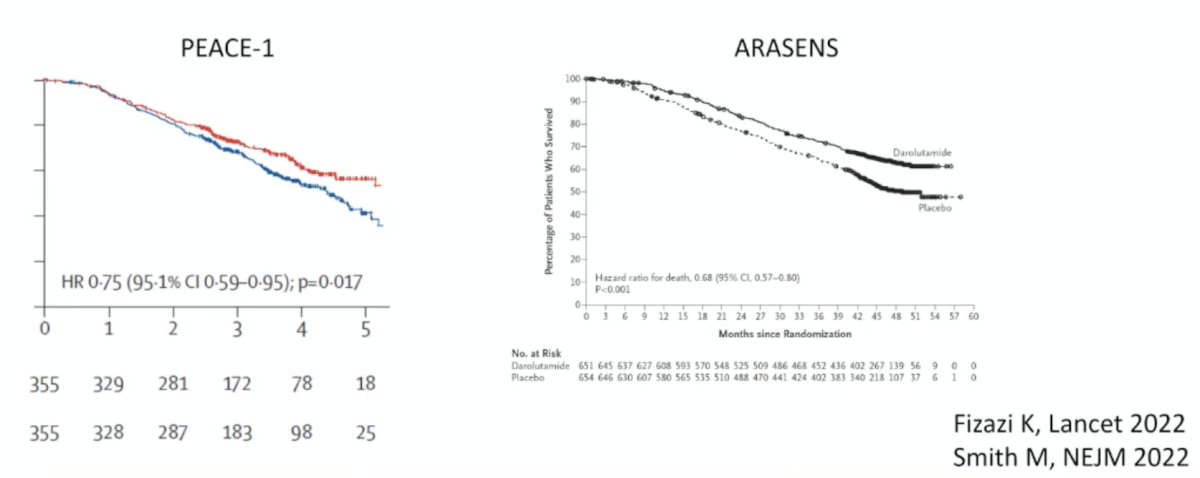
(UroToday.com) The 2026 APCCC meeting featured a management of metastatic hormone sensitive prostate cancer (mHSPC) session and a presentation by Dr. Karim Fizazi discussing patients that should receive triplet systemic therapy. Why should we favor triplet therapy in de novo mHSPC? Dr. Fizazi notes that we have the most meaningful overall survival benefit ever versus an active comparator based on the PEACE-11 and ARASENS2 trials:
Dr. Fizazi emphasized that there are many other good reasons to choose a triple regimen in de novo mHSPC:
- There is benefit regardless of volume and risk of disease
- Only 6 cycles of docetaxel over ~4.5 months are required in mHSPC, which is usually well tolerated with G-CSF support
- Androgen receptor pathway inhibitors and taxanes complete each other
- There is heterogeneity in mHSPC: androgen receptor sensitive clones, as well as taxane sensitive clones
- If not used in the mHSPC space, docetaxel is likely to be used for mCRPC, when patients are typically older and sicker
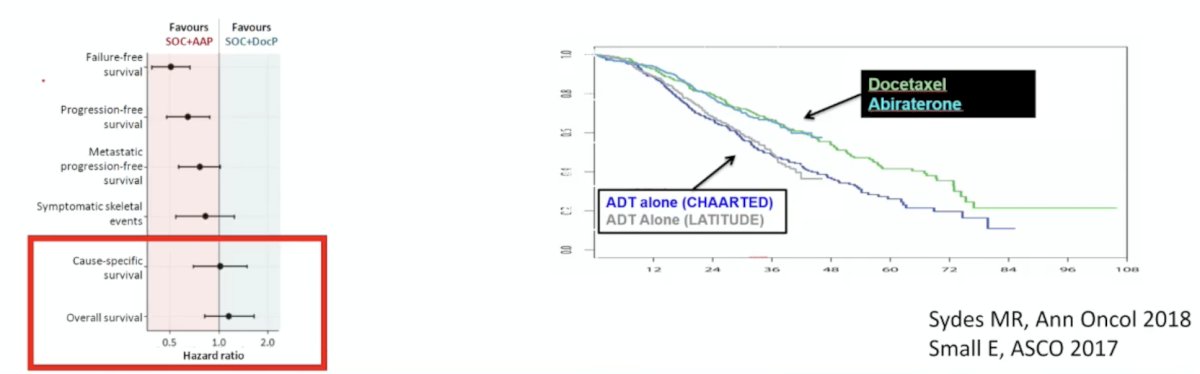
