(UroToday.com) The 2026 Advanced Prostate Cancer Consensus Conference (APCCC) meeting featured a management of metastatic hormone-sensitive prostate cancer (mHSPC) session and a presentation by Dr. Dana Rathkopf discussing the considerations for selection of androgen receptor pathway inhibitors in older patients with mHSPC.
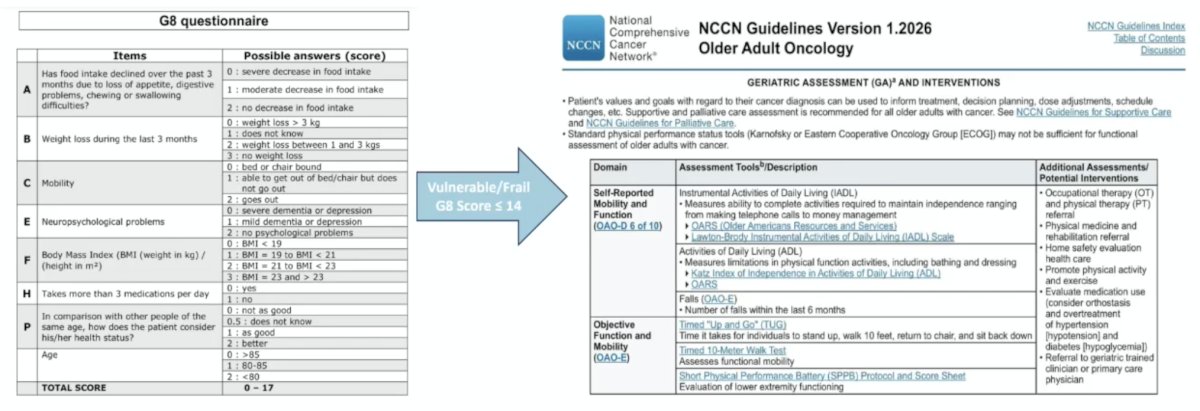
How old is “old”? Dr. Rathkopf states that it is important to consider physiological age more than chronological age, which includes taking into account comorbidities, functional status, cognitive function, and overall frailty. Measuring frailty is important, as across many cancer types it conveys an increased risk of mortality, toxicity, intolerance, and hospitalization. Geriatric assessment-guided management can reduce toxicity without compromising survival in older patients:
In older/frail Veterans with mHSPC receiving ADT +/- androgen receptor pathway inhibitor, a study presented at ASCO GU 2026 showed that ADT + androgen receptor pathway inhibitor was associated with a lower risk of death in the following patients:
- Age >= 75 years: 33.1 versus 22.8 months
- Frailty (VA-FI score): 27.1 versus 19.7 months
- Comorbidities (CCI 3+): 29.0 versus 19.6 months
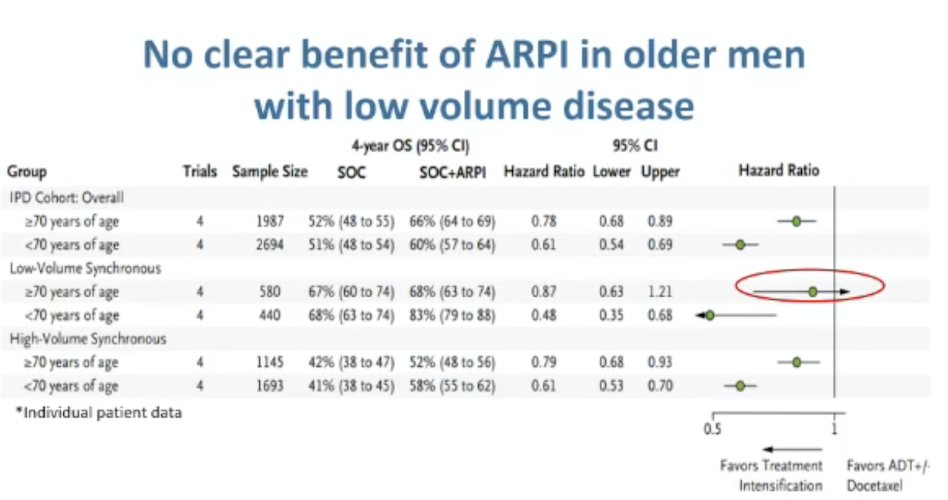
In 2025, Morgans et al.1 performed a systematic review and meta-analysis to assess if age impacts the overall survival benefit from systemic treatment intensification with androgen receptor pathway inhibitors and/or chemotherapy in mHSPC. Among 11 randomized comparisons (n = 13,648), treatment intensification was not associated with improvement in overall survival in older men treated in trials utilizing predominantly triplet therapy (HR 0.94, 95% CI 0.77-1.14). Moreover, an androgen receptor pathway inhibitor addition was associated with improved overall survival in men 70 years or older with high volume synchronous disease (HR 0.83, 95% CI 0.70 to 0.99), but not in low volume synchronous disease (HR 0.89, 95% CI 0.61 to 1.30):
In the PEACE-1 trial,2 a post hoc analysis assessing men >= 70 years of age receiving ADT + docetaxel +/- abiraterone in mHSPC. This analysis showed that older men derived a lower benefit, likely due to more toxicity and earlier drug discontinuation. In the ARASENS trial3 assessing ADT + docetaxel +/- darolutamide in mHSPC, age-specific subgroup analyses demonstrated an increased survival benefit in men 75-84 years of age (HR 0.61 versus HR 0.69 for the total population).
