(UroToday.com) The 2026 Advanced Prostate Cancer Consensus Conference (APCCC) meeting featured a management of metastatic hormone-sensitive prostate cancer (mHSPC) session and a presentation by Dr. Tyler Seibert discussing radiation therapy of the primary in patients with mHSPC. For the first part of his presentation, Dr. Seibert highlighted the current literature assessing radiation to the primary for patients with mHSPC, starting with the HORRAD trial.1
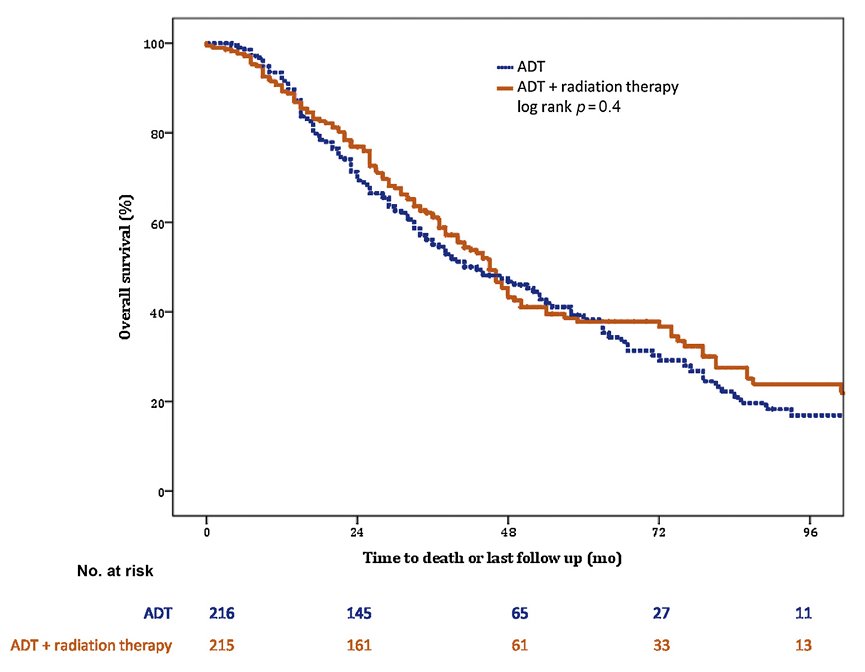
HORRAD was a multicenter, prospective, randomized controlled trial of 432 patients with previously untreated, de novo mHSPC at 28 centers across The Netherlands between November 2004 and September 2014. All study-eligible patients had a PSA >20 ng/ml and documented bone metastases on bone scan. Patients were randomized in a 1:1 fashion to either ADT with external beam radiotherapy or ADT alone. Patients in the external beam radiotherapy group received either intensity-modulated or three-dimensional conformal radiotherapy to the prostate alone (70 Gy in 20 fractions or 57.76 Gy in 19 fractions), and pelvic lymph nodes were not included in the clinical target volume. The median patient age in HORRAD was 67 years, and the median PSA was 142 ng/ml. At a median follow-up of 47 months, there were no significant differences in median overall survival between the two treatment arms: 45 and 43 months in the external beam radiotherapy + ADT and ADT arms, respectively (HR 0.90, 95% CI 0.70-1.14, p=0.40):
