(UroToday.com) The 2026 Advanced Prostate Cancer Consensus Conference (APCCC) meeting featured a poster session and a presentation by Dr. Laura Resa-Forns discussing early PSA response, tolerability, and treatment related adverse events among patients receiving darolutamide in a multi-institutional Spanish real world cohort. Darolutamide has demonstrated efficacy and a favorable safety and tolerability profile in pivotal phase 3 trials (ARAMIS,1 ARASENS,2 and ARANOTE3) across three distinct prostate cancer stages: non-metastatic castration-resistant (nmCRPC), metastatic hormone sensitive with docetaxel (mHSPC), and chemotherapy-free mHSPC. However, patients treated in routine clinical practice are often older, poly-medicated, and managed with diverse treatment intensification strategies. Real world analyses complement trial findings by evaluating treatment outcomes in broader, unselected populations representative of clinical practice. The objective of this study, presented at APCCC 2026, was to evaluate early PSA response in prostate cancer patients receiving darolutamide and to assess its association with disease progression and mortality. The incidence, severity, and profile of treatment related adverse events, as well as the rate of treatment discontinuations, were also evaluated.
This retrospective multi-institutional Spanish real world observational study included patients with HSPC or CRPC, both metastatic and non-metastatic, treated with darolutamide. Early PSA response was defined as a ≥90% decline from baseline (PSA90), PSA <0.2 ng/mL, or PSA <0.02 ng/mL within 3 months of treatment initiation. mHSPC patients were stratified by treatment intensity (ADT + darolutamide doublet versus ADT + docetaxel + darolutamide triplet) and classified according to the definition of polypharmacy (≥5 drugs). Adverse events were graded according to the CTCAE v5.0 and classified as treatment related or unrelated. Associations between early PSA response, disease stage, and clinical outcomes, and comparisons across disease stages and treatment intensities were analyzed using chi-square or Fisher’s exact tests and Cox regression models.
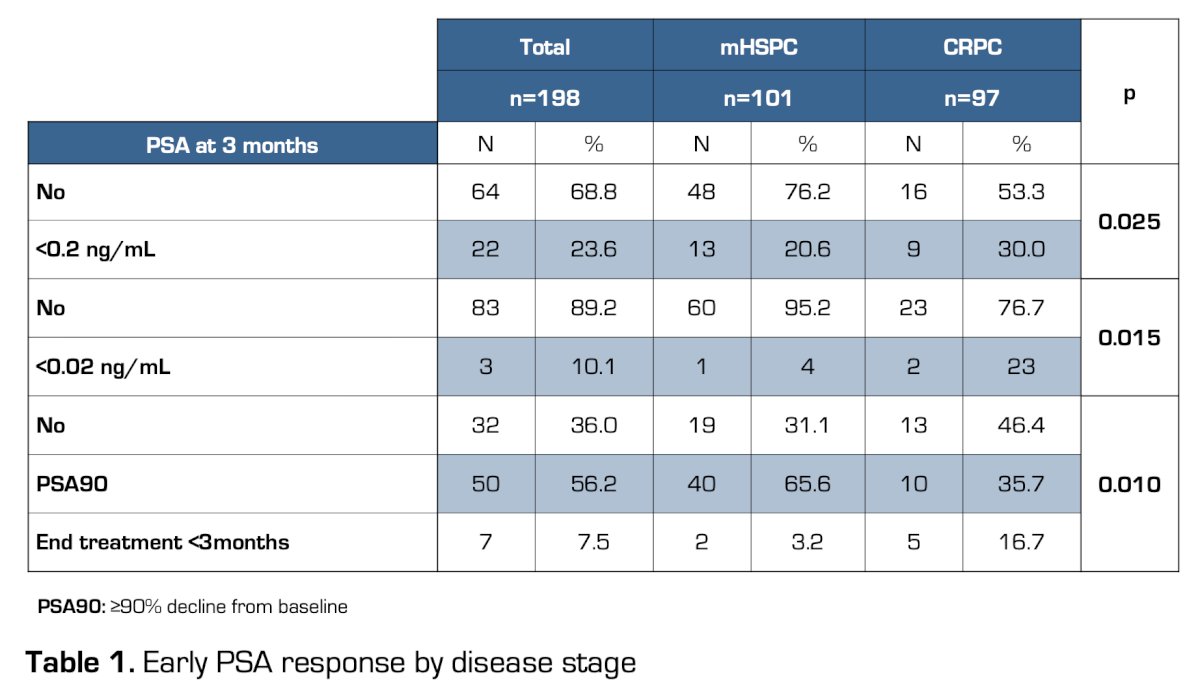
A total of 198 patients were included: 101 (51%) with mHSPC and 97 (49%) with CRPC. The median follow-up was 14.6 months (IQR 7.2–25.2). The cohort was characterized by advanced age (median 72 years, SD ± 10) and extensive polypharmacy, with a mean of 9.8 ± 3.4 concomitant medications, and 91% of patients met the definition of polypharmacy. The median PSA at diagnosis was 39 ng/mL (IQR 12–144), decreasing to 0.79 ng/mL (IQR 0.2–4.1) at 3 months (p = 0.92 between disease stages). A PSA of <0.2 ng/mL was achieved in 23.6% of patients overall (20.6% mHSPC versus 30.0% CRPC; p = 0.025), while PSA <0.02 ng/mL occurred in 10.1% (4% mHSPC versus 23% CRPC; p = 0.015):
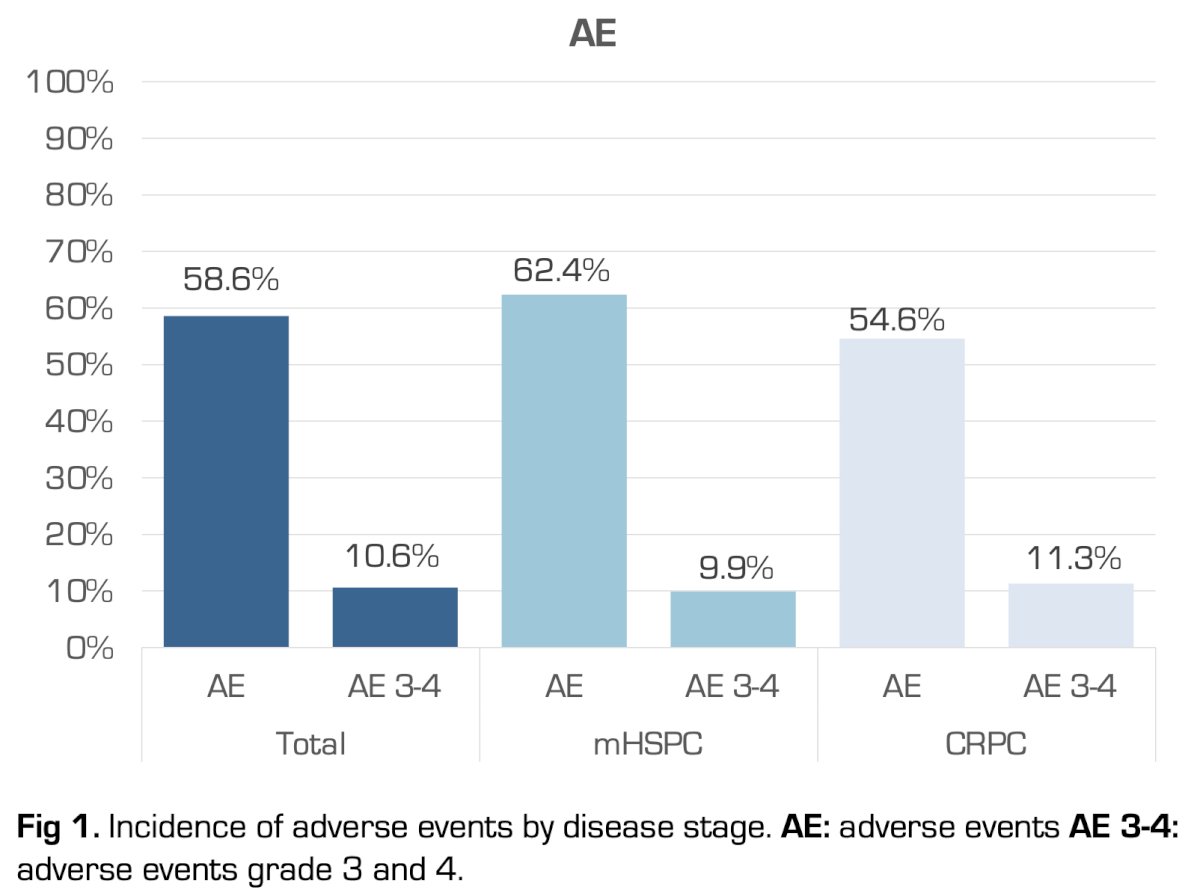
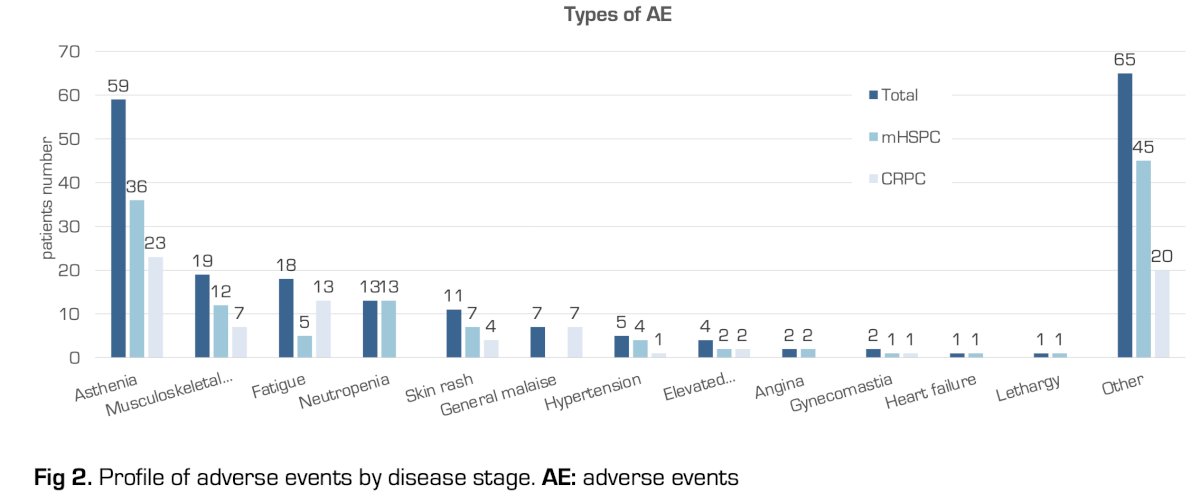
