(UroToday.com) The 2026 Advanced Prostate Cancer Consensus Conference (APCCC) meeting featured a treatment of PSA recurrence session and a presentation by Dr. Kosj Yamoah discussing in which patients metastases directed therapy without systemic therapy is sufficient.
There are several important definitions to clarify in this disease space when considering the utilization of metastasis-directed therapy:
- Oligometastatic hormone-sensitive prostate cancer: de novo synchronous oligometastatic hormone-sensitive prostate cancer, with a metastatic burden <= 5 lesions
- Oligorecurrent hormone-sensitive prostate cancer: metachronous oligorecurrent hormone-sensitive prostate cancer, with a metastatic burden <= 5 lesions
- Oligoprogressive castration resistant prostate cancer: oligoprogressive castration resistant prostate cancer, with a metastatic burden <= 5 lesions
With regards to NCCN definitions, metastasis-directed therapy is preferred for metachronous or oligorecurrent hormone-sensitive prostate cancer. Metastasis-directed therapy is “acceptable based on clinical and medical need” for synchronous oligometastatic hormone-sensitive prostate cancer and for oligoprogressive castration resistant prostate cancer. Metastasis-directed therapy alone is “not suitable” for synchronous oligometastatic hormone-sensitive prostate cancer, rather systemic therapy (most commonly ADT + androgen receptor pathway inhibitor) and treatment of the primary tumor with radiotherapy is recommended for most patients, with metastasis-directed therapy added in select cases.
Dr. Yamoah first discussed the STOMP trial,1 which provided the first phase 2 randomized evidence that metastasis-directed therapy can safely delay systemic therapy initiation in oligometastatic hormone-sensitive prostate cancer. In STOMP, 68 patients with up to 3 extracranial sites were randomly assigned (1:1) to either surveillance or metastasis-directed therapy of all detected lesions. The primary endpoint was ADT-free survival. The 5-year ADT-free survival was 8% for the surveillance group and 34% for the metastasis-directed therapy group. The ORIOLE trial2 was a phase 2 randomized clinical trial that demonstrated stereotactic body radiotherapy significantly improved progression-free survival compared to observation in men with oligometastatic hormone-sensitive prostate cancer. ORIOLE enrolled 54 men with 1-3 metastases detected by conventional imaging, randomizing them 2:1 to receive stereotactic body radiotherapy versus observation. At 6 months, progression was noted in 19% of patients receiving stereotactic body radiotherapy compared to 61% in the observation arm.
Other studies supporting stereotactic body radiotherapy for metachronous oligometastatic hormone-sensitive prostate cancer include the SABR-COMET trial.3 This trial included patients with 1-5 metastatic lesions, with all metastases amenable to stereotactic body radiotherapy. Of the 99 patients enrolled, 16 were prostate cancer patients, demonstrating an improved overall survival for those receiving stereotactic body radiotherapy. The EXTEND trial compared was a phase II trial comparing metastasis-directed therapy to intermittent ADT for oligometastatic hormone-sensitive prostate cancer. Among 87 patients, the median progressive free survival time for all patients was 22.4 months (15.8 months for those receiving ADT alone, and not reached for those receiving radiotherapy + ADT). This resulted in a progression of disease rate of 30% for those receiving metastasis-directed therapy + ADT versus 64% for those receiving ADT monotherapy. The RADIOSA trial5 was a phase 2, single-center trial among patients with biochemical progression after local treatment – either nodal relapse or bone metastasis (maximum 3 lesions). Patients received stereotactic body radiotherapy (30 Gy/3fx daily) +/- ADT for 6 months. The median progression-free survival was 15.1 months (95% CI 12.4-22.8) versus 32.2 months (22.4 – not reached) for the stereotactic body radiotherapy + ADT group:
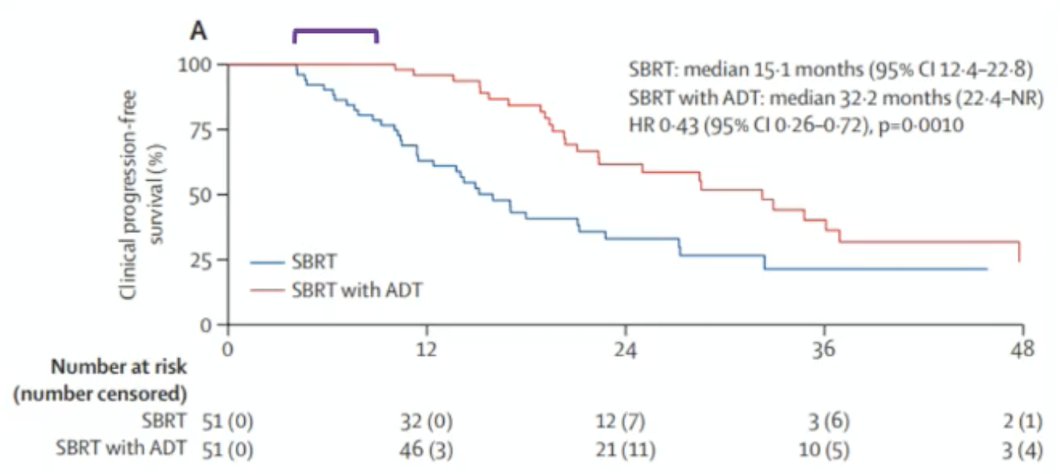
Dr. Yamoah notes that it is interesting that patients with <= 43 months from the time of first curative treatment to radiotherapy had a significantly improved progression-free survival (HR 0.34, 95% CI 0.17-0.68), whereas those >43 months (HR 0.55, 95% CI 0.25-1.24) did not, suggesting early metastasis-directed therapy is beneficial.