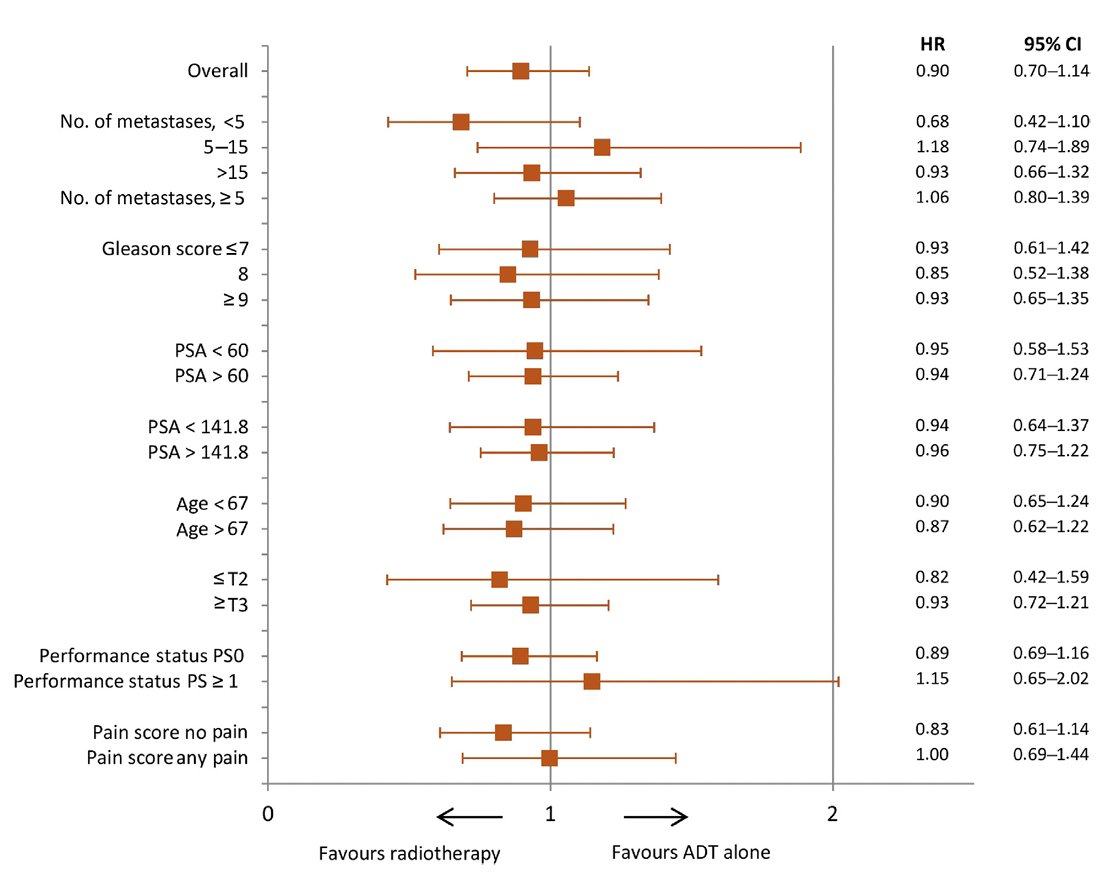
No subgroup analysis by CHAARTED volume criteria was performed, but subgroup analysis by number of metastatic lesions suggested a potential overall survival benefit for radiotherapy in patients with <5 metastatic sites (HR: 0.68, 95% CI: 0.42-1.10):
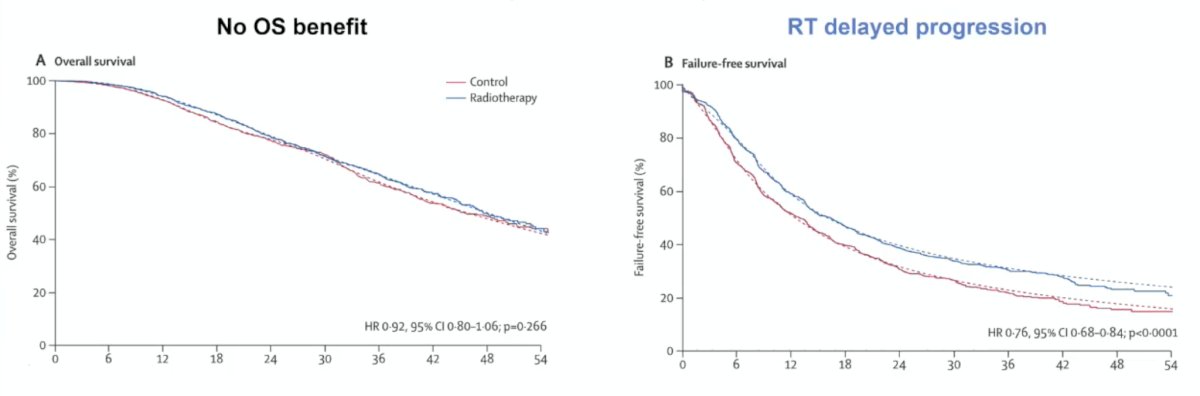
STAMPEDE (Arm H) was an open-label, randomized controlled phase III trial of 2,061 men from 117 hospitals across Switzerland and the UK. This arm randomized patients with de novo mHSPC in a 1:1 fashion to standard of care + radiotherapy versus standard of care alone between January 2013 and September 2016. Standard of care was lifelong ADT with upfront docetaxel permitted from December 2015. Men allocated to radiotherapy received either a daily (55 Gy in 20 fractions over 4 weeks) or weekly (36 Gy in six fractions over 6 weeks) schedule that was nominated before randomization. The planning target volume consisted of the prostate only, the primary outcome was overall survival, and subgroup analysis by metastatic volume (CHAARTED criteria) was planned a priori. The median patient age was 68.0 years, with a median PSA of 97 ng/ml; 18% of patients received early docetaxel. Overall, 54% of men had