(UroToday.com) The 2026 Advanced Prostate Cancer Consensus Conference (APCCC) meeting featured a treatment of PSA recurrence session and a presentation by Dr. Daniel Spratt discussing whether there are patients with PSA recurrence who do not need imaging and treatment.
Dr. Spratt notes that there are two forces pulling post-radical prostatectomy biochemical recurrence management in opposite directions:
- Intensifying treatment: the push to escalate
- PSMA-PET detects disease at PSA 0.2–0.5 ng/mL — where conventional imaging is blind
- EMBARK1 showed a metastasis-free survival benefit for the androgen receptor pathway inhibitor for men with high-risk biochemical recurrence (PSA doubling time ≤9 months)
- RTOG 96012 established a survival benefit for long-term hormone therapy + secondary radiotherapy in defined subsets
- Decipher identifies high-risk biology even in otherwise favorable disease
- The natural history is long — median 8 years from biochemical recurrence to metastasis, 5 more years to death3
- Most biochemical recurrence patients die with prostate cancer, not of prostate cancer — especially with PSA doubling times ≥15 months4
- Postoperative radiation carries some risk (far less than ADT)
- ADT/androgen receptor pathway inhibitors carry real harm — cardiovascular, metabolic, bone, cognitive, and quality of life
- Detection ≠ benefit — finding an avid lesion does not mean treating it improves survival
