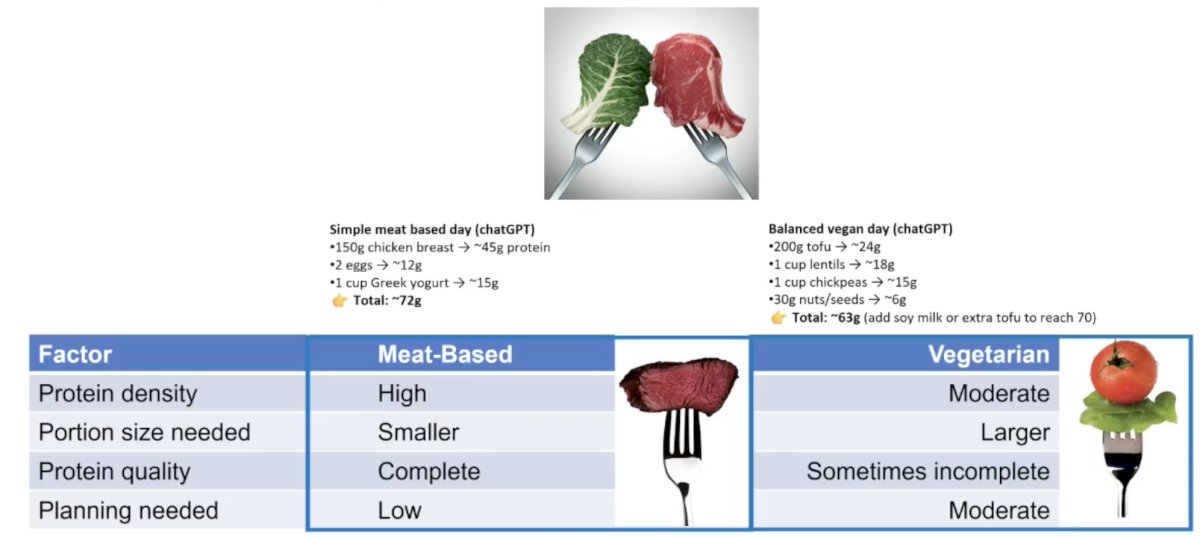
Regarding meat intake, there is no strong proof that eating meat directly worsens prostate cancer in men on ADT. However, diet patterns do influence survival, and ADT makes cardiovascular risk a major driver of outcomes. Limiting red/processed meat is based on risk reduction, not strict cancer causation. Regarding sugar intake, patients should not aim for “zero sugar,” as there is no evidence that complete sugar elimination improves prostate cancer on ADT. However, patients should limit added sugars mainly to protect weight, glucose control, lipids, and cardiovascular health while on ADT.
There are several common patient nutritional questions and answers for men on ADT, as highlighted in the following table:1

Regarding diets and fasting, Dr. De Santis states that patients should avoid unproven “anti cancer diets” and extreme diets. What may be reasonable is a ketogenic diet, low-carbohydrate diet, fasting, and intermittent/interval fasting. The following table provides an overview of the evidence and guidelines for ketogenic/low carbohydrate diets and prostate cancer patients on ADT:

In 2022, Umlauff et al.2 performed a meta-analysis of 11 studies (n = 536) to summarize the available evidence on the effects of dietary interventions on lean mass, fat mass, and BMI in men treated with ADT for prostate cancer. Dietary advice and supplementation interventions combined were not associated with significant changes in lean mass (0.05 kg; 95% CI: -0.17, 0.26; p = 0.674), fat mass (-0.22 kg; 95% CI: -0.45, 0.01; p = 0.064), or BMI (-0.16 kg*m-2; 95% CI: -0.37, 0.04; p = 0.121). Dietary advice interventions alone were associated with a significant fat mass reduction (-0.29 kg; 95% CI: -0.54, -0.03; p = 0.028). Future interventions need to investigate whether a combination of dietary advice and protein supplementation with concomitant resistance exercise could counteract ADT-induced muscle wasting.
Intermittent fasting is defined as time restricted eating (5:2; 4:3), which has been an effective modality for weight loss, and has a similar effect overall to calorie restriction. What does it mean?
- 5:2 fasting: 5 normal days + 2 fasting days
- 4:3 fasting: more aggressive than 5:2, but still flexible
- 16:8 fasting: eat within an 8 hour window daily
A 2025 systematic review and network meta-analysis (not prostate cancer specific) assessed whether intermittent fasting is effective, and whether it is better than a usual caloric restriction or ad-libitum diet.3 There were 99 randomized controlled trials (n= > 6,500) on intermittent fasting diets and continuous energy restriction versus ad-libitum diets, with the metric of cardio-metabolic outcomes. This analysis found that all intermittent fasting strategies and continuous energy restriction diets showed a reduction in body weight compared with an ad-libitum diet. Further, alternate day fasting showed benefit in body weight reduction compared with continuous energy restriction.
A 2026 Cochrane systematic review assessed intermittent fasting (16:8, 5:2, alternate-day) versus continuous dieting (not prostate cancer specific). There were 22 randomized controlled trials (n = ~2,000), and weight loss was the selected metric. This analysis found that intermittent fasting was comparable to continuous dieting, with both modalities leading to a decrease of ~3% body weight, with no meaningful difference. Ultimately, total calorie intake matters most.
Dr. De Santis provided the following summary points regarding diets in prostate cancer patients on hormonal treatment:
- Supported: low carbohydrate approaches can help manage ADT side effects
- Uncertain: ketogenic diets for prostate cancer patients on ADT
- Caution: risk of muscle loss, adherence issues, and nutritional imbalance if unsupervised
Dr. De Santis noted that there are now tools and apps to support patients on ADT, with ADT-specific lifestyle education platforms. The goal is to help patients build sustainable diet + exercise habits, and to support long-term weight and metabolic health.
Dr. De Santis concluded her presentation discussing practical recommendations for nutrition in patients starting on long term systemic therapies with the following take-home points:
- Nutrition in ADT is not just weight control
- There needs to be a focus on: muscle preservation, metabolic health, compliance and quality of life
- There should be a combination of diet + exercise
- Diets should not be extreme, low carbohydrate diet is preferred, and total caloric intake is what matters, not how it is achieved (consider the addition of protein and resistance exercise)
- Individualized care is essential
Presented by: Maria De Santis, MD, PhD, Charite Universitatsmedizin Berlin, Berlin, Germany
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 Advanced Prostate Cancer Consensus Conference (APCCC), Lugano, Switzerland, Thurs, April 30 – Sat, May 2, 2026.
References:
- Kenfield SA, van Blarigan EL, Graff RE, et al. Nutrition guidance for patients on androgen deprivation therapy. Eur Urol Focus. 2023 May;9(3):427-430.
- Umlauff L, Weber M, Freitag N, et al. Dietary interventions to improve body composition in men treated with androgen deprivation therapy for prostate cancer: A solution for the growing problem? Prostate Cancer Prostatic Dis. 2022 Feb;25(2):149-158.
- Semnani-Azad Z, Khan TA, Chiavaroli L, et al. Intermittent fasting strategies and their effects on body weight and other cardiometabolic risk factors: Systematic review and network meta-analysis of randomized clinical trials. BMJ. 2025 Jun 18:389:e082007.