high metastatic burden compared to 40% with low metastatic burden (6% unknown). In the overall cohort, radiotherapy improved failure-free survival (HR 0.76, 95% CI 0.68–0.84) but not overall survival (HR 0.92, 95% CI 0.80–1.06):
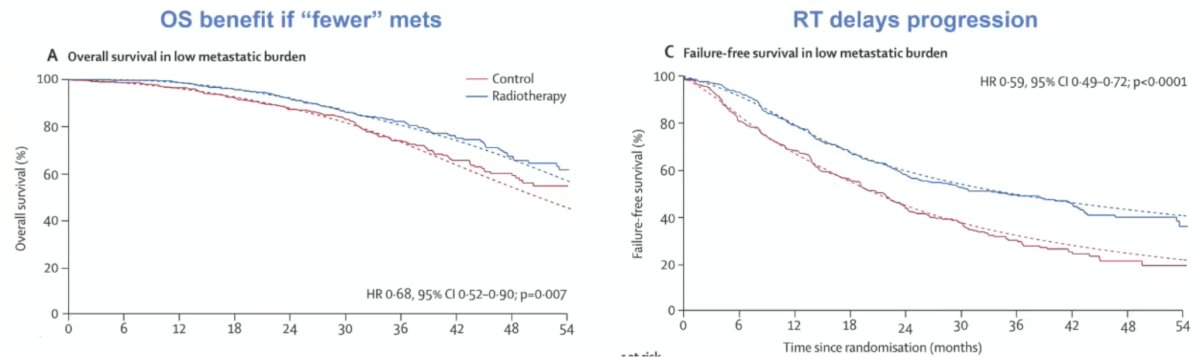
However, when stratified by metastatic burden, overall survival benefits were seen in the low volume group (HR 0.68, 95% CI 0.52-0.90), with restricted mean survival time improved by 3.6 months from 45.4 to 49.1. Additionally, there was also an improvement in failure-free survival among patients with low-volume metastatic disease (HR 0.59, 95% CI 0.49-0.72):
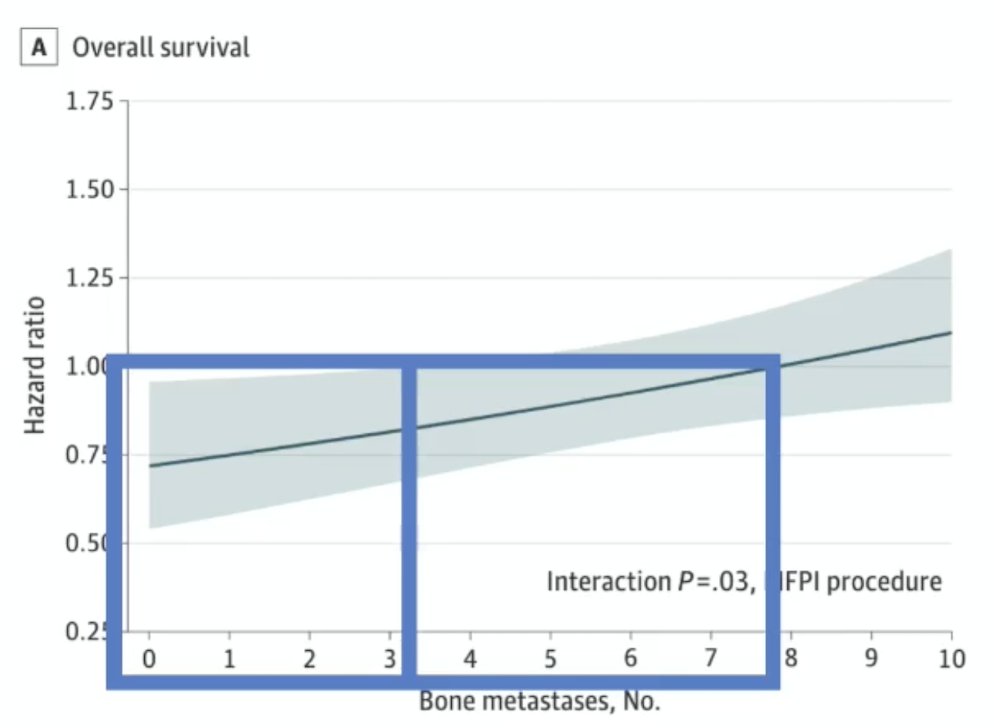
A secondary analysis of the STAMPEDE Arm H trial evaluating the association of metastatic burden with survival benefit from prostate radiotherapy demonstrated that the survival benefit decreased continuously as the number of bone metastases increased, with benefit most pronounced up to 3 bone metastases. The magnitude of benefit from the addition of prostate radiotherapy was greater in patients with low metastatic burden with only non-regional lymph nodes (M1a) or 3 or fewer bone metastases without visceral metastasis (HR for overall survival: 0.62, 95% CI 0.46 - 0.83; HR for failure-free survival: 0.57, 95% CI 0.47 - 0.70) than among patients with 4 or more bone metastases or any visceral/other metastasis (HR for overall survival: 1.08; 95% CI: 0.91 - 1.28; interaction p= 0.003; HR for failure-free survival: 0.87; 95% CI: 0.76 - 0.99; interaction p = 0.002):
