(UroToday.com) The 2026 Advanced Prostate Cancer Consensus Conference (APCCC) meeting featured a management of metastatic hormone sensitive prostate cancer (mHSPC) session and a presentation by Dr. Nicholas van As discussing the optimal management of metachronous oligometastatic hormone sensitive prostate cancer on PSMA PET. Since PSMA PET has created new opportunities (and new uncertainty), there are four key questions that define management:
What are we really treating?- Local disease? Prostate/prostate bed
- Regional disease? Pelvic lymph nodes
- Systemic disease? Distant nodes and bone metastases
- Does detecting more disease change management?
- Should all PSMA lesions be treated?
- ADT alone versus intensification?
- Finite versus continuous treatment?
- Who can safely de-escalate treatment?
- Is cure achievable in some patients?
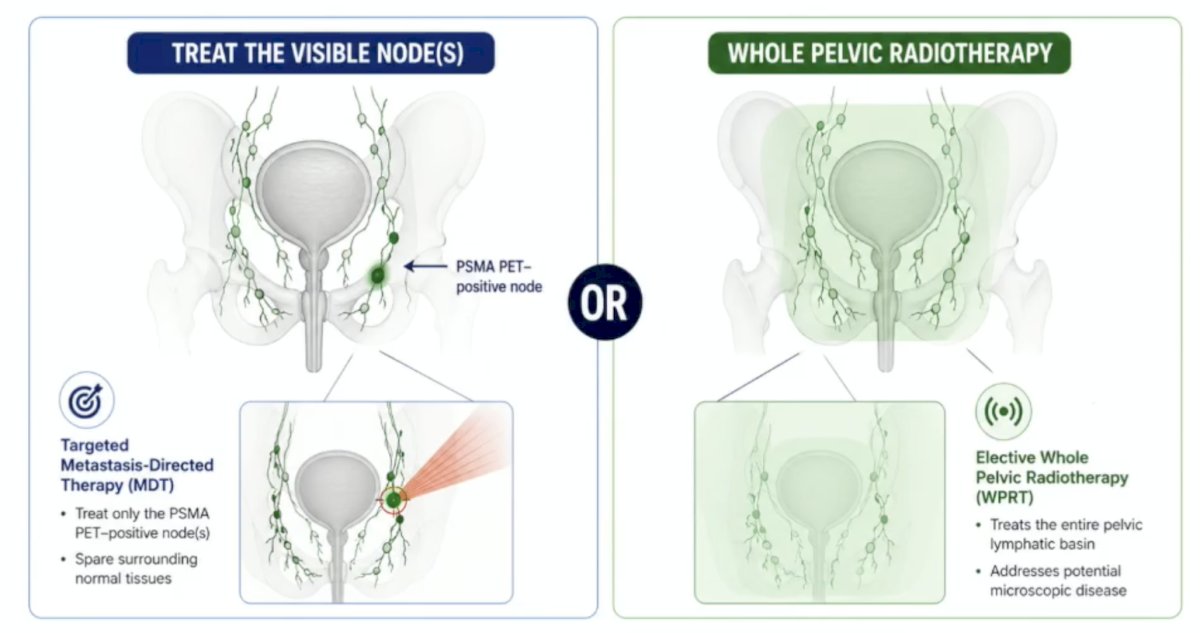
PSMA PET detects nodal relapse in the pelvis, but should these patients have treatment of all visible nodes with targeted metastasis directed therapy or have whole pelvic radiotherapy to the entire lymph node basin?