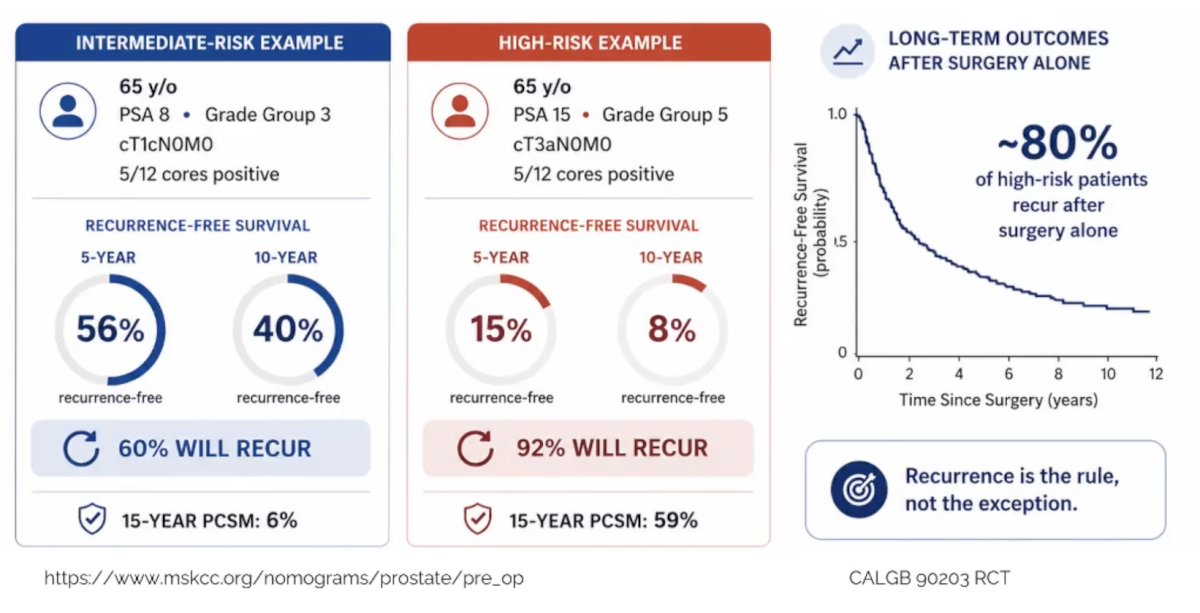
Based on data from the CALGB 90203 trial,5 Dr. Spratt notes that biochemical recurrence is common after radical prostatectomy, as illustrated in the following MSKCC clinical nomogram:
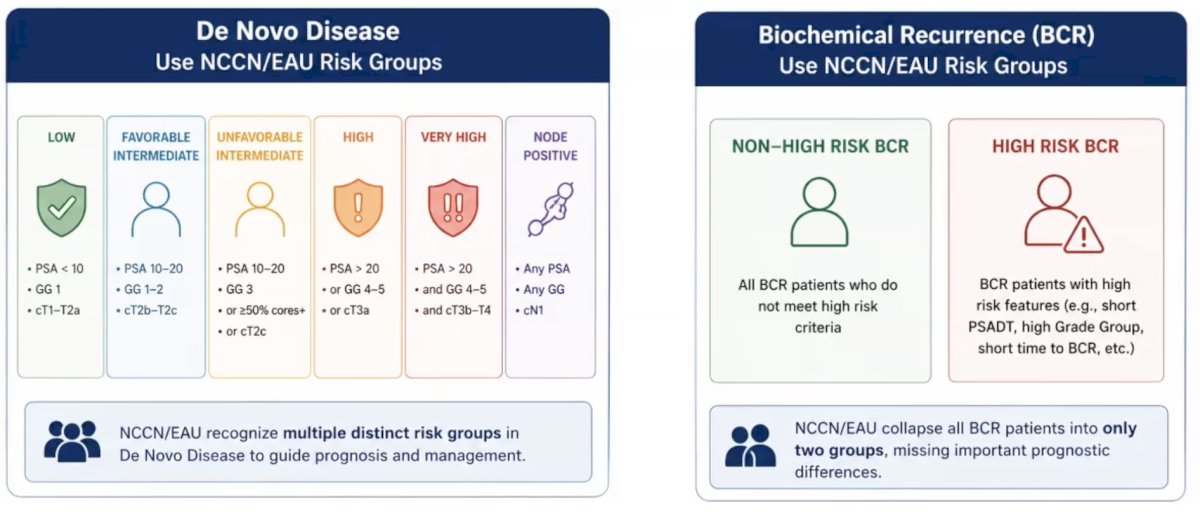
As such, there are several important challenges to acknowledge. Challenge #1 is that there is insufficient risk stratification for biochemical recurrence. For de novo disease, the NCCN/EAU recognizes multiple distinct risk groups to guide prognosis and management. For biochemical recurrence, the NCCN/EAU collapses all biochemical recurrence patients into only two groups, missing important prognostic differences:
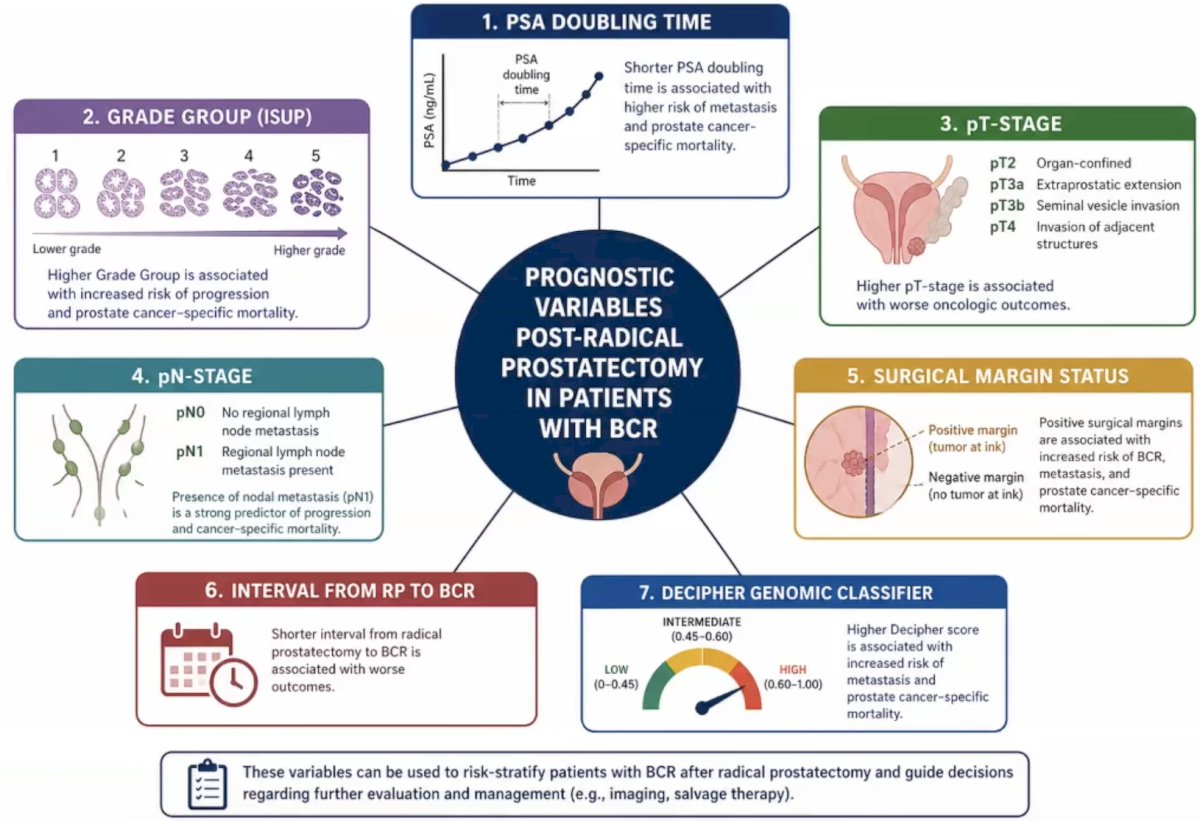
Prognostic variables in patients post radical prostatectomy with biochemical recurrence include (i) PSA doubling time, (ii) grade group, (iii) pT stage, (iv) pN stage, (v) surgical margin status, (vi) the interval from radical prostatectomy to biochemical recurrence, and (vii) Decipher Genomic Classifier:
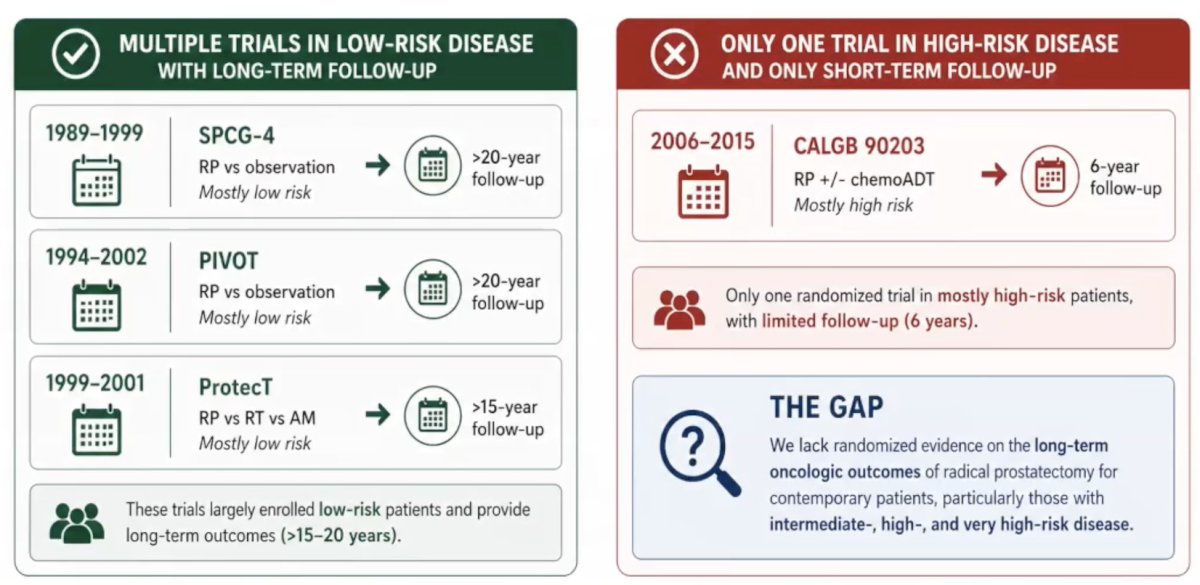
Challenge #2 is that there is a lack of contemporary randomized clinical trials of surgery in non-low-risk patients with long-term data. There are multiple trials in low-risk disease (with long-term follow-up), but only one trial in high-risk disease (and short-term follow-up):