The PEACE-1 trial also assessed the efficacy and safety of prostate radiotherapy for patients with low-volume, de novo mHSPC.4 Radiotherapy to the prostate was delivered in 37 fractions for a cumulative dose of 74 Gy, and pelvic lymph nodes were not included. The co-primary endpoints for this analysis were overall survival and radiographic progression-free survival, assessed per the PCWG2 criteria. The median age in the low-volume cohort was 67 years. The median PSA was 9.0 and 10.3 ng/ml in the standard of care + radiotherapy and standard of care arms, respectively. Notably, 50% of patients received docetaxel as standard of care treatment, with 50% of the cohort overall randomized to receive additional abiraterone acetate/prednisone. In the overall cohort, there was no overall survival benefit for the addition of radiotherapy (HR 0.98, 95% CI 0.83-1.14), however radiotherapy delayed castration resistance (HR 0.79, 95% CI 0.69-0.90):
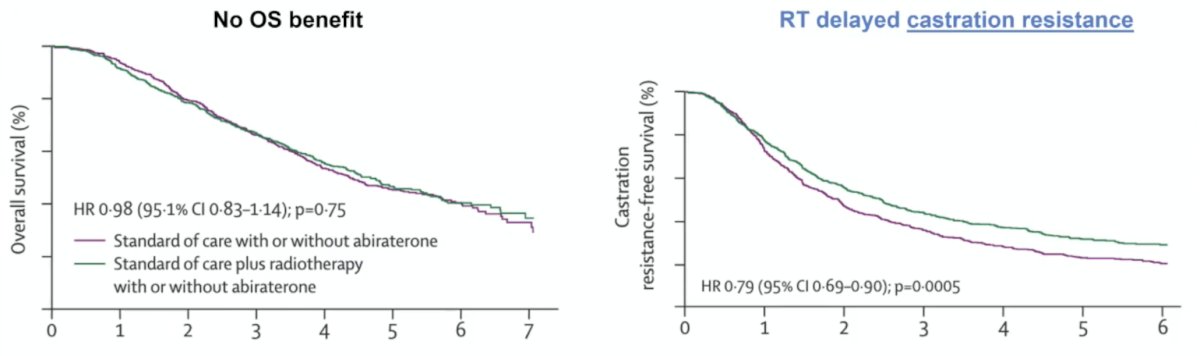
The addition of prostate radiotherapy to standard of care +/- abiraterone was also associated with a significant improvement in time to castration resistance in the low-volume cohort (HR 0.62, 95% CI 0.44 – 0.87).