This question was asked in the STORM/PEACE V trial, which is a phase II randomized trial of metachronous oligorecurrent nodal disease (<= 5 nodes) on PSMA PET. All patients had prior radical treatment (radical prostatectomy or radiotherapy), and all patients received 6 months of ADT, with a primary endpoint of metastasis free survival. Arm A had MDT alone + 6 months of ADT, and Arm B had elective nodal radiotherapy + metastasis directed therapy + 6 months of ADT:
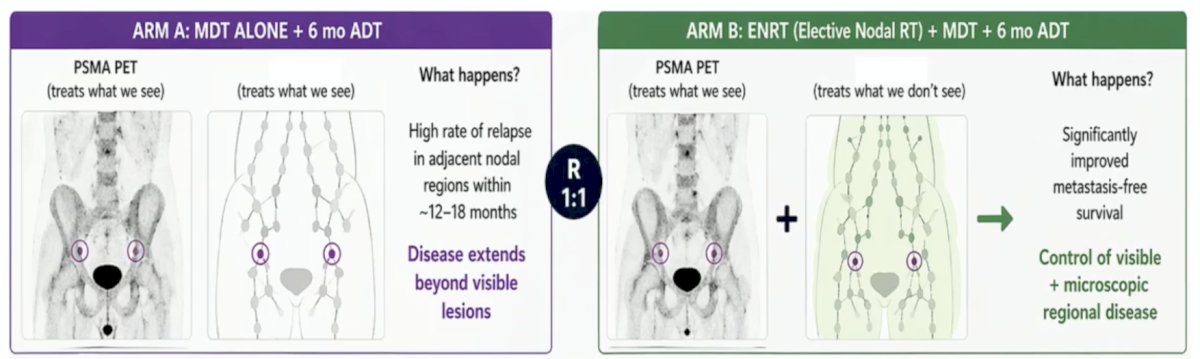
Dr. van As emphasized that STORM is not metastasis directed therapy versus no metastasis directed therapy, rather it tests focal metastasis directed therapy versus regional (elective) nodal radiotherapy, both on a background of systemic therapy.
In the metachronous oligometastatic hormone sensitive prostate cancer, one question is: should we add an androgen receptor pathway inhibitor early? EMBARK was a phase III, double-blind study among high risk biochemical recurrence patients (PSA doubling time <= 9 months), randomizing patients to Arm A (ADT + placebo) versus Arm B (ADT + enzalutamide).1 Amongst the key results, the 5 year metastasis free survival rate for ADT + placebo was 66.1% versus 87.3% for ADT + enzalutamide (HR 0.42, 95% CI 0.30-0.61). Importantly, the intermittent strategy maintained a benefit, with lower cumulative toxicity versus continuous therapy, and preservation of quality of life. PRESTO was a phase III, open label trial among patients with high risk biochemical recurrence (PSA doubling time <= 9 months), randomizing men to Arm A (ADT) versus Arm B (ADT + apalutamide) versus Arm C (ADT + apalutamide + abiraterone), with treatment being for 12 months.2 The key results included a median progression free survival of 20.0 months for ADT, 25.1 months for ADT + apalutamide (HR 0.49, 95% CI 0.39-0.61), and 26.0 months for ADT + apalutamide + abiraterone (HR 0.50, 95% CI 0.40-0.62). Testosterone recovery at 12-18 months was similar across all arms (~90%), with manageable toxicity, and no new safety signals.
Dr. van As notes that we do not currently have good evidence to use an androgen receptor pathway inhibitor with stereotactic body radiotherapy/metastasis directed therapy in PSMA detected disease. However, Dr. Piet Ost is conducting the DART trial among oligorecurrent hormone sensitive prostate cancer patients (n = 128) with <= 5 metastases based on PSMA PET. Patients will be randomized to stereotactic body radiotherapy alone versus stereotactic body radiotherapy + 6 months of darolutamide.
Dr. van As then presented a case presentation of a 75 year old man who had a radical prostatectomy 6 years ago for Gleason 3+4 disease and an initial PSA of 9 ng/mL. Post-operatively, he had negative margins and an undetectable PSA, his PSA started to rise four years after surgery, with a PSA doubling time of ~12 months. His current PSA is 0.7 ng/mL, and a PSMA PET/CT showed one pelvic lymph node. There are five treatment options for this patient, so what is the most appropriate management?