Data from the STOPCAP group was presented by David Fisher at ASCO GU 2025, assessing which patients with mHSPC benefit from androgen receptor pathway inhibitors. There were 11 eligible androgen receptor pathway inhibitor trials, including 11,154 patients, with available data for 7 trials (7,778 patients; 70%). Four trials used androgen biosynthesis inhibitors (4,685 patients; STAMPEDE-Abiraterone, LATITUDE, PEACE-1, SWOG 1216), and 3 trials used “amides” +/- abiraterone (3,093 patients; ENZAMET, TITAN, STAMPEDE-Abiraterone + Enzalutamide). Based on this data, adding an androgen receptor pathway inhibitor to ADT improved overall survival (HR 0.66, 95% CI 0.62-0.71), with a 13% absolute improvement at 5 years. Moreover, there was also a clear benefit for androgen receptor pathway inhibitors, improving progression-free survival (HR 0.51, 95% CI 0.48-0.55), with a 21% absolute improvement at 5 years. Based on 48% “amide” data, there was no clear difference by class of agent. Age was not prognostic: progression-free survival decreased with increasing age (interaction HR 1.15, 95% CI 1.06-1.24), and overall survival effect also decreased with increasing age (interaction HR 1.11, 95% CI 1.01-1.21). There are several key takeaway messages from this study:
- There is a clear benefit of androgen receptor pathway inhibitors on overall survival and progression-free survival for the majority of mHSPC patients
- For young patients, there is a clear benefit from all androgen receptor pathway inhibitors
- For older patients, there should be a consideration of the benefits and risks of abiraterone and “amides.”
- This is the first meta-analysis of individual participant data from the androgen receptor pathway inhibitor trials
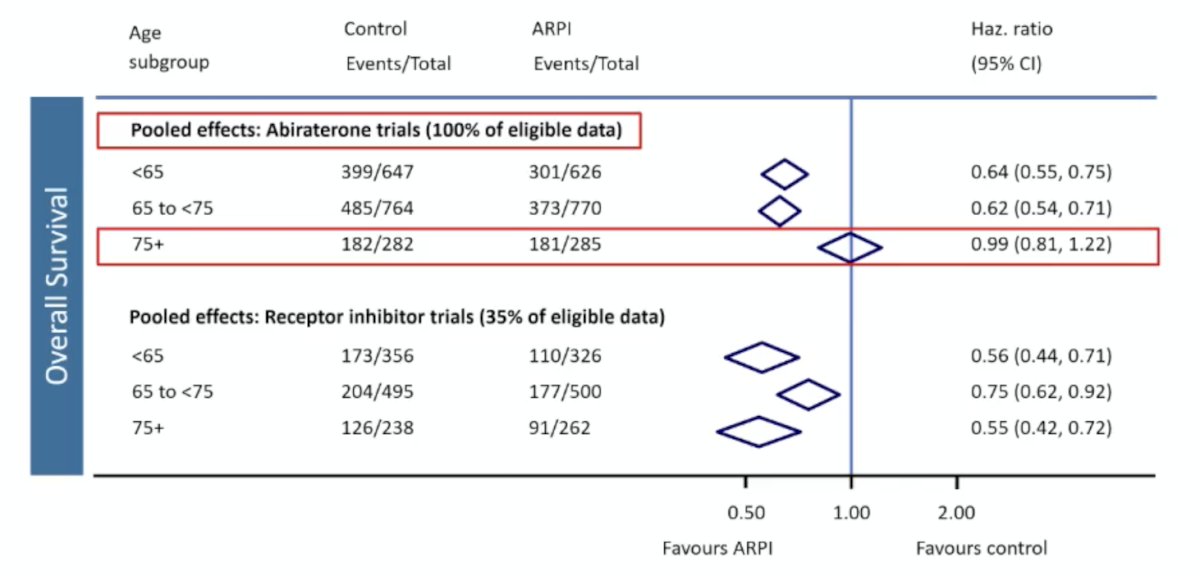
Dr. Rathkopf also presented additional STOPCAP data from David Fisher, who presented a poster at the APCCC 2026 meeting evaluating which people with mHSPC benefit more from androgen receptor pathway inhibitor trials. Androgen receptor pathway inhibitor effects decreased in older age groups (interaction p = 0.0027 for progression-free survival; p = 0.13 for overall survival). These associations differed by class of androgen receptor pathway inhibitor agent (p = 0.022 for progression-free survival; p = 0.0010 for overall survival):
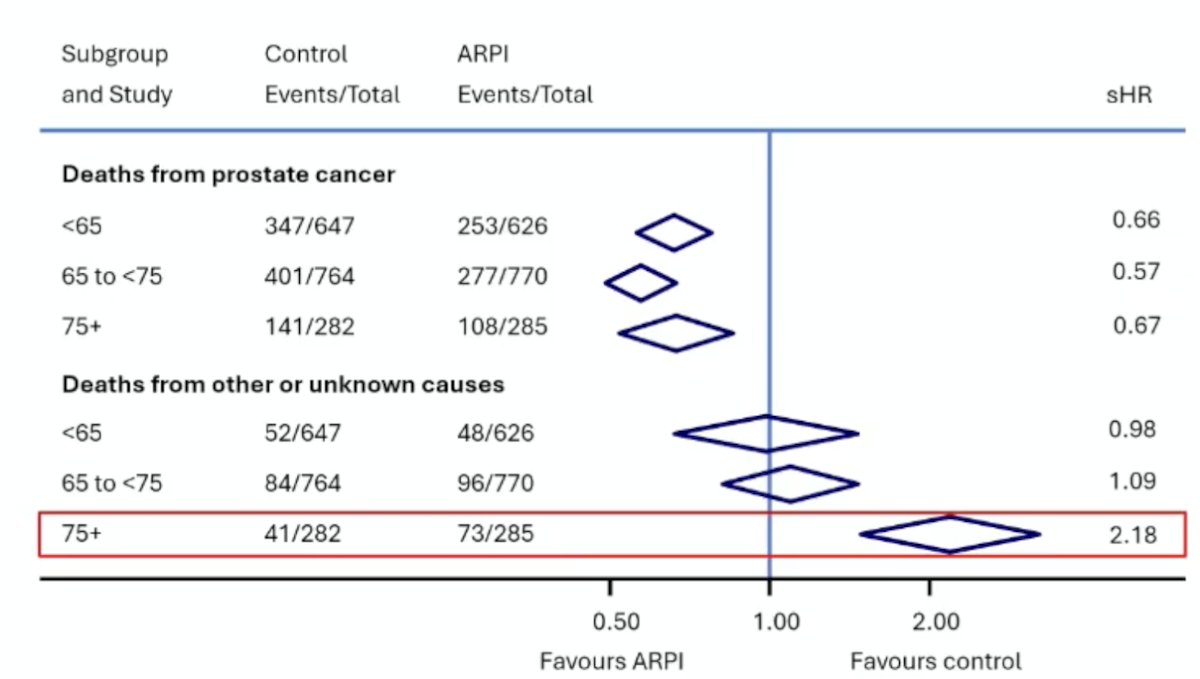
Abiraterone decreased the 5-year cumulative incidence of prostate cancer deaths by ~15% for all age groups, and was associated with ~12% absolute increase in non-cancer deaths in the over-75s age group:
In 2024, El-Taji et al.4 performed a systematic review and meta-analysis of 24 studies assessing cardiovascular events and androgen receptor signaling inhibitors in advanced prostate cancer. The median age was 63–77 years, with ~67% of androgen receptor pathway inhibitor-treated men having≥1 cardiovascular risk factor. Overall, androgen receptor pathway inhibitor + ADT doubled grade ≥3 cardiovascular events (15.6% versus 7.8%; RR 2.10):
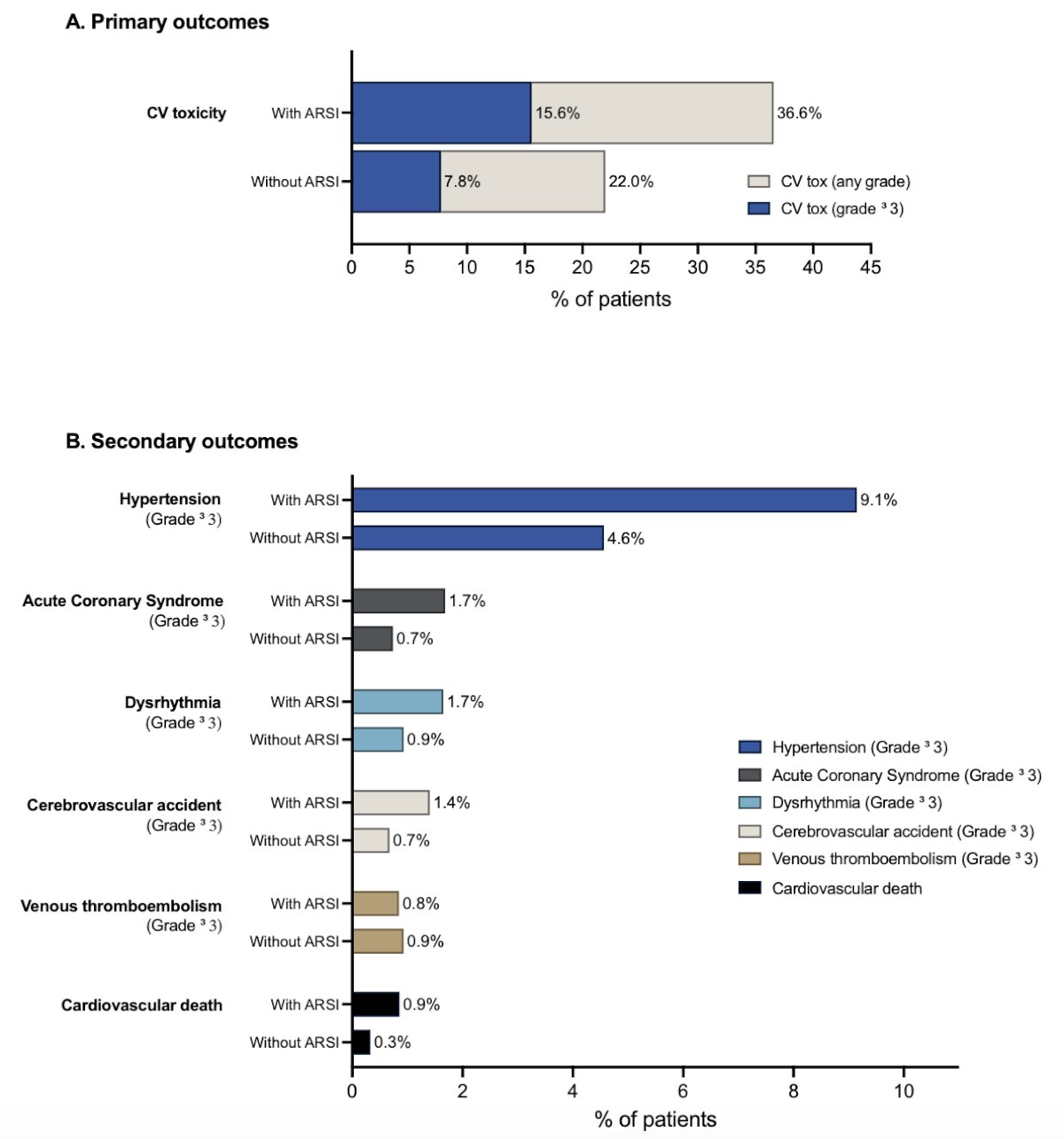
M0 hormone-sensitive prostate cancer had the highest relative risk across states (Grade ≥3 cardiovascular events: 6.9% versus 2.4–3.6%; RR 3.80).
