(UroToday.com) The 2026 APCCC meeting featured a management of metastatic CRCP (mCRPC) session and a presentation by Dr. Gerhardt Attard discussing relevant circulating biomarkers for prostate cancer precision medicine. There are several potential circulating biomarkers, including serum PSA, plasma DNA/circulating tumor DNA (ctDNA), circulating tumor cells, extra-cellular vesicles, and plasma proteins/lipids. In the interest of time, Dr. Attard focused on clinically relevant now/soon circulating biomarkers: serum PSA and plasma DNA/ctDNA.
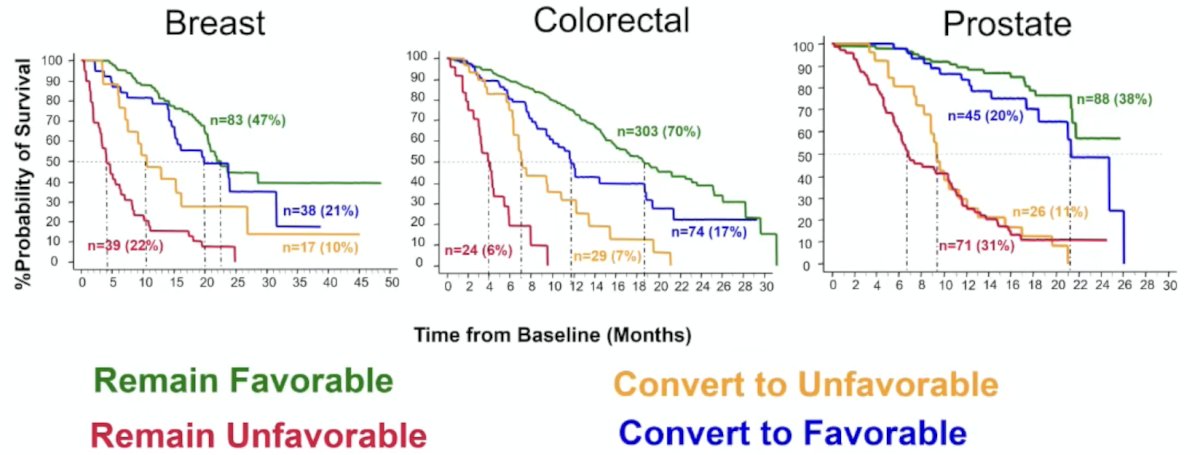
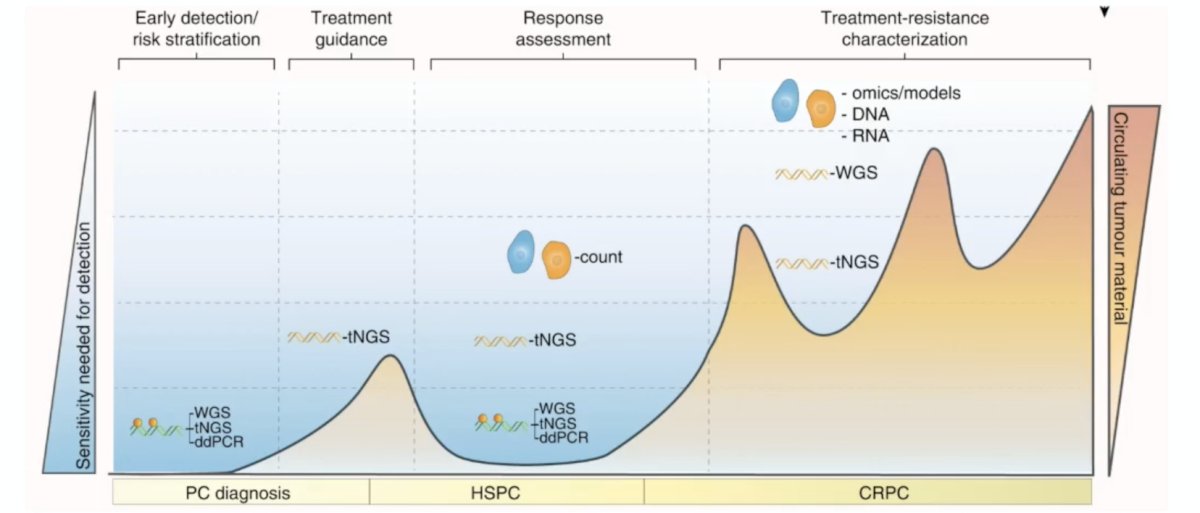
Data from breast and colorectal cancer have led the way with circulating tumor cells data, with the following figure highlighting these two tumor types alongside prostate cancer and the trajectory of ctDNA over time from baseline:
Dr. Attard notes that every test needs a treatment (or intervention) to partner with. For ctDNA in prostate cancer, this includes:
- BRCA2 or BRCA1 partnering with PARP inhibitors
- MSI/dMMR/TMB >= 10, partnering with pembrolizumab
Every physician loves a blood test, but there is currently no other relevant clinical (not on trial) indication for ctDNA in prostate cancer.