- Metastasis directed therapy to the node with 6 months of ADT
- Metastasis directed therapy + pelvic radiotherapy with 6 months of ADT
- Metastasis directed therapy + long term ADT
- Metastasis directed therapy + ADT + an androgen receptor pathway inhibitor
- Systemic therapy alone with ADT + an androgen receptor pathway inhibitor
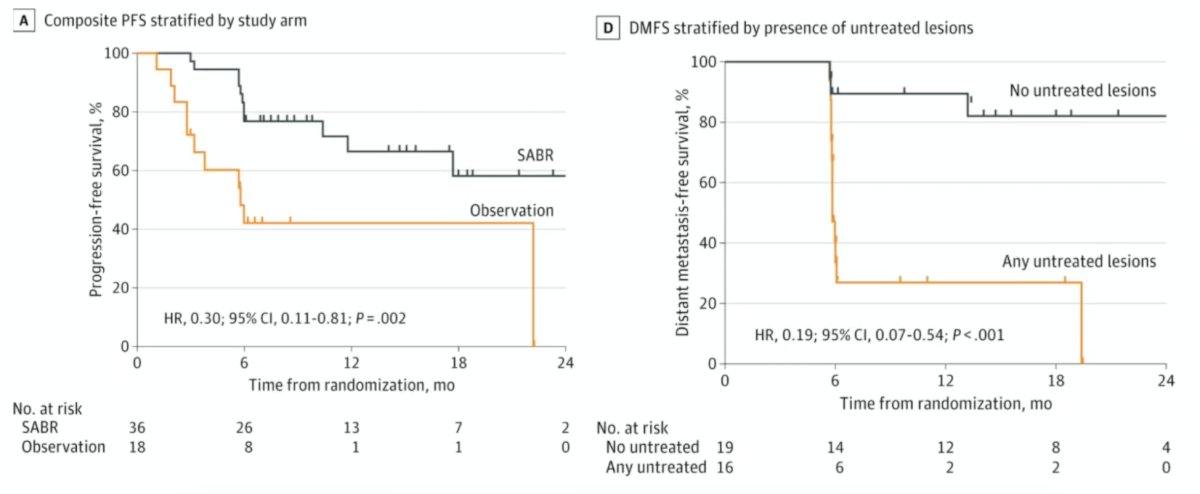
Does PSMA PET imaging make a difference? In the ORIOLE trial,3 all patients received conventional imaging and PSMA PET/CT, and physicians were blinded to the PSMA result. In the following Kaplan-Meier curves for composite progression free survival (HR 0.30, 95% CI 0.11-0.81) and distant metastasis free survival (HR 0.19, 95% CI 0.07-0.54), no untreated lesions had significantly improved outcomes compared to any untreated lesions:
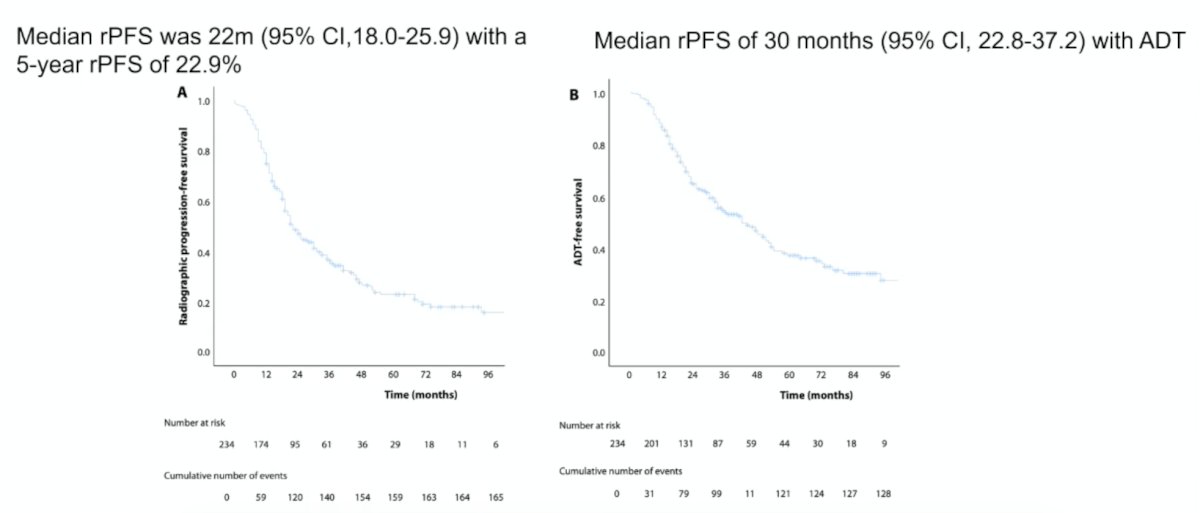
Dr. van As and colleagues recently published a study assessing predictors of long term disease free survival with stereotactic body radiation therapy for oligometastatic prostate cancer.4 From 2011 to 2023, 