(UroToday.com) The 2026 Advanced Prostate Cancer Consensus Conference (APCCC) meeting featured a poster session and a presentation by David Fisher discussing a STOPCAP meta-analysis of individual participant data assessing which patients with metastatic hormone sensitive prostate cancer (mHSPC) benefit from androgen receptor pathway inhibitors. Effects of adding androgen receptor pathway inhibitors to ADT may be modified by clinical features of mHSPC. This STOPCAP collaborative meta analysis of individual participant data aimed to investigate if patient or tumor characteristics influence androgen receptor pathway inhibitor efficacy, and determine who benefits most. The investigators sought individual participant data for completed trials examining the effects of adding androgen receptor pathway inhibitors to ADT-based standard of care for mHSPC.
For this study, analyses of main effects were based on overall survival. Pooled effects were estimated using two-stage common effect meta analysis of hazard ratios, adjusted for age, PSA, performance status, Gleason score, planned docetaxel use, and adaptations to trial design. Interaction effects were based on progression free survival to maximize power, then overall survival where significant progression free survival interactions were found. Prostate cancer specific survival was analyzed where data allowed, and competing-risks analysis of causes of death was used to estimate sub-distribution hazard ratios and 5-year absolute effects.
David Fisher and colleagues obtained updated individual participant data from 7 trials and 7,778 participants:
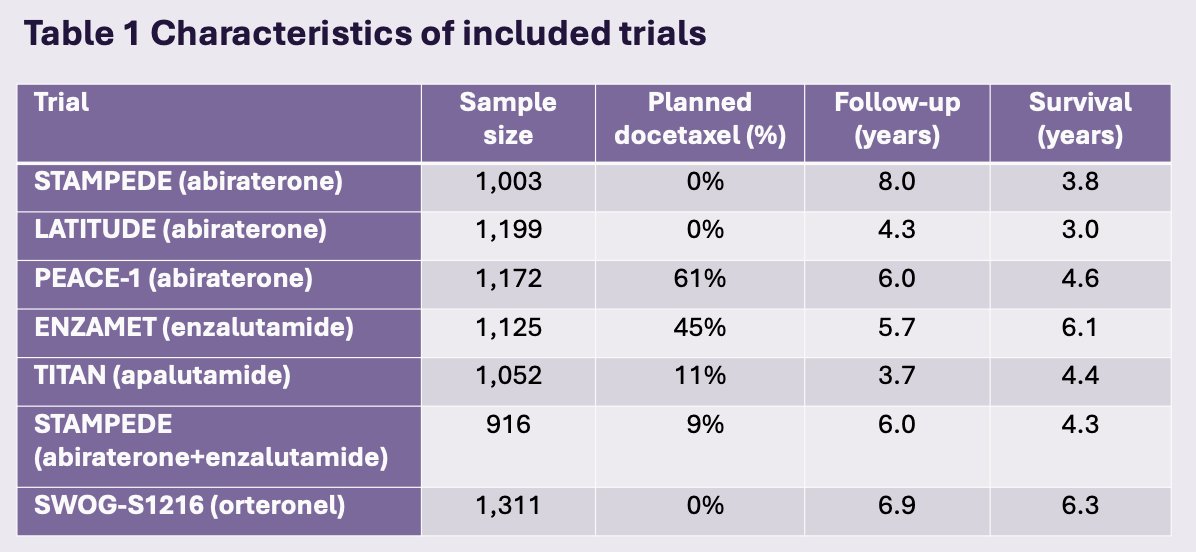
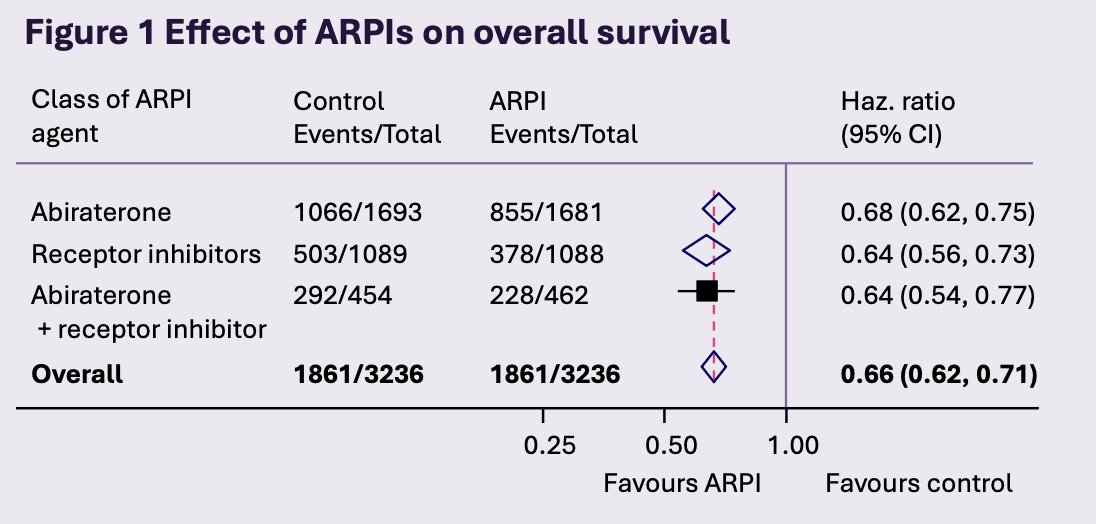
These represent 100% of the eligible data from biosynthesis inhibitor trials and 35% of the eligible data from receptor inhibitor trials. Adding an androgen receptor pathway inhibitor to ADT improved overall survival and progression free survival, with 13% and 21% absolute benefits at 5 years, respectively:
Although SWOG-S1216 was excluded from this primary analysis (no progression free survival or volume data), inclusion in sensitivity analysis gave similar results.
Androgen receptor pathway inhibitor effects decreased in older age groups (interaction p = 0.0027 for progression free survival; p = 0.13 for overall survival). These associations differed by class of androgen receptor pathway inhibitor agent (p = 0.022 for progression free survival; p = 0.0010 for overall survival):
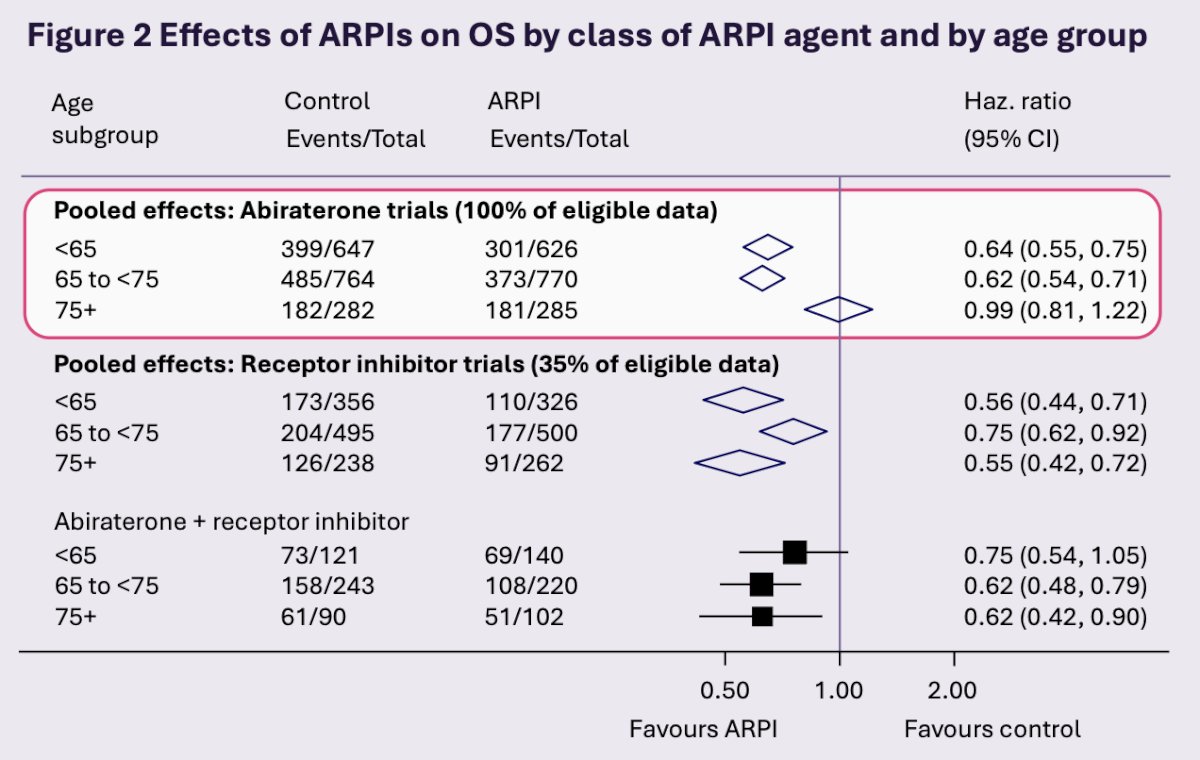
There was no evidence that the effects of the androgen receptor pathway inhibitor varied by disease volume, docetaxel use, Gleason score, WHO performance status, or metastatic burden.
