(UroToday.com) The 2026 APCCC meeting featured a management of metastatic hormone-sensitive prostate cancer (mHSPC) session and a presentation by Dr. Robert Jones discussing patients who should receive doublet systemic therapy.
Dr. Jones started his presentation by emphasizing that the reason we use multi-agent regimens is that most curative regimens are multi-agent, cytotoxic regimens, and one drug typically directly targets a resistance pathway of another. The reason we use androgen receptor pathway inhibitor doublet regimens is that all but one of these double trials have shown an overall survival gain, despite the crossover rate to androgen receptor pathway inhibitor in the control arms being high (ie. PEACE-1: 80% received an androgen receptor pathway inhibitor). However, this increases the duration of exposure to one or both drugs, even if the total time on therapy may be shorter.
The following table highlights triplet versus doublet therapies in differing subgroups:
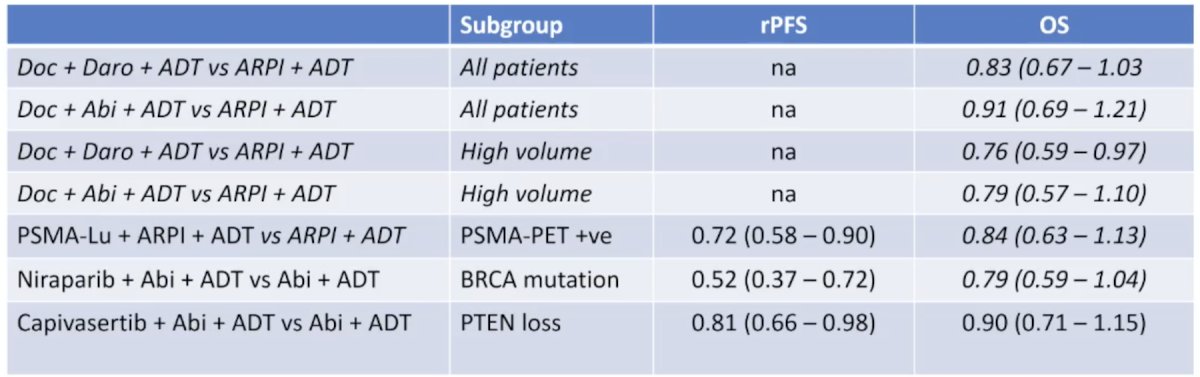
Dr. Jones notes that we currently have several options for mHSPC treatment:
- 0 drugs: for patients who desire to avoid castration, and perhaps utilize metastasis-directed therapy
- 1 drug: ADT – evidence suggests that this is still a ‘popular’ option
- 2 drugs: ADT + androgen receptor pathway inhibitor
- 3 drugs: ADT + androgen receptor pathway inhibitor + (capivasertib, docetaxel, niraparib, 177Lu-PSMA-617)