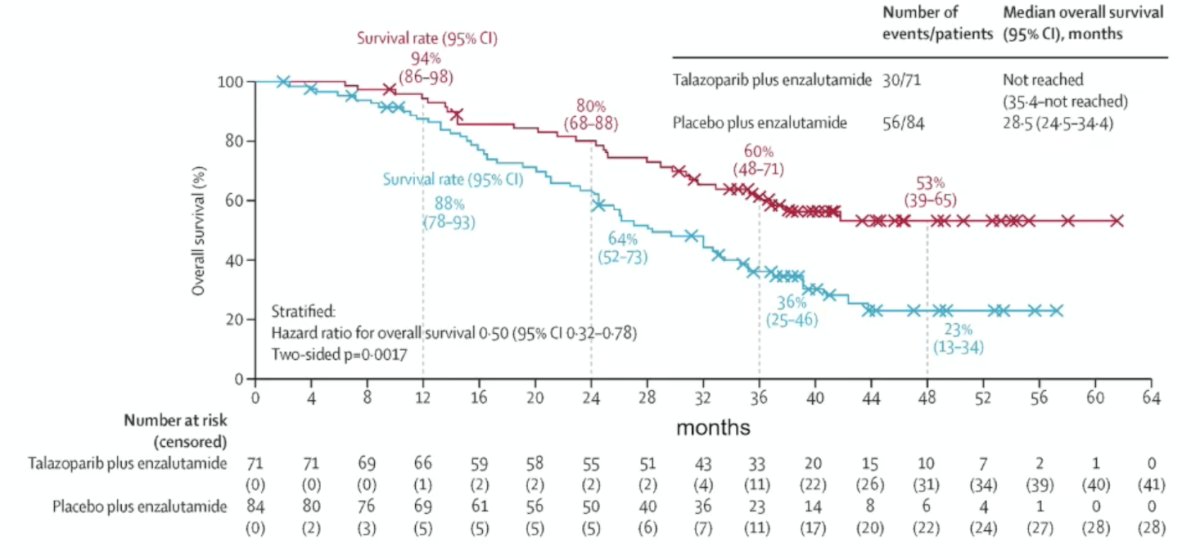
How should we test for BRCA in mCRPC? Dr. Attard emphasized that we should be testing in every possible way. He states that the importance of testing is supported by trial data, such as overall survival in the TALAPRO 2 trial assessing first line talazoparib + enzalutamide versus enzalutamide + placebo (HR 0.50, 95% CI 0.32-0.78) in the BRCA mutated population:1
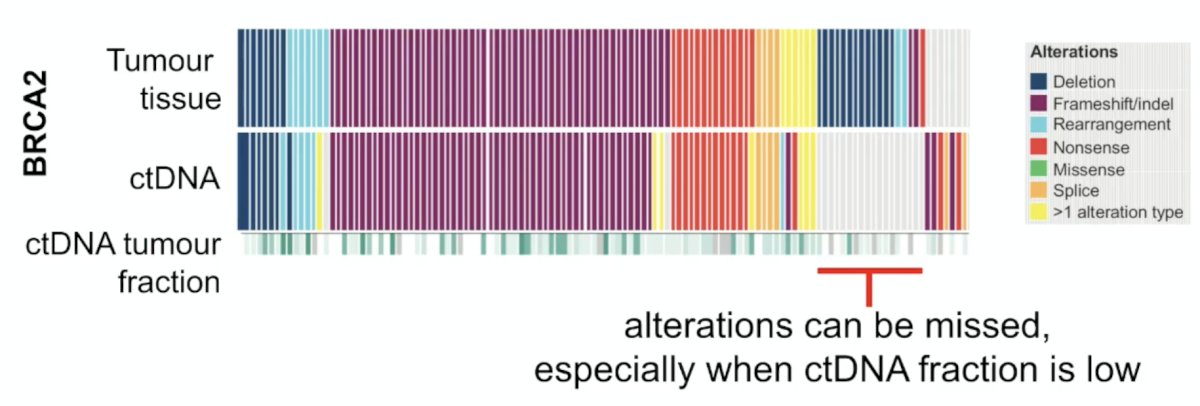
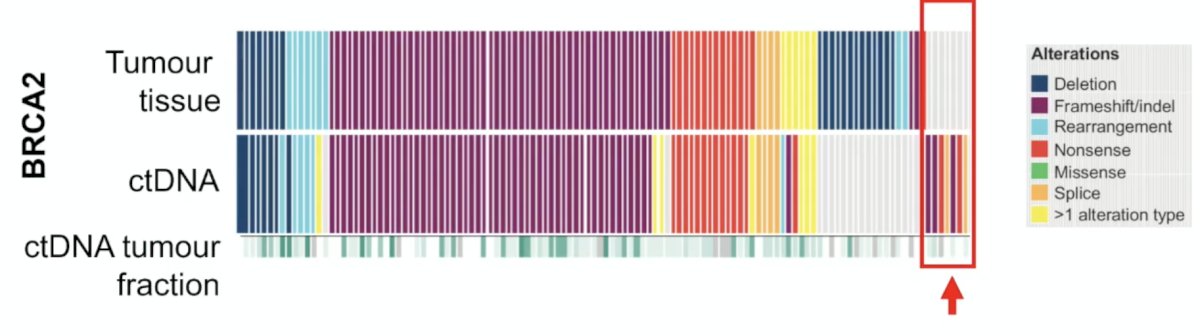
Plasma DNA may be used for BRCA testing, but there are some limitations, including that alterations can be missed, especially when ctDNA fraction is low:
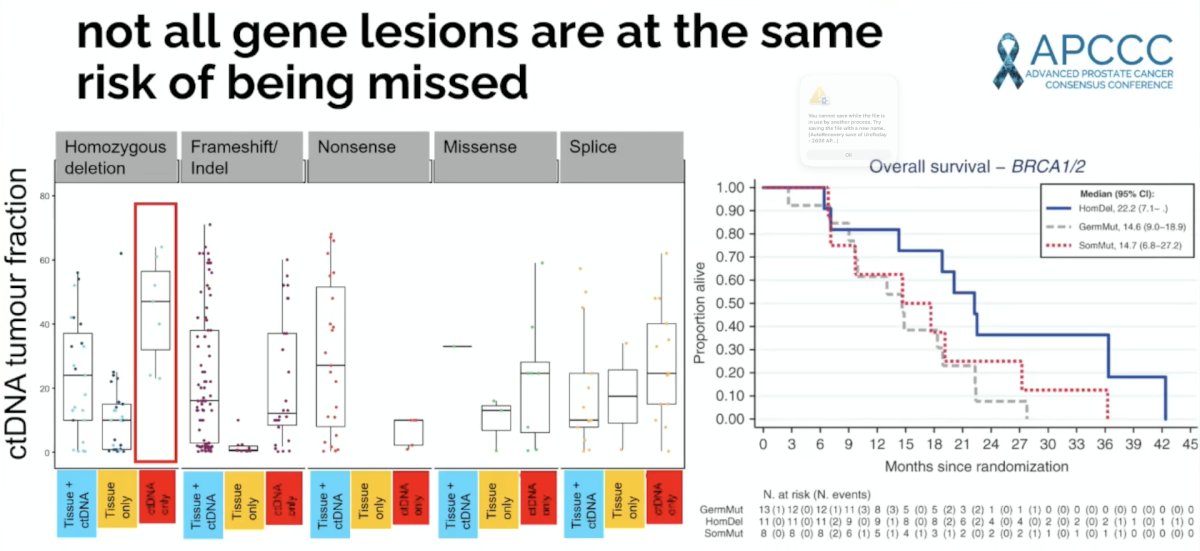
Moreover, Dr. Attard notes that not all gene lesions are at the same risk of being missed:
Importantly, ctDNA fraction is lower at the disease point we now want to test BRCA, so most ctDNA assays are now helpfully reporting estimated tumor fraction:
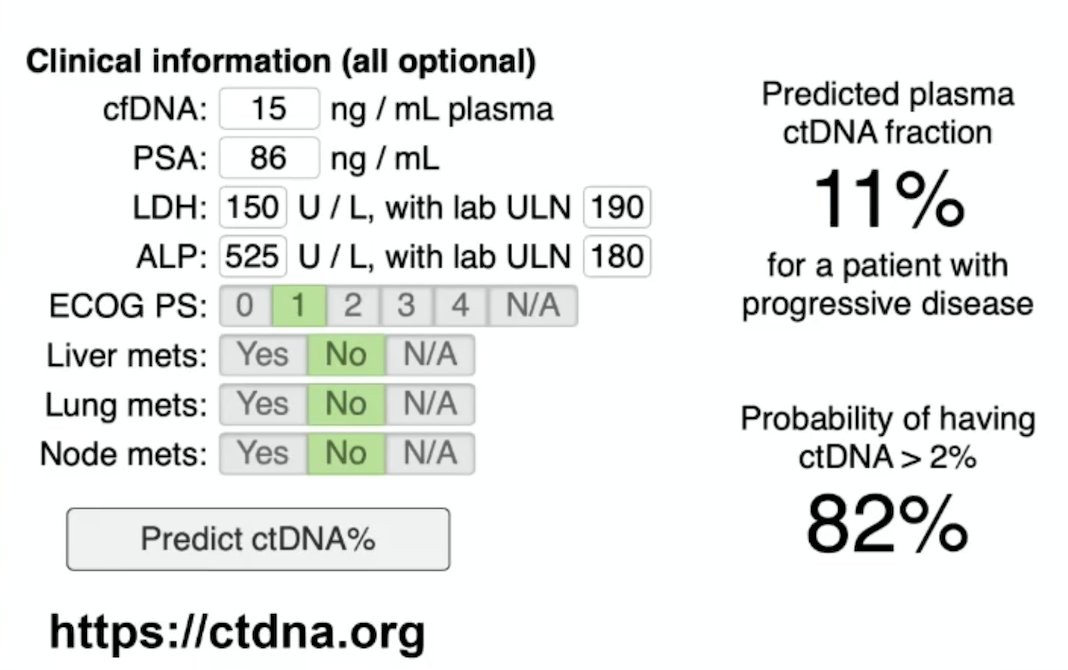
Should we test or should we wait? ctDNA fraction in mCRPC has a predicted plasma ctDNA fraction of 11% for patients with progressive disease, and an 82% probability of ctDNA >2%, according to the following patient characteristics and reported by https://ctdna.org
It is also important to test for ctDNA when the tumor tissue is negative, given that clinical next generation sequencing of FFPE tissue can miss germline mutations in ~10-20% of cases, and there is minimal control over the tissue block selected for testing:
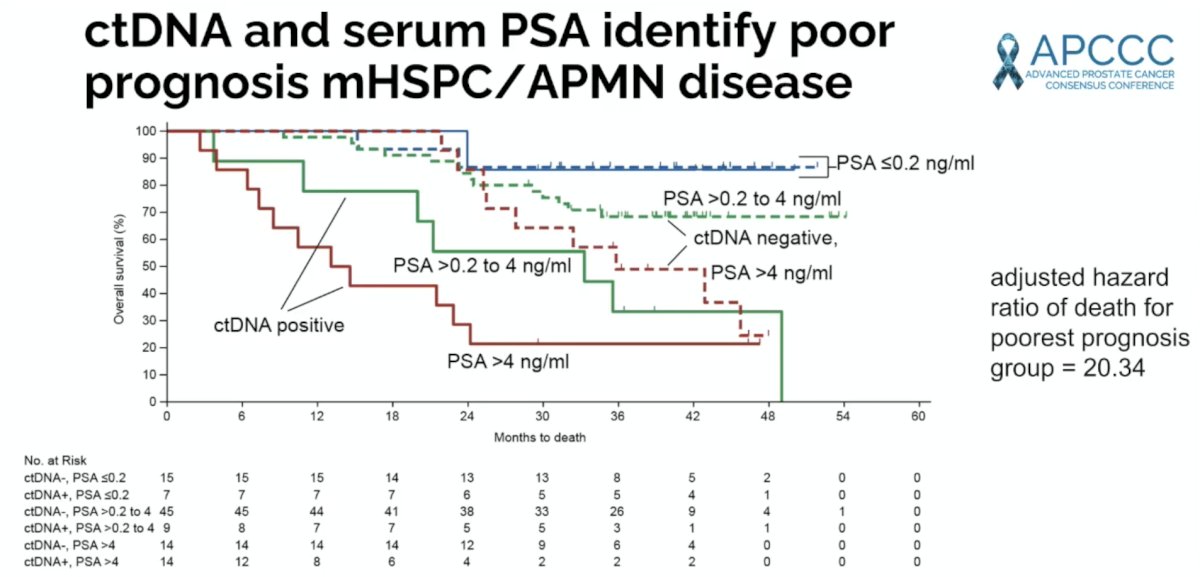
Can we intercept mCRPC? From the breast cancer literature, recent data were presented suggesting a treatment change based on ESR1 mutations in ctDNA. Work presented at IPCS just prior to APCCC 2026 suggests that ctDNA and serum PSA identify poor prognosis mHSPC disease, thus potentially providing the opportunity to intercept and enact treatment change:
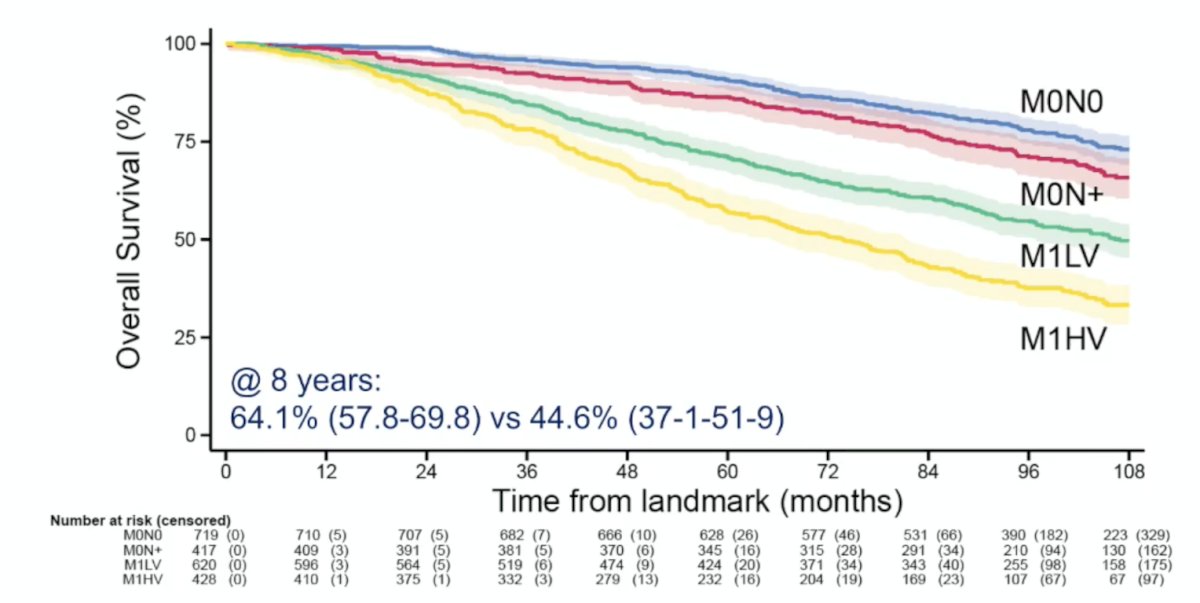
Finally, circulating biomarkers should not be interpreted in isolation. Thus, does baseline metastatic volume make a difference when assessing prognosis for a patient who has a serum PSA <0.2 ng/mL with primary treatment? Based on a recent STAMPEDE platform study2 evaluating the association between PSA nadir values and survival outcomes, stratified by pre-treatment metastatic volume (n = 4,438), the answer is yes. Among patients with metastatic disease in the abiraterone with or without enzalutamide group who had a PSA of 0.2 ng/mL or less at 24 weeks, 96-month overall survival in patients with low-volume metastatic disease (64.1% [95% CI 57.8-69.8]) was higher than in patients with high-volume metastatic disease (44.6% [95% CI 37.1-51.9]), but lower than in patients with non-metastatic, node-positive disease (79.4% [73.8-83.9]):
Presented by: Gerhardt Attard, University College London, London, United Kingdom
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 Advanced Prostate Cancer Consensus Conference (APCCC), Lugano, Switzerland, Thurs, April 30 – Sat, May 2, 2026.
References:
- Agarwal N, Azad AA, Carles J, et al. Talazoparib plus enzalutamide in men with first-line metastatic castration-resistant prostate cancer (TALAPRO-2): A randomized, placebo-controlled, phase 3 trial. Lancet. 2023 Jul 22;402(10398):291-303.
- Kayani M, Murphy L, Dutey-Magni P, et al. On-treatment serum prostate-specific antigen and overall survival in prostate cancer (STAMPEDE platform protocol): A post-hoc analysis of data from five phase 3 trials. Lancet Oncol. 2026 May;27(5):625-636.