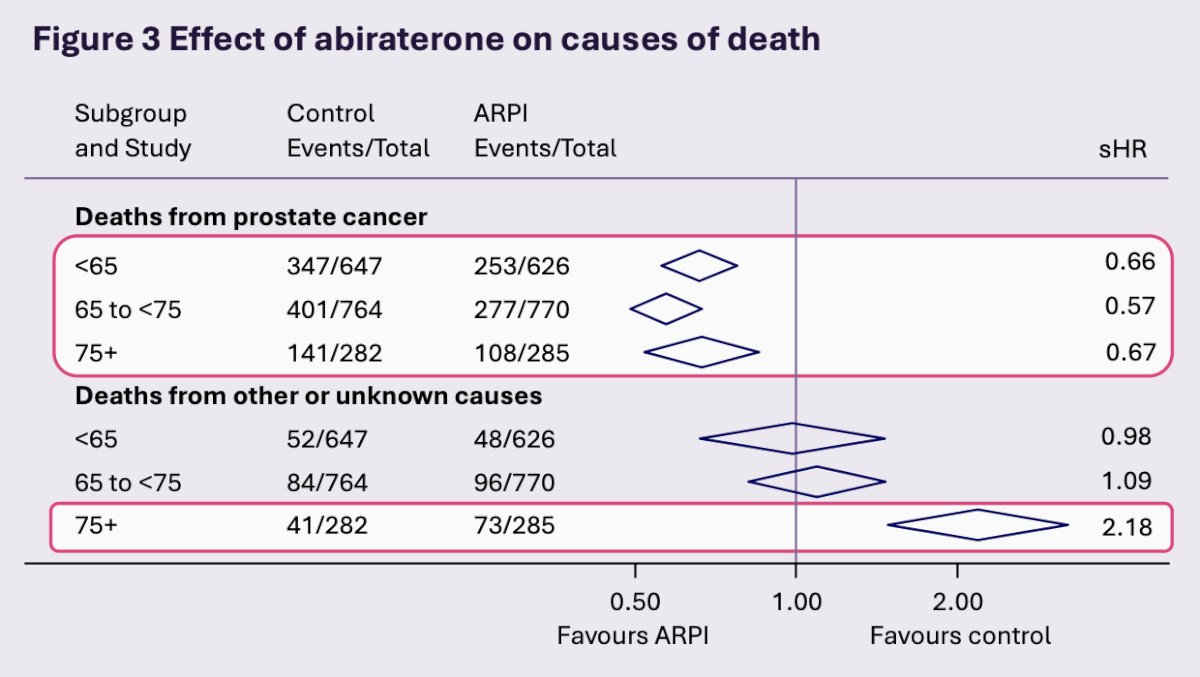
Abiraterone decreased 5-year cumulative incidence of prostate cancer deaths by ~15% for all age groups, and was associated with ~12% absolute increase in non-cancer deaths in the over-75s age group:
David Fisher concluded his presentation discussing which patients with mHSPC benefit from androgen receptor pathway inhibitors with the following take-home points:
- Androgen receptor pathway inhibitors improve survival outcomes in men with mHSPC, regardless of disease volume or docetaxel use
- For younger patients, all androgen receptor pathway inhibitors showed a clear benefit
- For older patients, abiraterone benefits appear reduced, likely due to more non-cancer deaths
- Currently, due to insufficient data, effects of receptor inhibitors on non-cancer mortality in older patients are uncertain
- Patient age and comorbidities need careful consideration when selecting androgen receptor pathway inhibitor therapy
Presented by: David Fisher, MRC Clinical Trials Unit, UCL, London, United Kingdom
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 Advanced Prostate Cancer Consensus Conference (APCCC), Lugano, Switzerland, Thurs, April 30 – Sat, May 2, 2026.