There are several groups of patients that should definitely not get triplet therapy (the “no brainers”), including patients who have all of: metachronous disease, low burden of disease, PSMA negative, BRCA intact, and PTEN competent. However, there are several groups that may not be ideal candidates for triplet therapy, but may require more thought/clinical decision making:
- Where comorbidity dictates they will not live to benefit from the incremental gain
- Where the incremental risk of harm outweighs the incremental gain (ie. negative quality of life years gained)
- Where health economics dictate, the additional costs may be better spent elsewhere
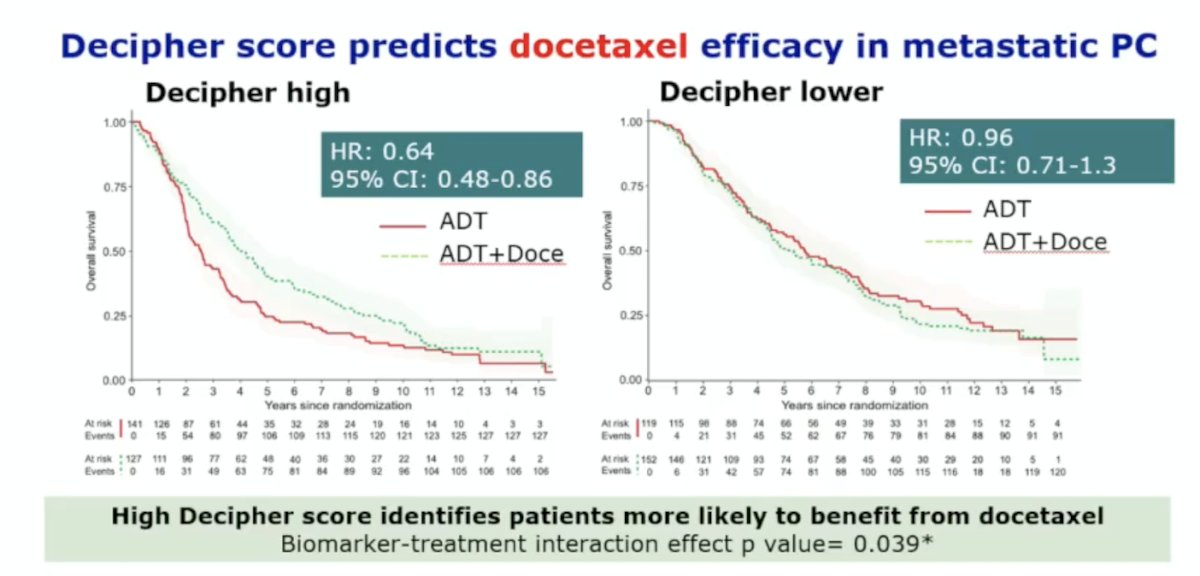
Perhaps we can predict who will not benefit from triplet therapy. Data presented at ESMO 2024 assessed the role of the Decipher GC in predicting docetaxel efficacy in metastatic prostate cancer in the STAMPEDE trial. Among 3,099 patients who were randomized to ADT +/- docetaxel +/- zoledronic acid or ADT +/- abiraterone, Dr. Grist and colleagues aimed to link tumor multi-gene expression signatures to 14-year prospective overall survival follow-up. They found that a high Decipher GC score identified patients more likely to benefit from docetaxel, with a biomarker-treatment interaction effect p-value of 0.039:
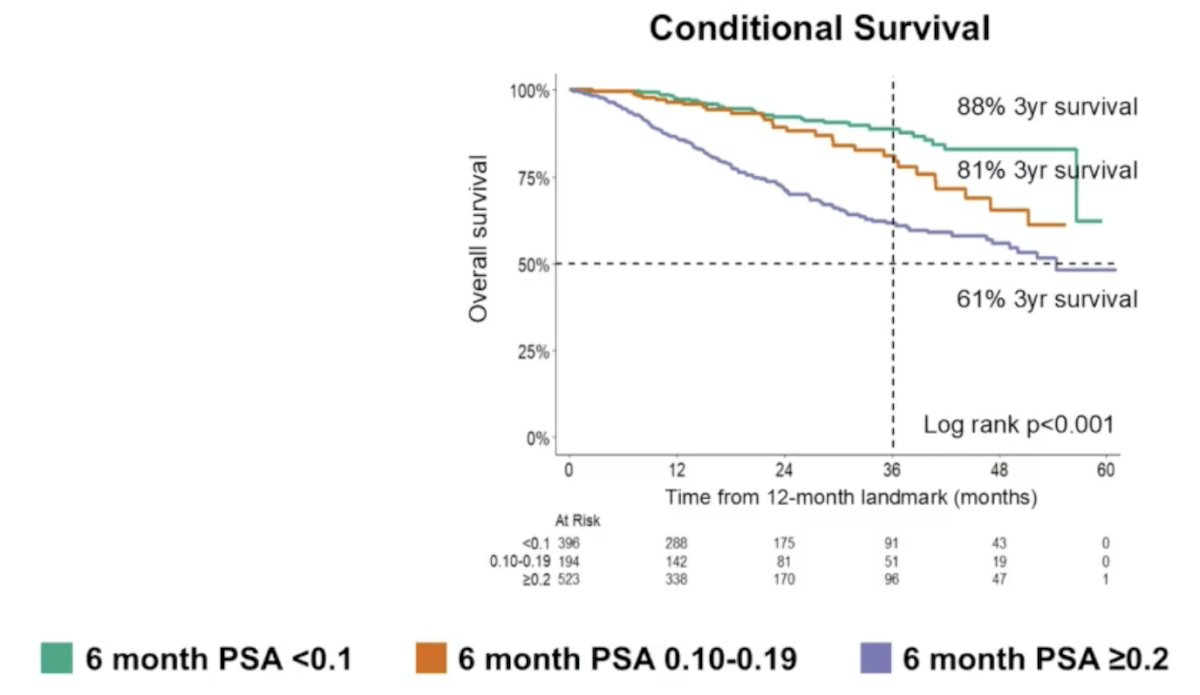
We can also further refine patient selection by assessing the 6-month PSA response to treatment. At ASCO 2025, Dr. Ong and colleagues showed that patients with a 6-month PSA response >= 0.2 ng/mL had worse outcomes compared to those with a 6-month PSA response of 0.10-0.19 ng/mL, with the worst outcomes among those with a 6-month PSA response <0.1 ng/mL:
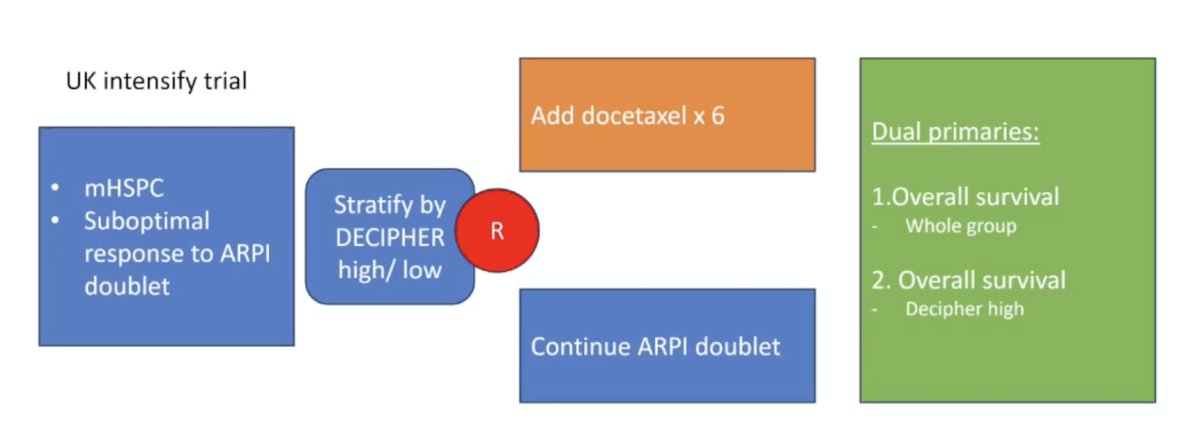