234 patients with ≤ 3 hormone sensitive metachronous prostate cancer oligometastases were treated with stereotactic body radiation therapy in the United Kingdom. Concurrent ADT was allowed by clinician discretion. In total, 308 lesions were treated in 234 patients:
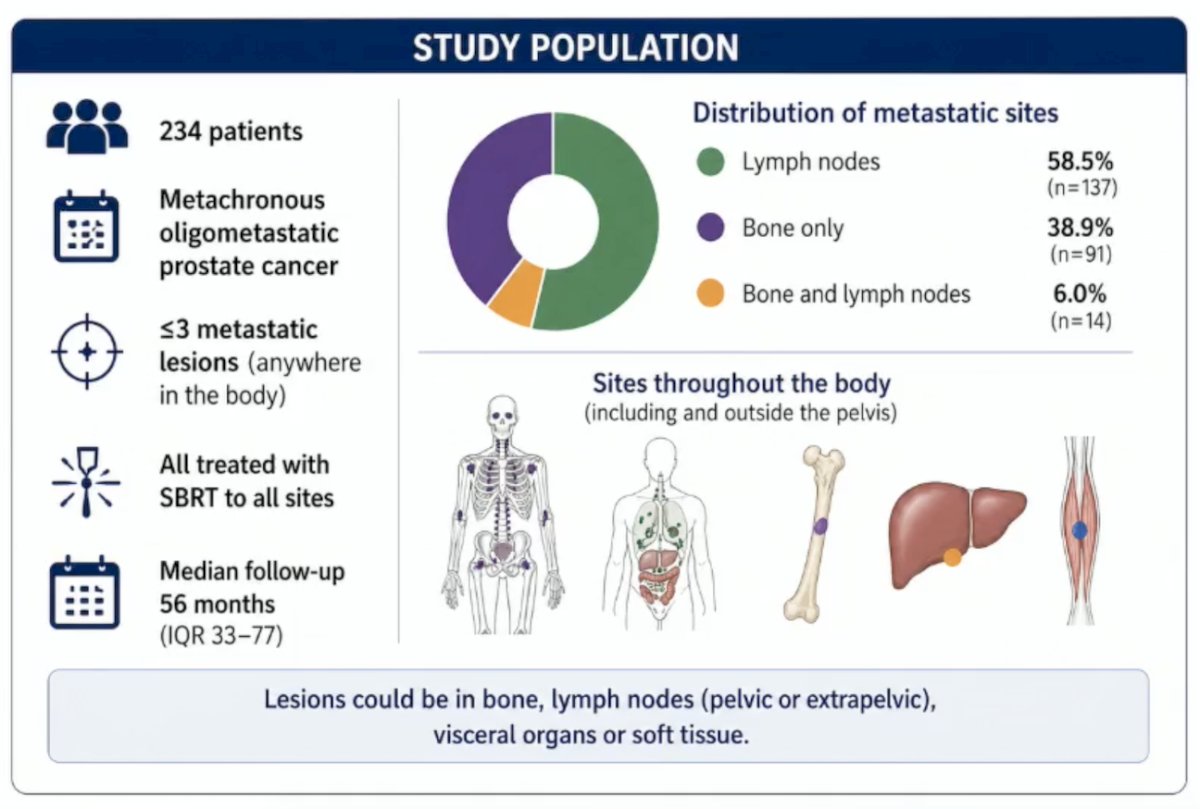
After a median follow-up of 56.5 months, the median radiographic progression free survival for stereotactic body radiation therapy was 22 months (95% CI 18.0-25.9) with a 5 year radiographic progression free survival rate of 22.9%. Among patients receiving concurrent ADT, the median radiographic progression free survival was 30 months (95% CI 22.8-37.2):
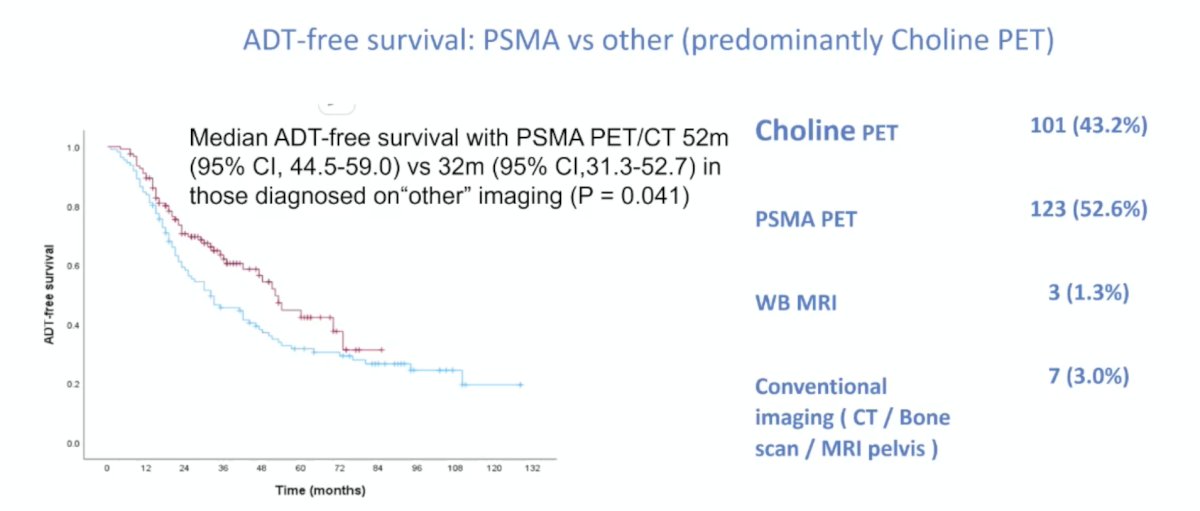
Patients diagnosed with oligometastases using baseline PSMA PET/CT had longer median ADT-free survival than those diagnosed with "other" imaging methods (52 versus 32 months, p = 0.041):
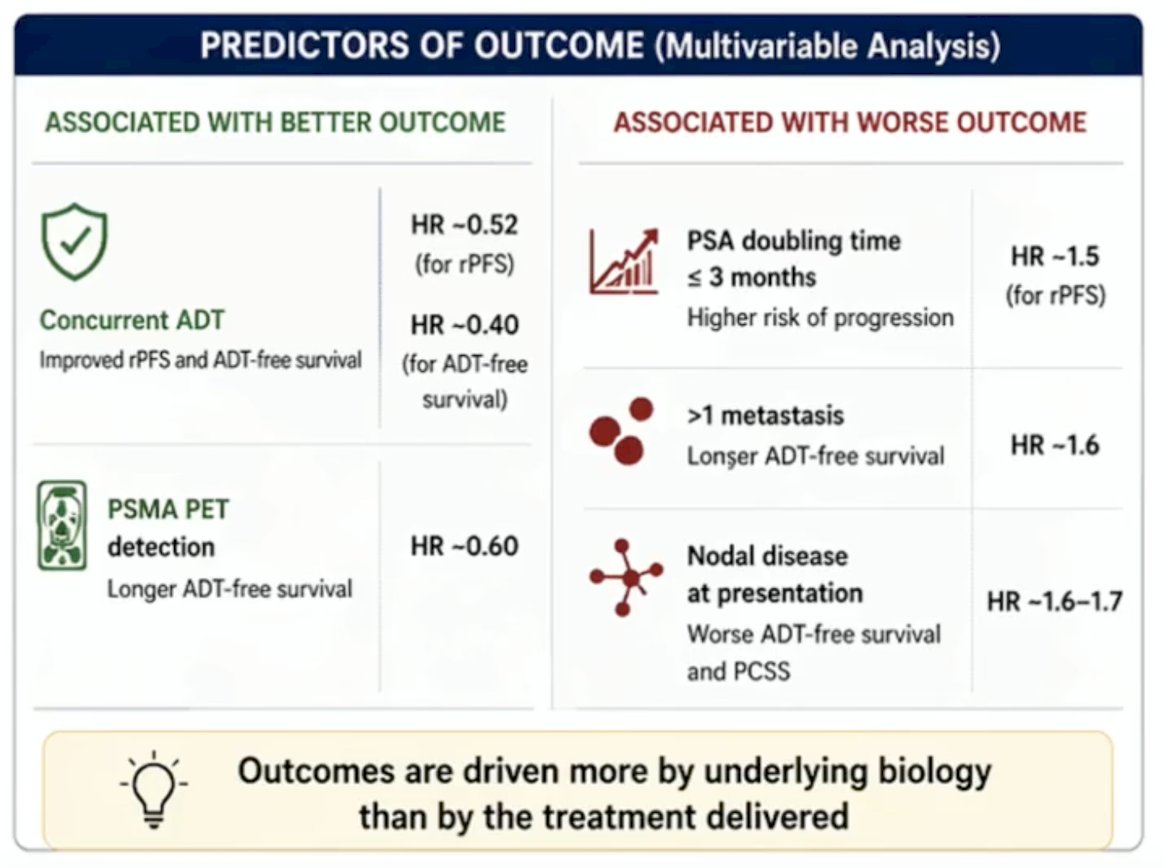
The 5-year prostate cancer specific survival rate was 96.4%, and the median was not reached. A summary of the outcomes from this study is highlighted in the following figure:

Predictors of better outcomes on multivariable analyses included concurrent ADT and PSMA PET detection of disease, whereas predictors of worse outcomes included a PSA doubling time <= 3 months, > 1 metastasis, and nodal disease at presentation:
Dr. van As concluded his presentation discussing the optimal management of metachronous oligometastatic hormone sensitive prostate cancer on PSMA PET by highlighting key principles to guide management:
- Use PSMA PET to define disease
- Most sensitive modality
- Detects more disease
- Closest to the “truth”
- Guides treatment strategy
- Biology is the ultimate driver
- Imaging is not equivalent to biology
- Tumor behavior drives outcomes
- Select patients carefully
- PSA doubling time is crucial
- Understand disease burden
- Personalize treatment intensity
- Escalate for high risk patients
- De-escalate in selected patients
- Balance benefit and harm
Presented by: Nicholas van As, The Royal Marsden NHS Foundation Trust, London, United Kingdom
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 Advanced Prostate Cancer Consensus Conference (APCCC), Lugano, Switzerland, Thurs, April 30 – Sat, May 2, 2026.
References:
- Freedland SJ, de Almeida Luz M, De Giorgi U, et al. Improved Outcomes with Enzalutamide in Biochemically Recurrent Prostate Cancer. N Engl J Med 2023 Oct 19;389(16):1453-1465.
- Aggarwal R, Heller G, Hillman DW, et al. PRESTO: A Phase III, Open-Label Study of Intensification of Androgen Blockade in Patients with High-Risk Biochemically Relapsed Castration-Sensitive Prostate Cancer (AFT-19). J Clin Oncol. 2024 Apr 1;42(10):1114-1123.
- Phillips R, Shi WY, Deek M, et al. Outcomes of Observation vs Stereotactic Ablative Radiation for Oligometastatic Prostate Cancer: The ORIOLE Phase 2 Randomized Clinical Trial. JAMA Oncol 2020 Mar 26;6(5):650-659.
- Yasar B, Chapman E, Taylor H, et al. Predictors of long-term disease-free survival with stereotactic body radiation therapy for oligometastatic prostate cancer. Int J Radiat Oncol Biol Phys. 2025 Nov 29 [Epub ahead of print].