There were 78 patients (39.4%) on polypharmacy (n = 33 mHSPC, n = 45 CPRC), of which 7.5% discontinued treatment before 3 months, with higher rates in CRPC (16.7% versus 3.2%). Any grade treatment related adverse events occurred in 58.6% of patients. Grade ≥3 adverse events were observed in 10.6%, most commonly fatigue (3.0%), hypertension (2.5%), and rash (1.5%). Serious adverse events leading to hospitalization occurred in 4.0%, with no treatment-related deaths reported:
Treatment discontinuation due to adverse events occurred in 6.5% of patients, slightly higher among patients receiving triplet therapy (8.3% versus 5.1%; p = 0.34). At 36 months, the estimated overall survival was 62% (95% CI 48–73%), with a median overall survival of 44.7 months. Progression free survival was 61% (95% CI 47–72%). In mHSPC, the 36-month overall survival approached 70%, consistent with pivotal trial outcomes. In CRPC, overall survival and progression free survival were within expected real world ranges:
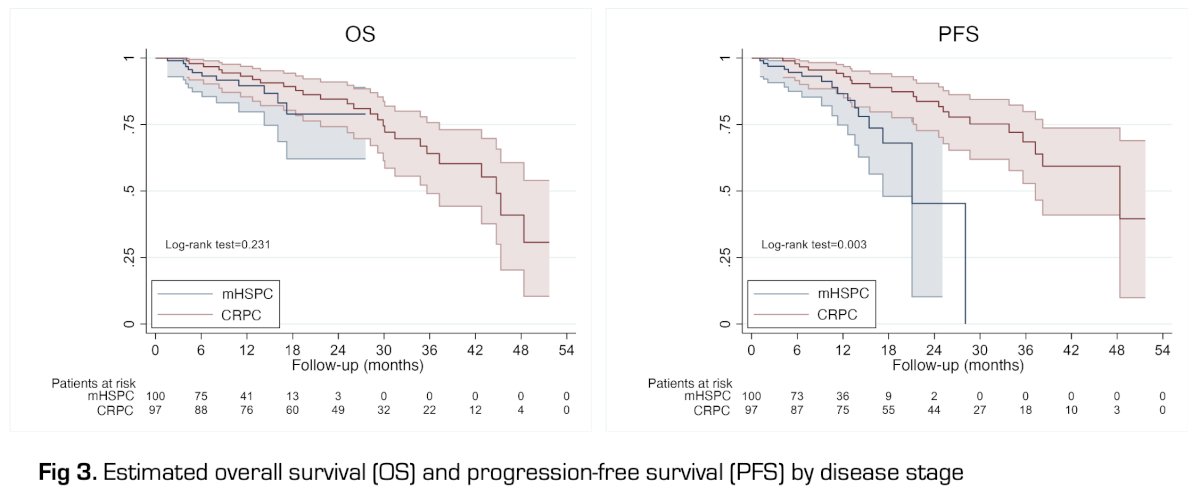
Patients achieving PSA90 exhibited significantly longer overall survival (HR 0.24; p = 0.026) and progression free survival (HR 0.85; p = 0.733). The safety profile remained consistent across disease stages and treatment regimens.
Dr. Resa-Forns concluded her presentation discussing early PSA response, tolerability, and treatment related adverse events among patients receiving darolutamide in a multi-institutional Spanish real-world cohort with the following take-home points:
- In this multi-institutional Spanish real world cohort, early PSA response to darolutamide varied by disease stage, with more pronounced effects in complete response settings
- Early PSA decline was associated with improved progression free survival and overall survival, reinforcing the external validity of darolutamide efficacy under routine clinical conditions
- Additionally, darolutamide demonstrated a favorable safety and tolerability profile, despite high rates of polypharmacy
- The low incidence of grade ≥3 adverse events and treatment discontinuations supports the reproducibility of the tolerability observed in pivotal trials under real world conditions
Presented by: Laura Resa-Forns, Hospital Fundación, Madrid, Spain
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 Advanced Prostate Cancer Consensus Conference (APCCC), Lugano, Switzerland, Thurs, April 30 – Sat, May 2, 2026.
References:
- Fizazi K, Shore N, Tammela TL, et al. Darolutamide in nonmetastatic castration-resistant prostate cancer. N Engl J Med. 2019;380(13):1235-1246.
- Smith MR, Hussain M, Saad F, et al. Darolutamide and Survival in Metastatic, Hormone-Sensitive Prostate Cancer. N Engl J Med. 2022 Mar 24;386(12):1132-1142.
- Saad F, Vjaters E, Shore N, et al. Darolutamide in Combination with Androgen-Deprivation Therapy in Patients with Metastatic Hormone-Sensitive Prostate Cancer From the Phase III ARANOTE Trial. J Clin Oncol. 2024 Dec 20;42(36):4271-4281.