Data from the Hopkins natural history of biochemical recurrence cohort6 suggests that many biochemical recurrences can be safely monitored:

Three variables predicted metastasis (and thus death):
- PSA doubling time: <10 months versus >= 10 months
- Pathologic Gleason score: <= 7 versus 8-10
- Time from radical prostatectomy to biochemical recurrence: <= 2 years versus >2 years
The bottom line is that patients with favorable risk biochemical recurrence (Gleason <= 7, late recurrence, PSA doubling > 10 months) have an 82% metastasis free rate at 7 years with no treatment. Dr. Spratt notes that biochemical recurrence is common, but a single label hides widely different diseases:7
![The bottom line is that patients with favorable risk biochemical recurrence (Gleason <= 7, late recurrence, PSA doubling > 10 months) have an 82% metastasis free rate at 7 years with no treatment. Dr. Spratt notes that biochemical recurrence is common, but a single label hides widely different diseases [7]:](/images/com-doc-importer/262-apccc-2026/apccc-2026-are-there-patients-with-psa-recurrence-who-do-not-need-imaging-and-treatment/image-5.jpg)
It is important to remember that this study is from patients from 1982-2000; thus, there was a markedly different grading system, and PSA screening was not routine for all patients. Even after metastasis, the survival tail is long.8 The median failure time from radical prostatectomy to PSA failure is 2 years, from PSA failure to metastasis is 2.7 years, from metastasis to death is 6.8 years, and from radical prostatectomy to death is 14.0 years:
