(UroToday.com) The 2026 Advanced Prostate Cancer Consensus Conference (APCCC) meeting featured a treatment of PSA recurrence or persistence session and a presentation by Dr. Jochen Walz discussing how to react to PSA persistence or recurrence after radical prostatectomy. Dr. Walz emphasized that it is important to understand PSA kinetics after radical prostatectomy, given that the total PSA half-life is 2.7-3.3 days, and depending on PSA levels preoperatively, there may be a 2-3 fold PSA increase during surgery. Based on this half-life, the PSA should be undetectable after 6 weeks.
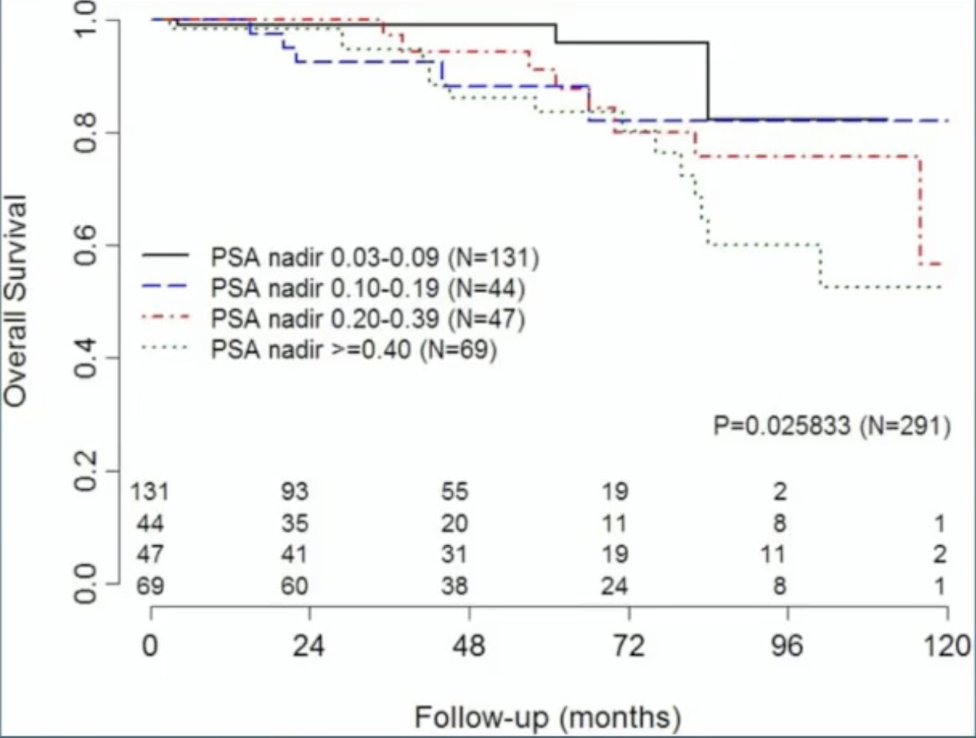
A persistent PSA is defined as at least 0.1 ng/mL for at least 6 weeks after surgery. Possible sources for a persistent PSA after surgery include (i) nodal or distant metastasis, (ii) local persistent prostate cancer, and (iii) local persistent benign tissue. Overall, the PSA remains detectable in 3-12% of patients after surgery. Data from Moreira and colleagues from 20091 in the US Veterans Affairs medical system suggests that overall survival is relative to the PSA nadir after surgery:
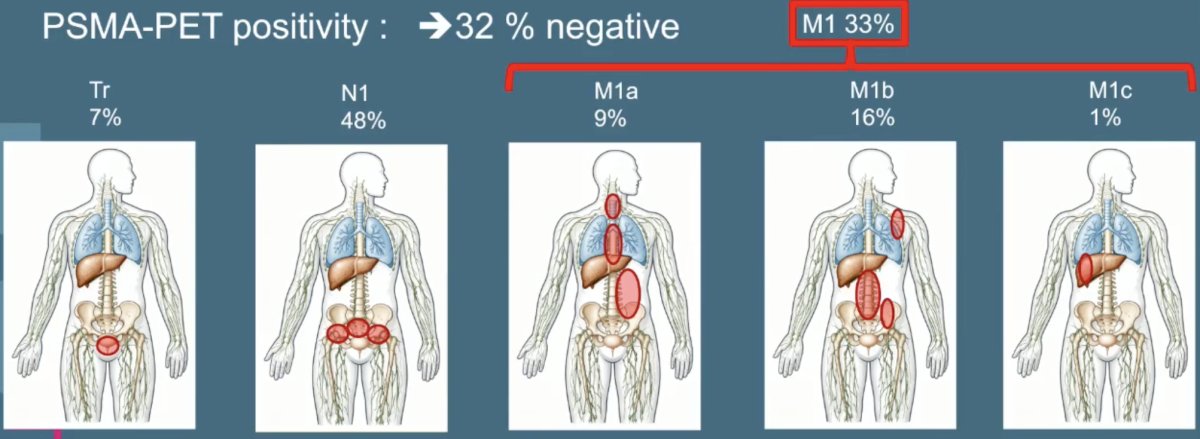
In 2019, Farolfi et al.2 assessed the ability of 68Ga-PSMA-11 PET to detect residual prostate cancer after prostatectomy. Among 191 patients, PSMA PET localized prostate cancer in 130 of 191 patients (68%) with PSA persistence at a median PSA of 1.1 ng/ml. The most frequently affected nodal regions were the obturator in 42% and the presacral/mesorectal region in 40%; 33% were M1 based on PET findings:
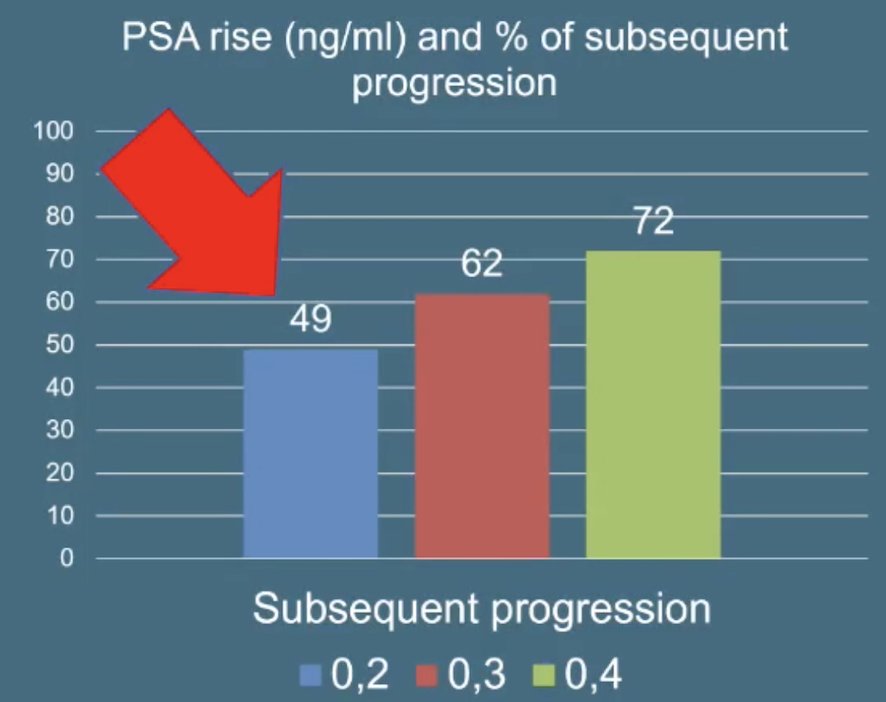
Although the definition of biochemical recurrence after radical prostatectomy is a rising PSA after a PSA has been undetectable (< 0.1 ng/mL) after radical prostatectomy, a PSA > 0.4 ng/mL best correlates with progression:
Do we need to treat everybody with biochemical recurrence? Based on the natural history of untreated biochemical recurrence-free survival, there is a median overall survival of 15.5 years from radical prostatectomy to death,3-4 suggesting that many patients do not need treatment:
![Do we need to treat everybody with biochemical recurrence? Based on the natural history of untreated biochemical recurrence-free survival, there is a median overall survival of 15.5 years from radical prostatectomy to death [3-4], suggesting that many patients do not need treatment:](/images/com-doc-importer/262-apccc-2026/apccc-2026-psa-persistence-or-recurrence-after-radical-prostatectomy---when-and-how-to-react/image-3.jpg)
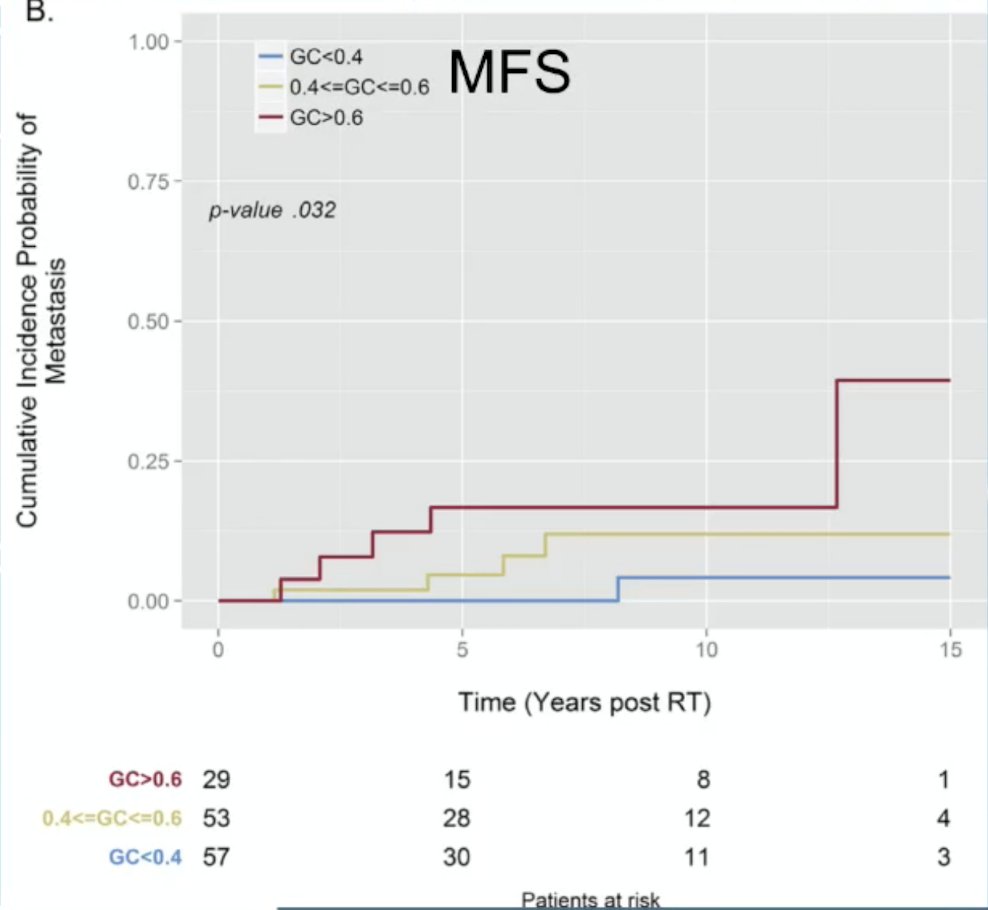
What are the risk factors for progression among patients with biochemical recurrence? There are several cancer characteristics in favor of progression, including pT3, pN+, and radical prostatectomy Gleason Group >= 4. Genomic classifiers may also be useful in determining the risk of metastasis among patients with biochemical recurrence:
Dr. Walz notes that PSA doubling time among patients with biochemical recurrence is also useful in delineating who may be at risk of progression. In 2019, Markowski et al.5 investigated the association of PSA value with metastasis-free survival in men with biochemical recurrence and a PSA doubling time < 12 months. Metastasis occurred in 250 of 656 patients with biochemical recurrence (median follow-up, 5 years). A PSA doubling time < 7.5 months and a Gleason score were independent risk factors for distant metastasis in multivariable analysis. Risk of metastasis increased for PSA doubling time of 6.01 to 7.50, 4.51 to 6.0, 3.01 to 4.50, and ≤ 3.0 months, after adjusting for Gleason score:
