(UroToday.com) The 2026 Advanced Prostate Cancer Consensus Conference (APCCC) meeting featured a management of metastatic hormone sensitive prostate cancer (mHSPC) session and a presentation by Dr. Piet Ost discussing the optimal management of synchronous oligometastatic hormone sensitive prostate cancer on PSMA PET. Dr. Ost notes that a patient presenting with synchronous oligometastatic hormone sensitive prostate cancer on PSMA PET forces three intertwined decisions:
- Pillar 1 – Systemic therapy: which intensity of ADT-based combination is appropriate, doublet, triplet, or ADT alone?
- Pillar 2: Local therapy of the prostate: does prostate radiotherapy remain indicated when the disease is seen only on PSMA PET?
- Pillar 3: Metastasis directed therapy: should stereotactic body radiotherapy be added to every PSMA PET visible metastasis?
PSMA PET reveals hidden low volume (oligometastatic) disease in “high risk M0” patients. Notably, in the THUNDER trial, 30% of high risk localized patients were upstaged on PSMA PET, 37% of STAMPEDE M0 eligible patients were upstaged on PSMA PET, and 19% were reclassified as miM1a-c, which are the hidden oligometastatic lesions. Overall, one in five “high risk M0” patients who drove the benefit signal in STAMPEDE M0 were, in fact, oligometastatic on PSMA PET. In THUNDER, 142 high risk prostate cancer patients will be treated with curative intent radiotherapy.
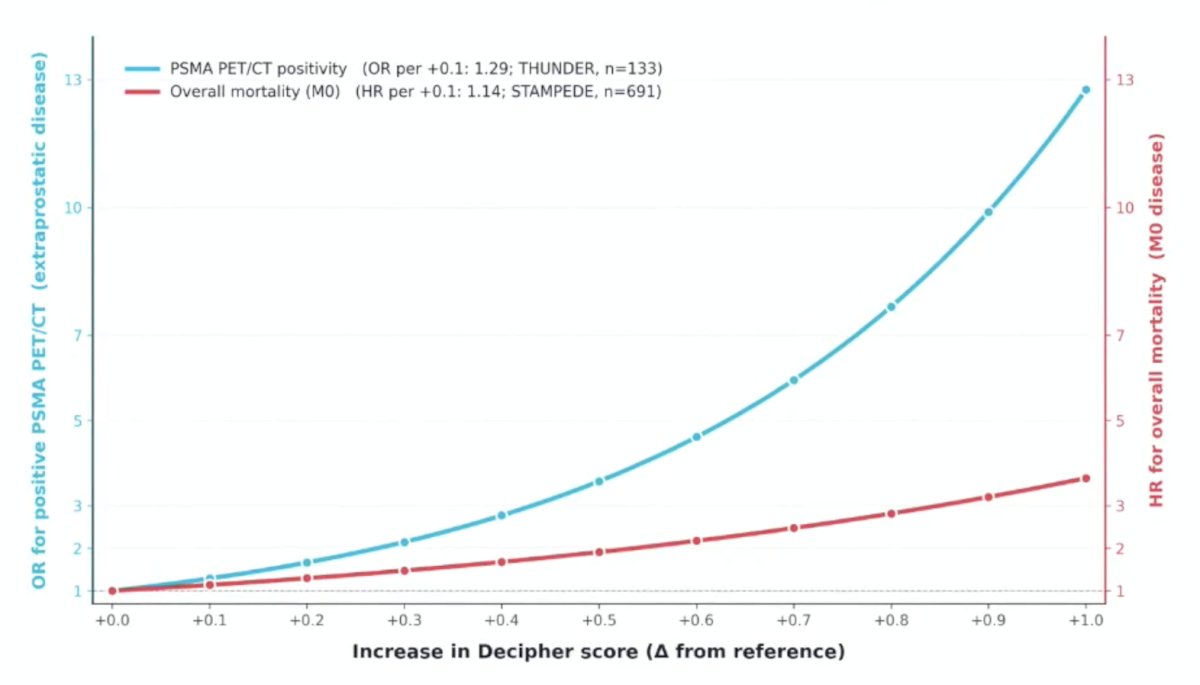