![It is important to remember that this study is from patients from 1982-2000; thus there was a markedly different grading system, and PSA screening was not routine for all patients. Even after metastasis, the survival tail is long [8]. The median failure time from radical prostatectomy to PSA failure is 2 years, from PSA failure to metastasis is 2.7 years, from metastasis to death is 6.8 years, and from radical prostatectomy to death is 14.0 years:](/images/com-doc-importer/262-apccc-2026/apccc-2026-are-there-patients-with-psa-recurrence-who-do-not-need-imaging-and-treatment/image-6.jpg)
Two variables identified men who did well despite metastasis: absence of pain at metastasis and PSA doubling time >= 3 months before metastasis.
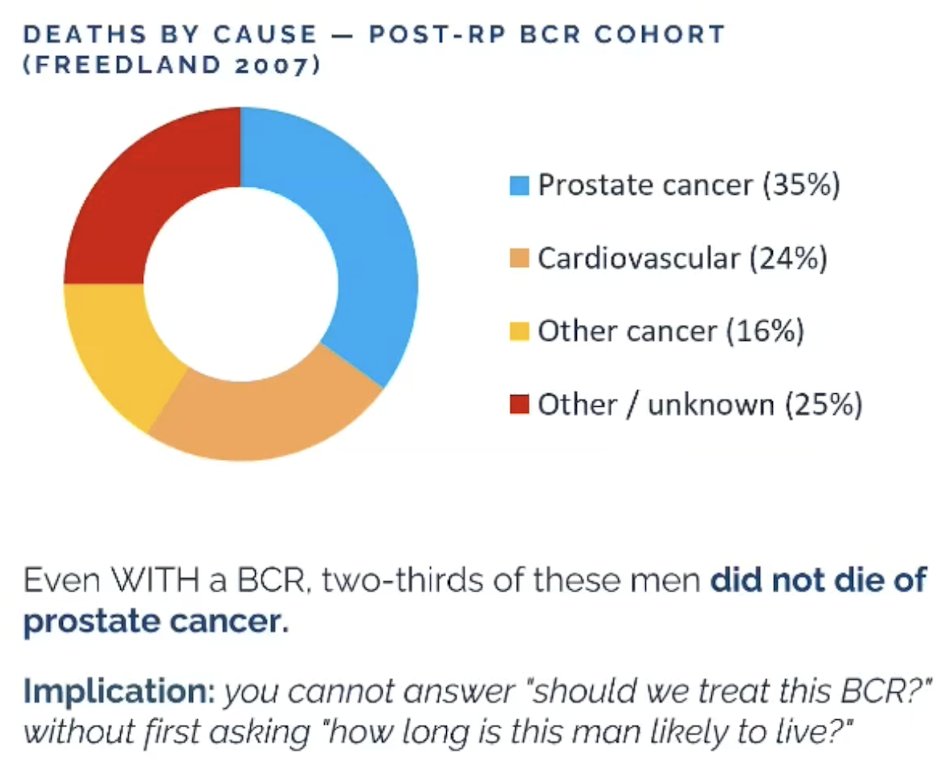
Dr. Spratt emphasized that life expectancy is the other key variable, given that biochemical recurrence outcomes only matter if the patient lives long enough to experience them. Even with biochemical recurrence, 2/3 of men do not die from prostate cancer:4
There are many validated tools for estimating life expectancy at the bedside, including (i) SSA Actuarial Tables, (ii) Lee Index, (iii) MSKCC Nomogram, (iv) NCCN-Adjusted LE, (v) Schonberg Index, and (vi) ePrognosis (UCSF).
So, who can we not image (PSMA PET/CT)?