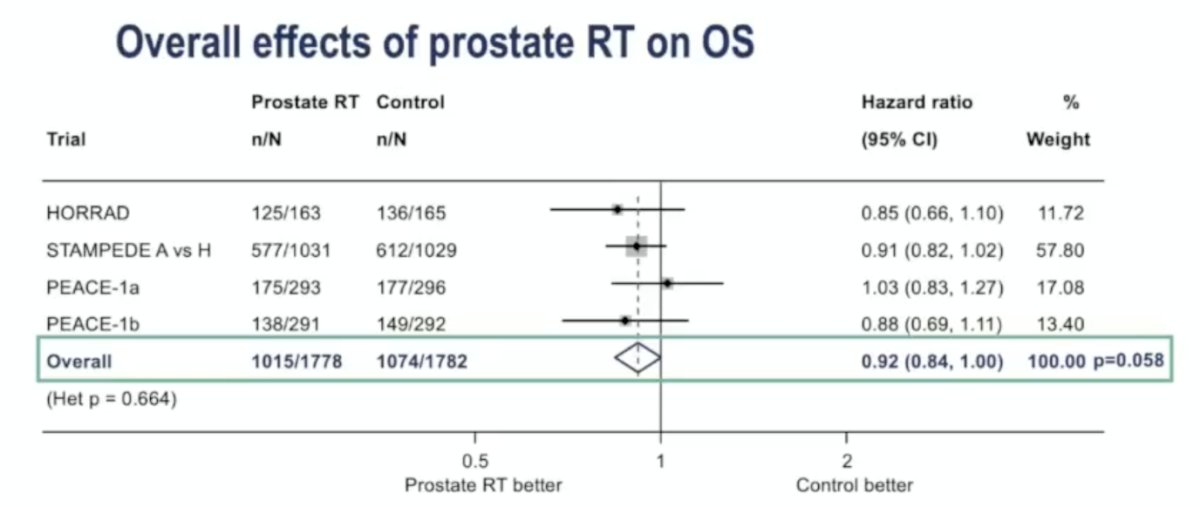
Presented at ESMO 2025, the STOPCAP meta-analysis assessed individual participant data in order to evaluate the effect of prostate radiotherapy on synchronous mHSPC. The analysis included data from HORRAD, STAMPEDE, and two PEACE-1 cohorts (radiotherapy with and without abiraterone). For the overall effect of prostate radiotherapy on overall survival, there was a pooled hazard ratio of 0.92 (95% CI 0.84–1.00; p = 0.058). While not reaching conventional statistical significance, the trend favored prostate radiotherapy. Moreover, there was a ~5% absolute 5-year overall survival benefit if there were <5 bone metastases:
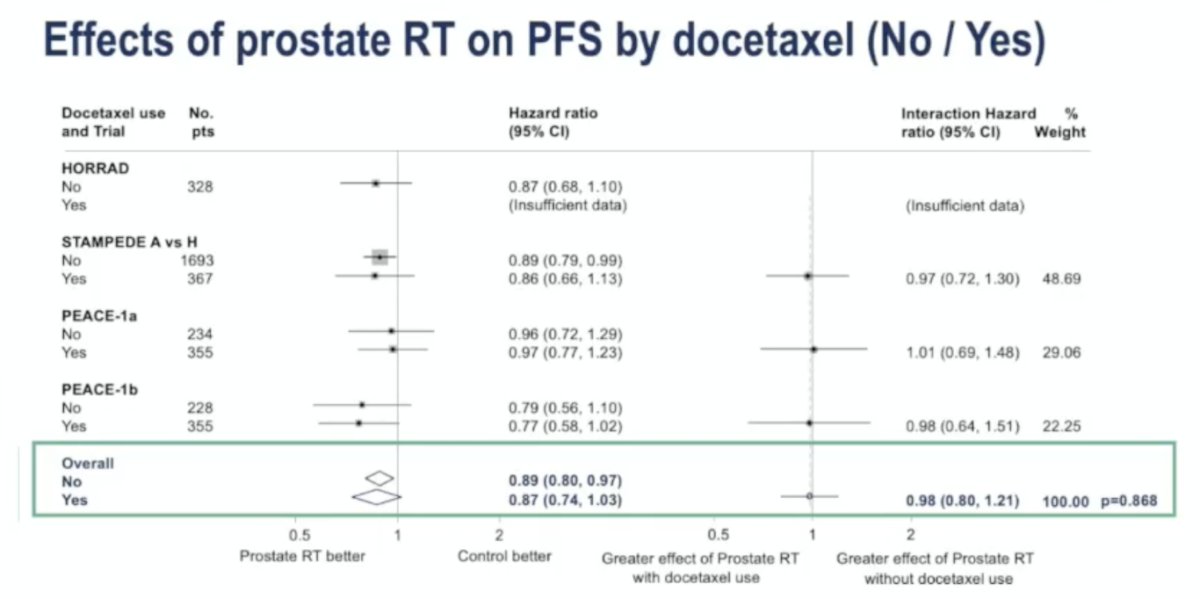
Additionally, the benefit of prostate radiotherapy on progression-free survival was consistent regardless of concurrent docetaxel use. The pooled HR was 0.89 (95% CI 0.80–0.97) for patients not receiving docetaxel and 0.87 (95% CI 0.74–1.03) for those receiving docetaxel, with no significant interaction between groups (interaction HR 0.98; 95% CI 0.80–1.21; p = 0.868):
What is the impact of radiotherapy on the primary on quality of life?