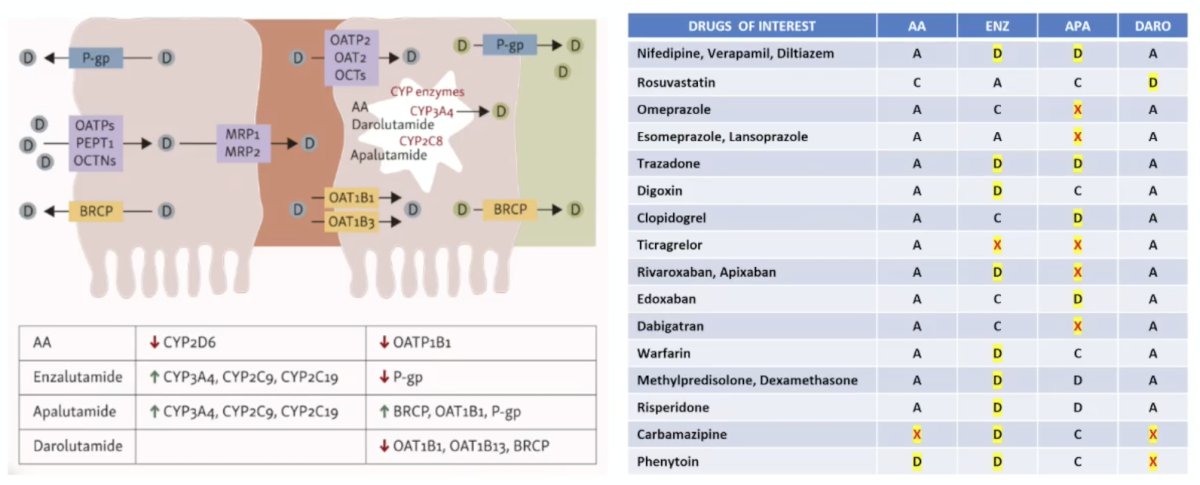
There are several adverse events of interest when considering androgen receptor pathway inhibitors in mHSPC. Abiraterone requires glucocorticoids, which can exacerbate osteoporosis, diabetes mellitus, and immunosuppression, as well as monitoring for mineralocorticoid excess. Enzalutamide and apalutamide can increase the risk of falls, fractures, and CNS-related toxicity (fatigue, cognitive impairment, seizure risk). Darolutamide has less CNS exposure (10-fold) and fewer drug-drug interactions relative to enzalutamide or apalutamide. The following figure and table summarize the drug-drug interactions for enzalutamide, apalutamide, and darolutamide:
Dr. Rathkopf concluded her presentation discussing the considerations for selection of androgen receptor pathway inhibitors in older patients with mHSPC with the following take-home points:
- Fit patients (based on available data)
- ADT + radiotherapy: consider for synchronous, low-volume disease
- Androgen receptor pathway inhibitor doublet: consider receptor inhibitors
- Androgen receptor pathway inhibitor + docetaxel triplet: consider darolutamide for synchronous, high-volume disease
- Vulnerable patients (reversible factors): optimize modifiable factors such as cardiac risk and polypharmacy
- Frail patients (irreversible factors – limited data): the magnitude of benefit with an androgen receptor pathway inhibitor may not be meaningful relative to risk, especially in those with short life expectancy or high competing morbidities
Presented by: Dana Rathkopf, MD, Genitourinary Oncologist, Memorial Sloan Kettering Cancer Center, New York, NY
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 Advanced Prostate Cancer Consensus Conference (APCCC), Lugano, Switzerland, Thurs, April 30 – Sat, May 2, 2026.
References:- Morgans AK, Roy S, Yia AY, et al. Age and treatment intensification in metastatic hormone-sensitive prostate cancer. NEJM Evid. 2025 Nov;4(11):EVIDoa2500109.
- Fizazi K, Foulon S, Carles J, Roubaud G, et al. Abiraterone plus prednisone added to androgen deprivation therapy and docetaxel in de novo metastatic castration-sensitive prostate cancer (PEACE-1): A multicentre, open-label, randomized, phase 3 study with a 2 x 2 factorial design. Lancet. 2022 Apr 30;399(10336):1695-1707.
- Smith MR, Hussain M, Saad F, et al. Darolutamide and Survival in Metastatic, Hormone-Sensitive Prostate Cancer. N Engl J Med. 2022 Mar 24;386(12):1132-1142.
- El-Taji O, Taktak S, Jones C, et al. Cardiovascular events and androgen receptor signaling inhibitors in advanced prostate cancer: A systematic review and meta-analysis. JAMA Oncol. 2024 Jul 1;10(7):874-884.