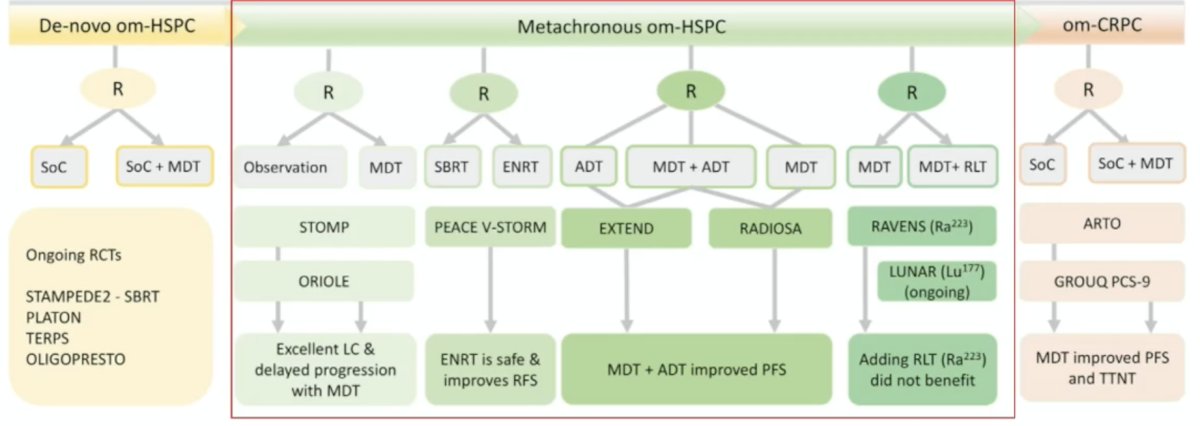
The following table summarizes the treatment landscape of metastasis-directed therapy in oligometastatic prostate cancer:
The WOLVERINE meta-analysis was published in early 20266 and amalgamated individual patient data across trials to evaluate the effectiveness of metastasis-directed therapy for oligometastatic prostate cancer. Overall, 7 phase 2 trials (n = 574) were included in the analysis. There were 6 trials randomly assigning 472 patients to metastasis-directed therapy + standard of care (n = 248) versus standard of care (n = 224) used to evaluate metastasis-directed therapy, and had a median follow-up time of 40.7 months (IQR 25.6-53.7). Metastasis directed therapy was associated with improved progression free survival (trial level HR 0.44, 95% CI 0.35-0.56, p < 0.0001; patient level HR 0.45, 95% CI 0.35-0.57, p < 0.0001), radiographic progression free survival (trial level HR 0.60, 95% CI 0.42-0.85, p = 0.0039; patient level HR 0.59, 95% CI 0.46-0.76, p < 0.0001), and castration resistance free survival (trial level HR 0.58, 95% CI 0.37-0.92, p = 0.019; patient level HR 0.58, 95% CI 0.37-0.91, p = 0.017). The association between metastasis-directed therapy and overall survival showed an HR of 0.63 (95% CI 0.39-1.00, p = 0.051) in trial-level analyses and 0.64 (95% CI 0.40-1.01, p = 0.057) in patient-level analyses.