PSMA PET detected oligometastatic disease is biologically distinct. In THUNDER, there is a 29% increased odds of positive PSMA PET per +0.1 increase in Decipher score, with a +14% increased hazard for death per +0.1 increase in Decipher score in STAMPEDE:
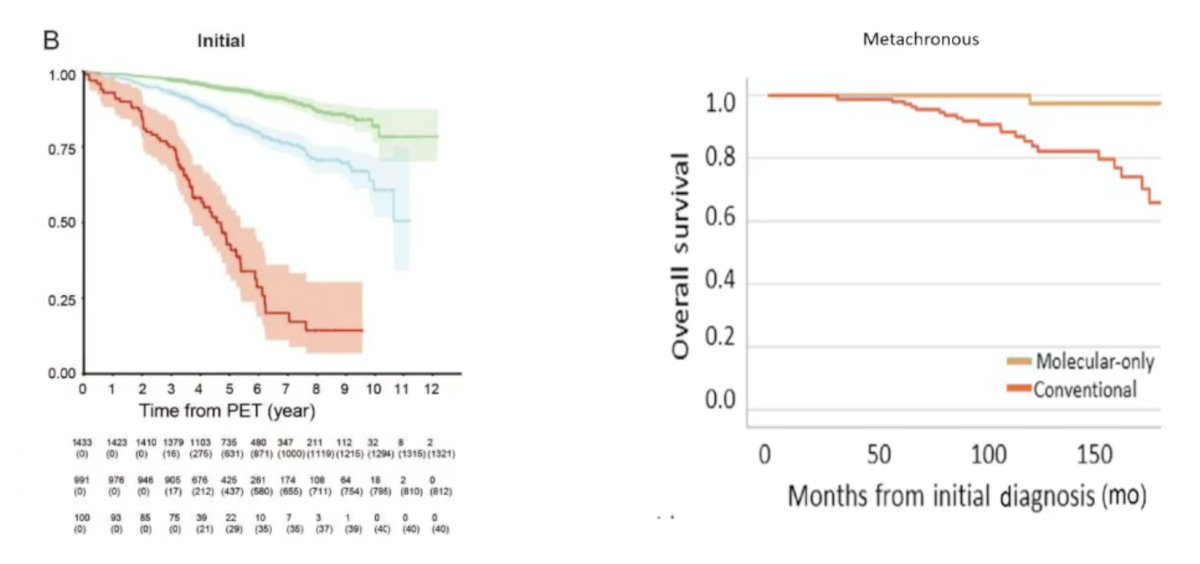
Based on the PPP3 prostate cancer risk groups, PSMA PET is a prognostic tool:1
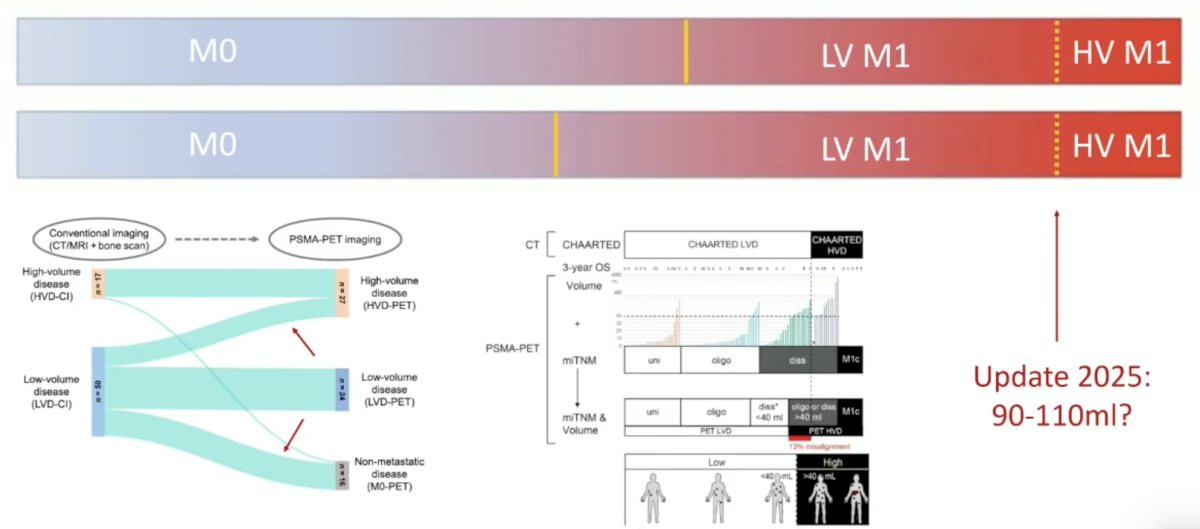
However, Dr. Ost notes that PSMA PET resets the goalposts, increasing the pool of low volume M1 disease patients and decreasing the pool of M0 patients:
For the first pillar of systemic therapy, Dr. Ost notes that landmark trials (M1 trials, STAMPEDE M0, and ENZARAD) are all conventionally staged. As such, the hypothesis is that the biggest benefit from androgen receptor pathway inhibitors/docetaxel in STAMPEDE M0 might be from patients with PSMA PET M+ (or Decipher high) disease. In ENZARAD, enzalutamide added to radiotherapy + ADT resulted in a 10 year metastasis free survival rate of 70% and 10 year overall survival rate of 75%. Dr. Ost estimates that 15% of these patients are PSMA PET positive. In STAMPEDE M0, abiraterone was added to radiotherapy + ADT, resulting in a 10 year metastasis free survival rate of 50% and 10 year overall survival rate of 50%.2 In this trial, Dr. Ost estimates a 37% PSMA PET positive rate amongst these patients. Perhaps androgen receptor pathway inhibitors/docetaxel are best suited for these higher risk, likely PSMA PET positive patients.