The UK Intensify trial is assessing patients with mHSPC and a suboptimal response to androgen receptor pathway inhibitor doublet therapy (stratified by Decipher GC high versus low score) and randomizing them to the addition of 6 cycles of docetaxel versus continuing androgen receptor pathway inhibitor doublet therapy. The dual primary endpoints are overall survival for the whole group and overall survival in the Decipher GC high patients:
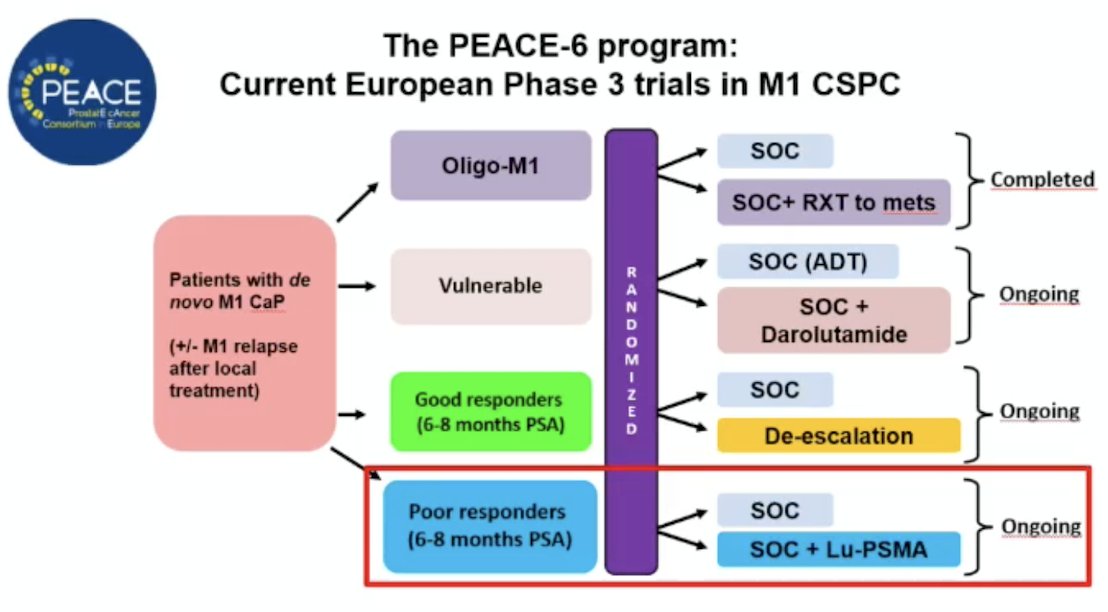
The PEACE-6 PR trial will also assess triplet and even quadruplet therapy for poor responders:
Early, deep PSA response (<= 0.2 ng/mL) is consistently associated with good outcomes, and some of these patients may have been overtreated, but these trials do not explore the value of additional treatment in good responders.
Dr. Jones concluded his presentation emphasizing that patients should receive doublet systemic therapy for mHSPC:
- BRCA wild type, PTEN competent, PSMA negative, low volume metachronous mHSPC
- No triplet therapy is unequivocally proven to be more active than sequential therapy:
- Shared decision-making is key
- Patients choosing doublet therapy is an inevitable consequence of shared decision-making
- Having a choice of triplets should increase the overall scope of triplet therapy
- Decision-making informed by biomarkers or early response may enable patient selection for doublet therapy
Presented by: Robert J. Jones, University of Glasgow, Beatson West of Scotland Cancer Centre, Glasgow, United Kingdom
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 Advanced Prostate Cancer Consensus Conference (APCCC), Lugano, Switzerland, Thurs, April 30 – Sat, May 2, 2026.