There are several ongoing trials of note in this disease space:
- DART (NCT04641078): stereotactic body radiotherapy ± short-term darolutamide in extending metastasis-free survival
- SPARKLE: randomized in a 1:1:1 allocation ratio between arm A: metastasis-directed therapy alone, arm B: metastasis-directed therapy with 1 month ADT, or arm C: metastasis-directed therapy with 6 months ADT together with an androgen receptor pathway inhibitor (enzalutamide 4 × 40 mg daily) for 6 months
- Promethean (NCT05053152): stereotactic body radiotherapy ± relugolix
- NCT04599686: randomized in a 1:1 ratio between arm A (ADT only) and arm B (stereotactic body radiotherapy for oligometastases only)
Dr. Yamoah also provided the following points for patient selection criteria for metastasis-directed therapy alone:
- Disease characteristics:
- Oligometastatic prostate cancer is defined as <= 5 metastatic sites by CT/MRI/bone scan, or <= 10 sites if PSMA PET is used
- The metastases are typically limited to the lymph nodes and osseous sites
- Visceral organ involvement is an exclusion for metastasis-directed therapy alone
- Disease state: metachronous or oligorecurrent hormone-sensitive prostate cancer
- Limitations include:
- Metastasis-directed therapy should not be used without systemic therapies for:
- Oligoprogressive castration resistant prostate cancer, and should be used in combination with ADT + androgen receptor pathway inhibitor
- Synchronous oligometastatic hormone-sensitive prostate cancer, and should be used in combination with ADT + androgen receptor pathway inhibitor + radiotherapy to the prostate +/- metastasis directed therapy in select cases
- Metastasis-directed therapy should not be used without systemic therapies for:
Dr. Yamoah concluded his presentation discussing in which patients metastases-directed therapy without systemic therapy is sufficient, with the following take-home points:
- Biochemical (PSA), metabolic (PSMA-PET), and genomic (high-risk mutations) factors are emerging as key determinants for metastases-directed therapy-guided strategies in oligometastatic prostate cancer
- Longer PSA doubling time may help identify candidates for metastasis-directed therapy alone. Patients with a short doubling time (<3 months) require systemic therapies
- Patients with tumors harboring a high-risk genomic mutation (TP53, ATM, BRCA1/2, RB1) progress very fast with metastases-directed therapy alone and require systemic therapy (RAVENS7)
Presented by: Kosj Yamoah, MD, PhD, Radiation Oncologist & Chair, Department of Radiation Oncology, Moffitt Cancer Center & Research Institute, Tampa, FL
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 Advanced Prostate Cancer Consensus Conference (APCCC), Lugano, Switzerland, Thurs, April 30 – Sat, May 2, 2026.
- Ost P, Reynders D, Decaestecker K, et al. Surveillance of metastasis-directed therapy for oligometastatic cancer recurrence: A prospective, randomized, multicenter phase II trial. J Clin Oncol. 2018 Feb 10;36(5):446-453.
- Phillips R, Shi WY, Deek M, et al. Outcomes of Observation vs Stereotactic Ablative Radiation for Oligometastatic Prostate Cancer: The ORIOLE Phase 2 Randomized Clinical Trial. JAMA Oncol 2020 Mar 26;6(5):650-659.
- Palma DA, Olson R, Harrow S, et al. Stereotactic ablative radiotherapy versus standard of care palliative treatment in patients with oligometastatic cancers (SABR-COMET): A randomized, phase 2, open-label trial. Lancet. 2019 May 18;393(10185):2051-2058.
- Tang C, Sherry AD, Haymaker C, et al. Addition of metastasis-directed therapy to intermittent hormone therapy for oligometastatic prostate cancer: The EXTEND phase 2 randomized clinical trial. JAMA Oncol. 2023 Jun 1;9(6):825-834.
- Marvaso G, Corrao G, Zaffaroni M, et al. ADT with SBRT versus SBRT alone for hormone-sensitive oligorecurrent prostate cancer (RADIOSA): A randomized, open-label, phase 2 clinical trial. Lancet Oncol. 2025 Mar;26(3):300-311.
- Tang C, Sherry AD, Hwang H, et al. Metastasis-directed therapy and standard of care versus standard of care for oligometastatic prostate cancer (WOLVERINE): A systematic review and individual patient data meta-analysis from the X-MET collaboration. Lancet Oncol. 2026 Feb;27(2):181-190.
- Wang JH, Sherry AD, Bazyar S, et al. Outcomes of Radium-223 and Stereotactic Ablative Radiotherapy versus Stereotactic Ablative Radiotherapy for Oligometastatic Prostate Cancers: The RAVENS Phase II Randomized Trial. J Clin Oncol. 2025 Jun 20;43(18):2059-2068.