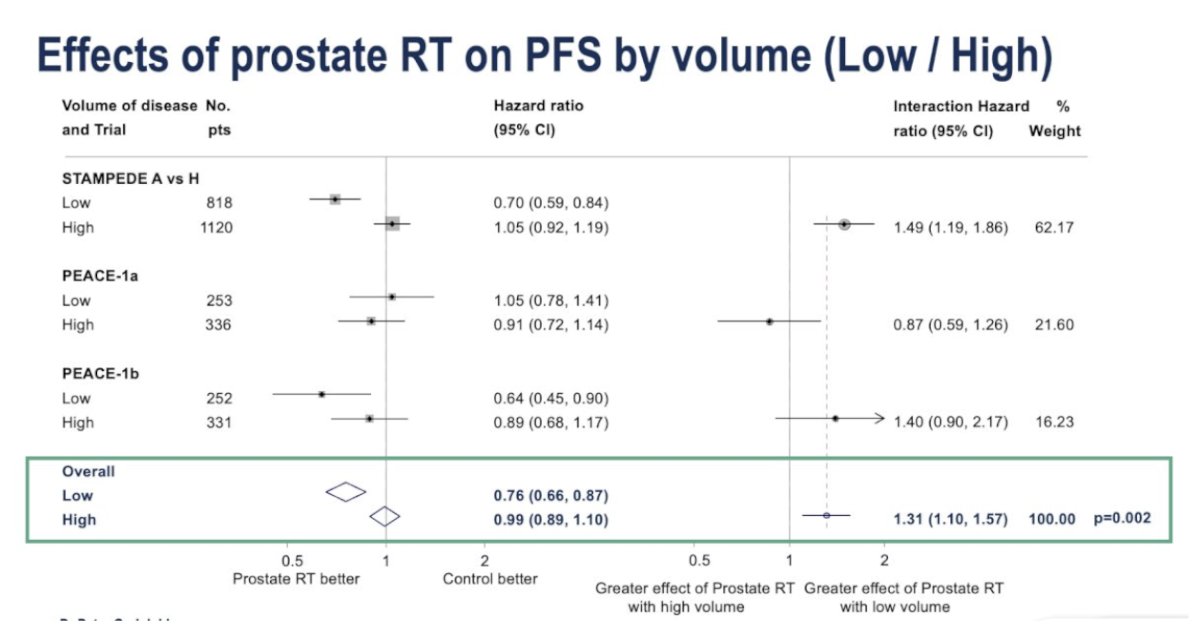
For the second pillar of prostate radiotherapy, the benefit spans from high risk prostate cancer to low volume metastatic prostate cancer. In the SPCG-7, MRC PR007, and STAMPEDE M0 trials, radiotherapy improved overall survival above ADT, with a >30% relative overall survival reduction. Low volume on PSMA PET is ~<40-110 mL. Furthermore, in the STOPCAP meta-analysis presented as ESMO 2025, when analyzed by disease volume, prostate radiotherapy significantly improved progression free survival in patients with low volume disease (HR 0.76, 95% CI 0.66–0.87), whereas no benefit was seen in those with high-volume disease (HR 0.99, 95% CI 0.89–1.10). The interaction p-value was 0.002, confirming a greater effect in low-volume cases:
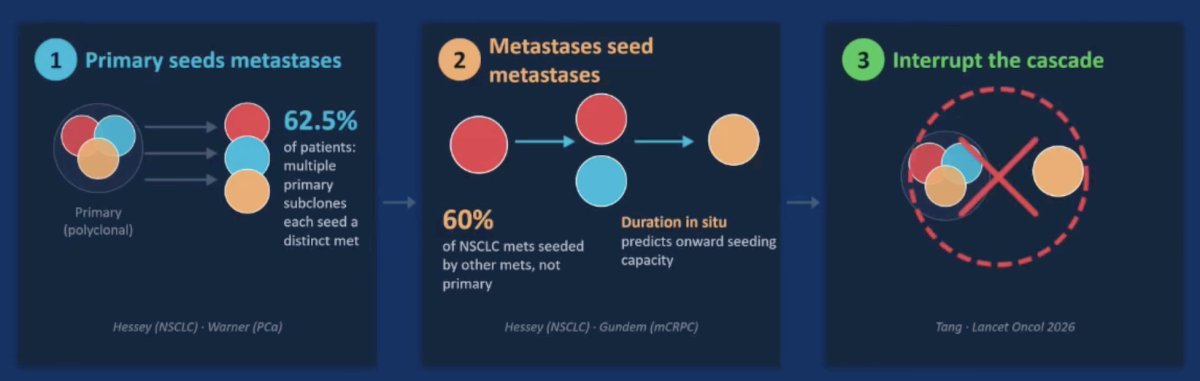
For the third pillar of metastasis directed therapy, there is a biological rationale for treating the primary tumor and metastasis directed therapy, whereby interrupting the metastatic cascade:
- The primary seeds the metastases
- Metastases seed metastases
- Metastasis directed therapy interrupts the cascade
Dr. Ost states that to date, there have been no completed phase III randomized clinical trials in synchronous disease. The WOLVERINE meta-analysis was published in early 20263 and amalgamated individual patient data across trials to evaluate the effectiveness of metastasis directed therapy for oligometastatic prostate cancer. Overall, 7 phase 2 trials (n = 574) were included in the analysis. There were 6 trials randomly assigning 472 patients to metastasis directed therapy + standard of care (n = 248) versus standard of care (n = 224) used to evaluate metastasis directed therapy, and had a median follow-up time of 40.7 months (IQR 25.6-53.7). Metastasis directed therapy was associated with improved progression free survival (trial level HR 0.44, 95% CI 0.35-0.56, p < 0.0001; patient level HR 0.45, 95% CI 0.35-0.57, p < 0.0001), radiographic progression free survival (trial level HR 0.60, 95% CI 0.42-0.85, p = 0.0039; patient level HR 0.59, 95% CI 0.46-0.76, p < 0.0001), and castration resistance free survival (trial level HR 0.58, 95% CI 0.37-0.92, p = 0.019; patient level HR 0.58, 95% CI 0.37-0.91, p = 0.017). The association between metastasis directed therapy and overall survival showed an HR of 0.63 (95% CI 0.39-1.00, p = 0.051) in trial level analyses and 0.64 (95% CI 0.40-1.01, p = 0.057) in patient level analyses.