- Anyone who does not need treatment: driven by the balance of life expectancy and prognostic risk
- Pre-test probability of meaningful change in outcomes: number needed to test <10-15
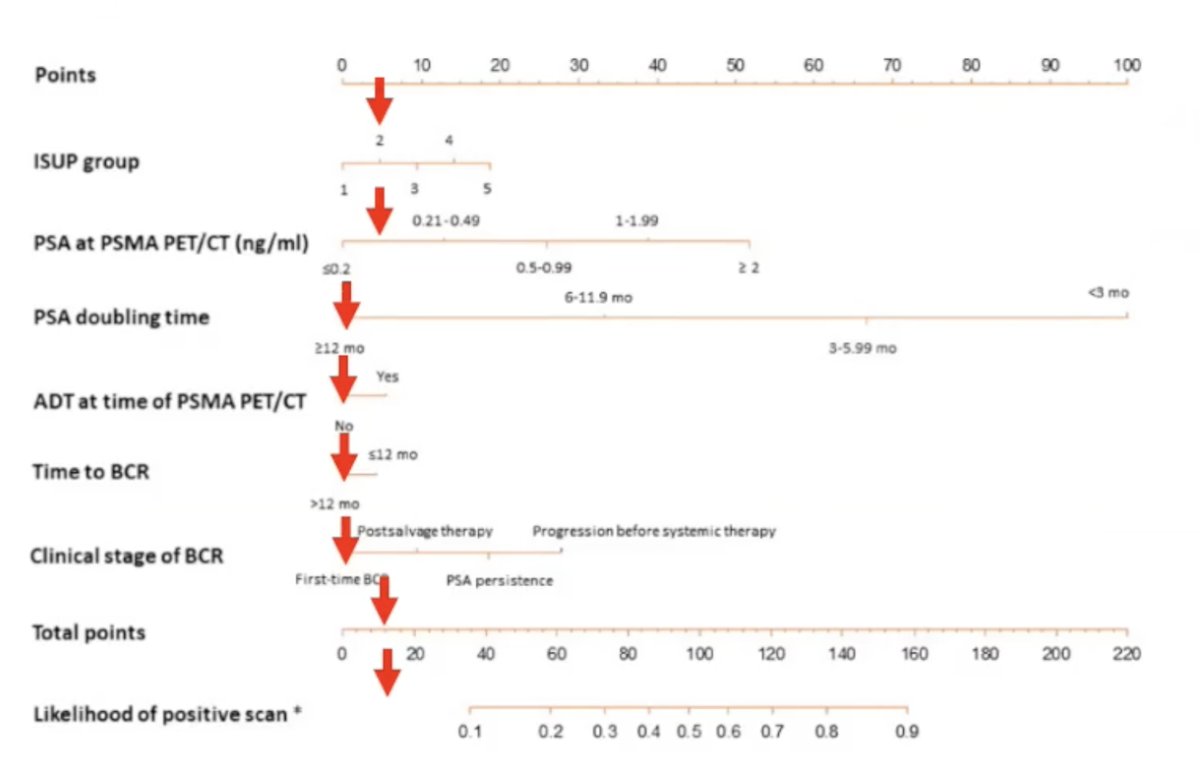
Based on data from Bianchi et al.,9 patients who may avoid PSMA PET/CT imaging include those with Gleason Grade Group 2 disease, PSA 0.2 ng/mL, PSA doubling time > 12 months, and time to biochemical recurrence >12 months. From this validated nomogram, there is a <5% chance of a positive scan assuming no interaction effects. Approximately 2.5% or a number needed to treat of 40 would change management:
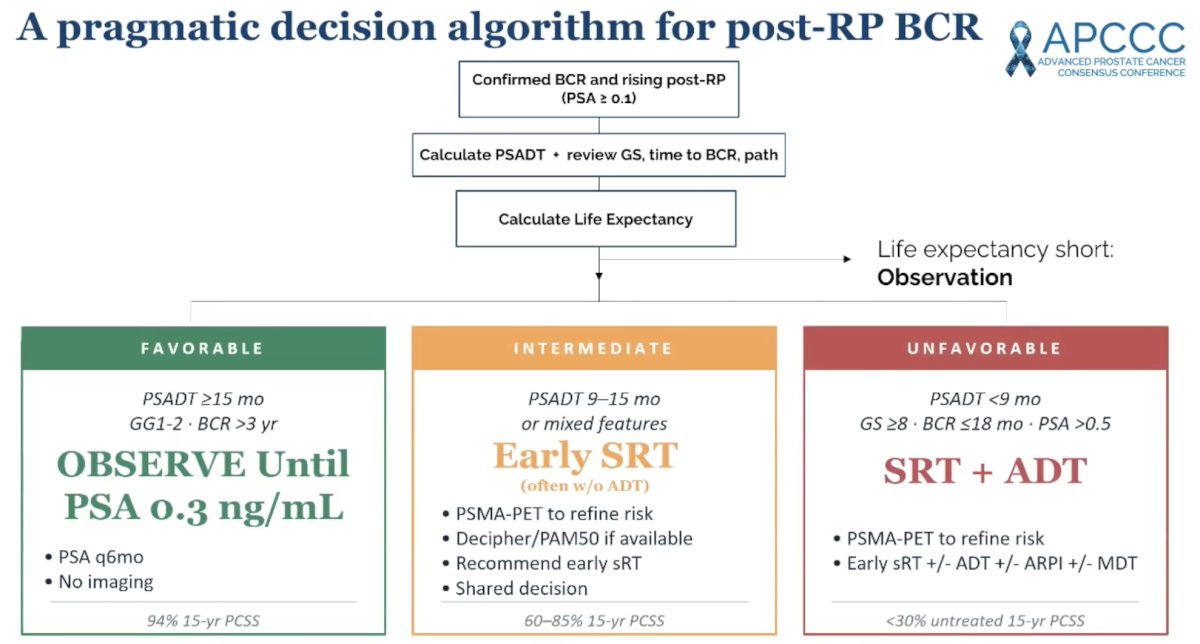
Dr. Spratt concluded his presentation discussing whether there are patients with PSA recurrence who do not need imaging and treatment with a pragmatic decision algorithm for post-radical prostatectomy biochemical recurrence:
Presented by: Daniel Spratt, MD, Chair and Professor of Radiation Oncology, UH Cleveland Medical Center, Seidman Cancer Center, Case Western Reserve University School of Medicine, Cleveland, OH
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 Advanced Prostate Cancer Consensus Conference (APCCC), Lugano, Switzerland, Thurs, April 30 – Sat, May 2, 2026.
- Freedland SJ, de Almeida Luz M, De Giorgi U, et al. Improved Outcomes with Enzalutamide in Biochemically Recurrent Prostate Cancer. N Engl J Med 2023 Oct 19;389(16):1453-1465.
- Shipley WU, Seiferheld W, Lukka HR, et al. Radiation with or without Antiandrogen Therapy in Recurrent Prostate Cancer. N Engl J Med 2017;376(5):417-428.