- Treatment takes time (5-6 fractions is more efficient)
- Acutely, grade 1-2 adverse events are common (genitourinary more common than gastrointestinal)
- There is no increase in grade 3+ adverse events (STAMPEDE)
- Radiotherapy is associated with fewer late urinary events (PEACE-1, HORRAD)
Dr. Seibert provided the following interpretation for low-burden metastatic patients:
- For M1 only on PSMA PET:
- Treat the primary. These patients were included in M0 trials
- Do not penalize patients for getting a better scan
- For low burden on conventional imaging: treat the primary, since there is a clear progression-free survival benefit and a probable overall survival benefit
Dr. Seibert also provided the following interpretation for high burden metastatic patients:
- For M1 only on PSMA PET
- Treat the primary. These patients were included in M0 trials
- Do not penalize patients for getting a better scan
- You will only know this if you get a bone scan
- High burden on conventional imaging
- Bulky disease - treat the primary
- Not bulky disease
- Start systemic therapy and assess in ~3 months
- Consider the patient’s performance status
- If they are receiving docetaxel, consider radiotherapy after treatment is complete
To conclude, Dr. Siebert noted several open-ended questions:
- Metastasis-directed therapy?
- We do not know which patients will benefit
- We should support ongoing trials: TERPS, STAMPEDE2, METANOVA, TRITONS
- What is the best radiotherapy dose?
- Doses: 55Gy/20fx, 36Gy/6fx (35Gy/5fx)
- On a trial with metastasis-directed therapy, we may consider a curative radiotherapy dose to the primary
- Pelvic lymph nodes (if not involved on PSMA PET)?
- Off trial: why treat a hypothetical microscopic disease in the setting of macroscopic metastasis?
- On trial: some trials allow/encourage elective nodal coverage on the metastasis-directed therapy arm
Presented by: Tyler Seibert, MND, PhD, Associate Professor, Division of Radiation Oncology, Associate Director of the Center for Translational Imaging and Precision Medicine (CTIPM), Section Chief, Genitourinary Cancers, RMAS Center for Precision Radiation Medicine (CPRM), UC San Diego Health, San Diego, CA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 Advanced Prostate Cancer Consensus Conference (APCCC), Lugano, Switzerland, Thurs, April 30 – Sat, May 2, 2026.
- Boeve LMS, Hulshof MCCM, Vis AN, et al. Effect on Survival of Androgen Deprivation Therapy Alone Compared to Androgen Deprivation Therapy Combined with Concurrent Radiation Therapy to the Prostate in Patients with Primary Bone Metastatic Prostate Cancer in a Prospective Randomised Clinical Trial: Data from the HORRAD Trial. Eur Urol. 2019;75(3):410-418.
- Parker CC, James ND, Brawley CD, et al. Radiotherapy to the primary tumour for newly diagnosed, metastatic prostate cancer (STAMPEDE): a randomised controlled phase 3 trial. Lancet. 2018;392(10162):2353-2366.
- Ali A, Hoyle A, Haran AM, et al. Association of Bone Metastatic Burden with Survival Benefit from Prostate Radiotherapy in Patients with Newly Diagnosed Metastatic Prostate Cancer: A Secondary Analysis of a Randomized Clinical Trial. JAMA Onc 2021 Apr 1;7(4):555-563.
- Bossi A, Foulon S, Maldonado X, et al. Efficacy and safety of prostate radiotherapy in de novo metastatic castration-sensitive prostate cancer (PEACE-1): A multicenter, open-label, randomized, phase 3 study with a 2 x 2 factorial design. Lancet. 2024 Nov 23;404(10467):2065-2076.