STAMPEDE2 SABR is the definitive trial (n = 2,476) in synchronous disease, with a co-primary endpoint of radiographic progression free survival and overall survival, with the first patient enrolled in June 2024 and results expected sometime after 2028. Outside of a trial, metastasis directed therapy should still be considered investigational, and in 2026, offering stereotactic body radiotherapy to all PSMA PET-visible metastases outside of STAMPEDE2 extrapolates from metachronous data.
Taken together, Dr. Ost sees the treatment spectrum of synchronous PSMA PET oligometastatic disease as follows:

Dr. Ost concluded his presentation discussing the optimal management of synchronous oligometastatic hormone sensitive prostate cancer on PSMA PET with the following take-home points:
- PSMA PET-detected oligometastatic disease is biologically distinct (higher Gleason, higher Decipher score)
- Systematic intensification benefits those with the worst disease: ENZARAD was negative overall, but with a HR of 0.43 for N1; STAMPEDE M0, conventional imaging negative, and possibly PSMA PET positive
- Prostate radiotherapy works from high-risk M0 to low volume M1 (on conventional imaging): if it works for low volume on conventional imaging, it works for low volume on PSMA PET
- Metastasis directed therapy in synchronous disease is not yet evidence based: there have been no completed phase III randomized clinical trials. Thus, patients should be enrolled in STAMPEDE2, since the evidence gap is real and must be filled
Presented by: Piet Ost, MD, PhD, Iridium Netwerk, Wilrijk, Belgium
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 Advanced Prostate Cancer Consensus Conference (APCCC), Lugano, Switzerland, Thurs, April 30 – Sat, May 2, 2026.
References:
- Karpinski MJ, Civan C, Rauschner I, et al. New prostate cancer risk groups by PSMA-PET (PPP3): An international, retrospective, registry-based cohort study. Lancet Oncol. 2026 Apr;27(4):480-490.
- Attard G, Murphy L, Clarke NW, et al. Abiraterone acetate and prednisolone with or without enzalutamide for high-risk non-metastatic prostate cancer: A meta-analysis of primary results from two randomized controlled phase 3 trials of the STAMPEDE platform protocol. Lancet 2022 Jan 29;399(10323):447-460.
- Tang C, Sherry AD, Hwang H, et al. Metastasis-directed therapy and standard of care versus standard of care for oligometastatic prostate cancer (WOLVERINE): A systematic review and individual patient data meta-analysis from the X-MET collaboration. Lancet Oncol. 2026 Feb;27(2):181-190.