- Pound CR, Partin AW, Eisenberger MA, Chan DW, Pearson JD, Walsh PC. Natural history of progression after PSA elevation following radical prostatectomy. JAMA 1999 May 5;281(17):1591-1597.
- Freedland SJ, Humphreys EB, Mangold LA, et al. Death in patients with recurrent prostate cancer after radical prostatectomy: prostate-specific antigen doubling time subgroups and their associated contributions to all-cause mortality. J Clin Oncol. 2007 May 1;25(13):1765-1771.
- Eastham JA, Heller G, Halabi S, et al. Cancer and Leukemia Group B 90203 (Alliance): Radical Prostatectomy With or Without Neoadjuvant Chemohormonal Therapy in Localized, High-Risk Prostate Cancer. J Clin Oncol. 2020 Sep 10;38(26)3042-3050.
- Pound CR, Partin AW, Eisenberger MA, Chan DW, Pearson JD, Walsh PC. Natural history of progression after PSA elevation following radical prostatectomy. JAMA 1999 May 5;281(17):1591-1597.
- Freedland SJ, Humphreys EB, Mangold LA, et al. Risk of prostate cancer-specific mortality following biochemical recurrence after radical prostatectomy. JAMA. 2005 Jul 27;294(4):433-439.
- Makarov DV, Humphreys EB, Mangold LA, et al. The natural history of men treated with deferred androgen deprivation therapy in whom metastatic prostate cancer developed following radical prostatectomy. J Urol. 2008 Jan;179(1):156-161.
- Bianchi L, Castellucci P, Farolfi A, et al. Multicenter external validation of a nomogram for predicting positive prostate-specific membrane antigen/positron emission tomography scan in patients with prostate cancer recurrence. Eur Urol Oncol. 2023 Feb;6(1):41-48.