![Dr. Walz notes that PSA doubling time among patients with biochemical recurrence is also useful in delineating who may be at risk of progression. In 2019, Markowski et al. [5] investigated the association of PSA value with metastasis-free survival in men with biochemical recurrence and a PSA doubling time < 12 months. Metastasis occurred in 250 of 656 patients with biochemical recurrence (median follow-up, 5 years). A PSA doubling time < 7.5 months and a Gleason score were independent risk factors for distant metastasis in multivariable analysis. Risk of metastasis increased for PSA doubling time of 6.01 to 7.50, 4.51 to 6.0, 3.01 to 4.50, and ≤ 3.0 months, after adjusting for Gleason score:](/images/com-doc-importer/262-apccc-2026/apccc-2026-psa-persistence-or-recurrence-after-radical-prostatectomy---when-and-how-to-react/image-5.jpg)
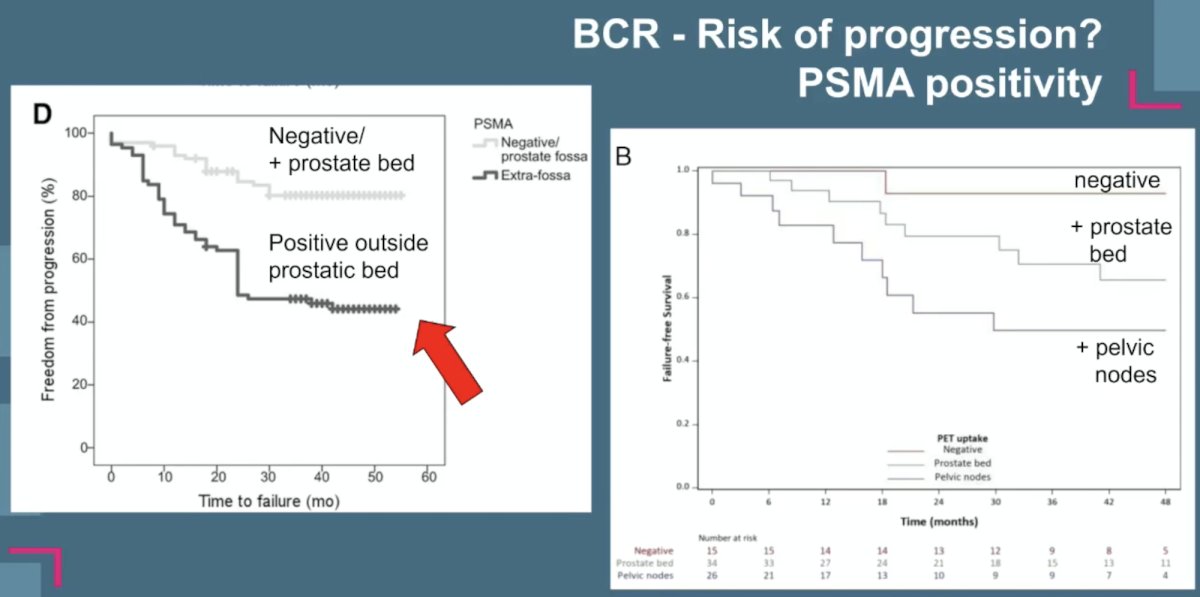
Dr. Walz notes that the EAU risk groups can also assist with predicting progression among patients with biochemical recurrence. Patients at low risk after radical prostatectomy include those with a PSA doubling time > 12 months + pathologic Grade Group < 4, whereas those at high risk after radical prostatectomy include patients with a PSA doubling time < 12 months +/- pathologic Grade Group 4-5 disease. Certainly, PSMA PET/CT is also helpful in these patients, with patients having a recurrence outside of the prostatic bed having worse outcomes compared to those with a negative PSMA PET/CT, and patients with positive lymph nodes on PSMA PET having worse outcomes compared to those with positive disease in the prostate bed:
Dr. Walz concluded his presentation discussing how to react to PSA persistence or recurrence after radical prostatectomy with the following take-home points:
- PSA persistence is associated with poor outcomes, and postoperative treatment is indicated
- Biochemical recurrence remains a heterogeneous clinical scenario
- Before treatment, estimate life expectancy and cancer potential for progression
- Offer monitoring in patients with a low risk of progression
- Very early salvage treatment is most effective
- Better risk stratification and treatment selection are necessary
Presented by: Jochen Walz, MD, Associate Professor in Urology, Head of the Department of Urology, Institut Paoli-Calmettes Cancer Centre, Marseille, France
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 Advanced Prostate Cancer Consensus Conference (APCCC), Lugano, Switzerland, Thurs, April 30 – Sat, May 2, 2026.
References:- Moreira DM, Presti JC Jr, Aronson WJ, et al. Natural history of persistently elevated prostate-specific antigen after radical prostatectomy: Results from the SEARCH database. J Urol. 2009 Nov;182(5):2250-2255.
- Farolfi A, Gafita A, Calais J, et al. 68Ga-PSMA-11 Positron Emission Tomography Detects Residual Prostate Cancer after Prostatectomy in a Multicenter Retrospective Study. J Urol. 2019 Dec;202(6):1174-1181.
- Pound CR, Partin AW, Eisenberger MA, Chan DW, Pearson JD, Walsh PC. Natural history of progression after PSA elevation following radical prostatectomy. JAMA 1999 May 5;281(17):1591-1597.
- Freedland SJ, Humphreys EB, Mangold LA, et al. Risk of prostate cancer-specific mortality following biochemical recurrence after radical prostatectomy. JAMA. 2005 Jul 27;294(4):433-439.
- Markowski MC, Chen Y, Feng Z, et al. PSA doubling time and absolute PSA predict metastasis-free survival in men with biochemically recurrent prostate cancer after radical prostatectomy. Clin Genitourin Cancer. 2019 Dec;17(6):470-475.