Dr. Fizazi acknowledges that there is a valid argument that we do not know if a triple regimen is better than a hormonal doublet regimen. However, STAMPEDE3 showed that overall survival is the same, whatever the doublet (ADT + docetaxel or ADT + abiraterone):
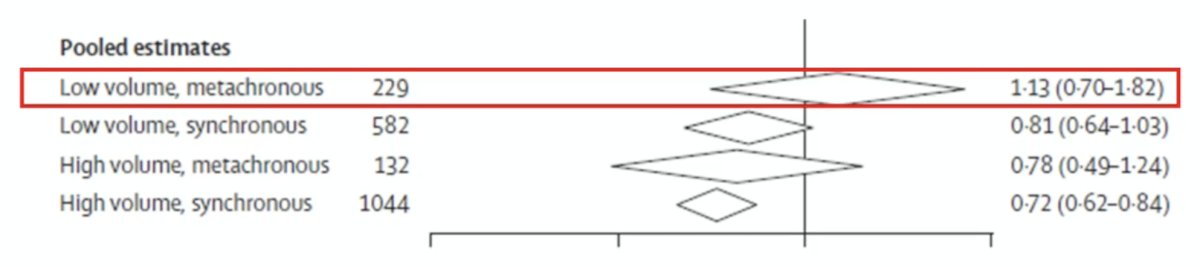
Dr. Fizazi notes that one caveat is that we should not be using triplet therapy for relapsing (low volume) mHSPC based on a systematic review and meta-analysis from Vale et al.:4
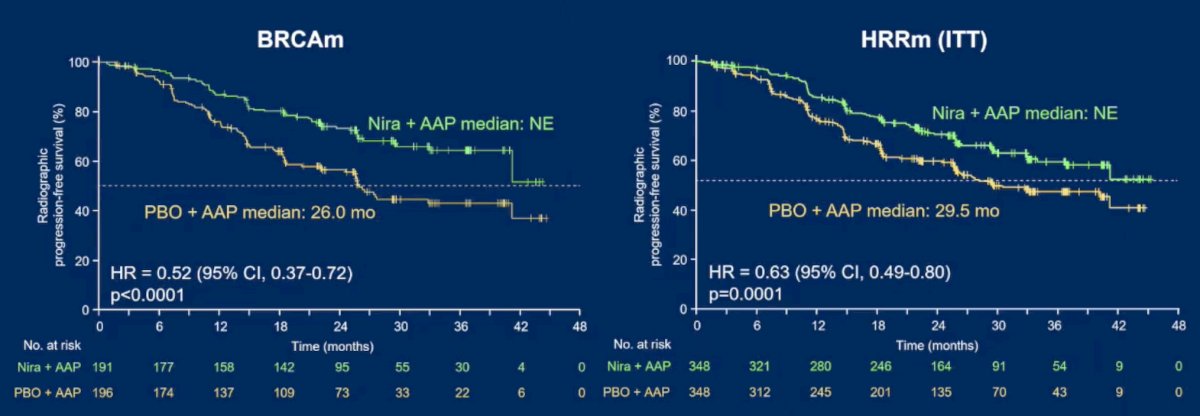
For the rest of his presentation, Dr. Fizazi discussed new systemic triplet therapies that are on the horizon. The AMPLITUDE trial evaluated combining niraparib with abiraterone acetate + prednisone versus placebo and abiraterone acetate + prednisone in mHSPC with HRR gene alterations:5
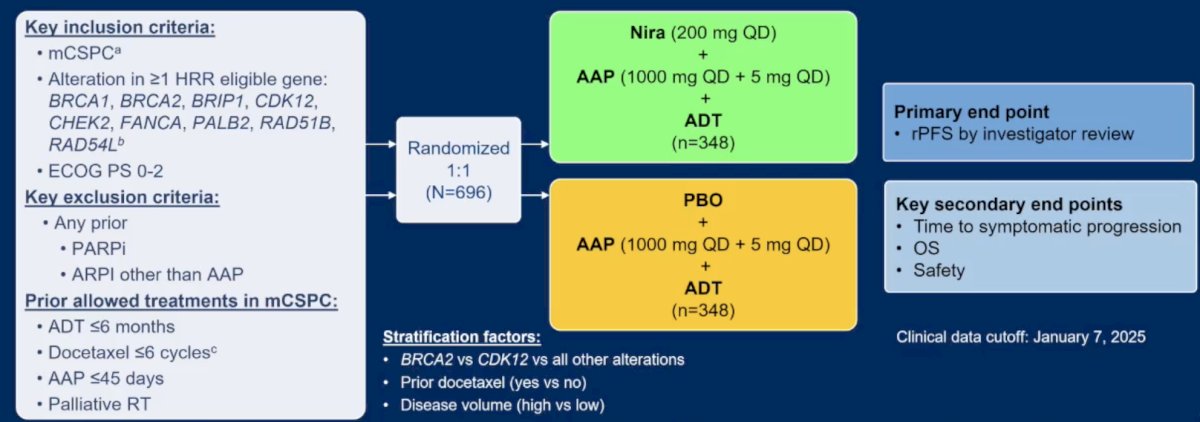
The primary endpoint was met, with a significant improvement in radiographic progression free survival observed in the BRCA subgroup: median not reached for niraparib and abiraterone acetate + prednisone group versus 26 months for the abiraterone acetate + prednisone group (HR 0.52, 95% CI 0.37-0.72; p < 0.0001). This was also noted in the intention to treat population (HR 0.63, 95% CI 0.49-0.80; p = 0.0001):
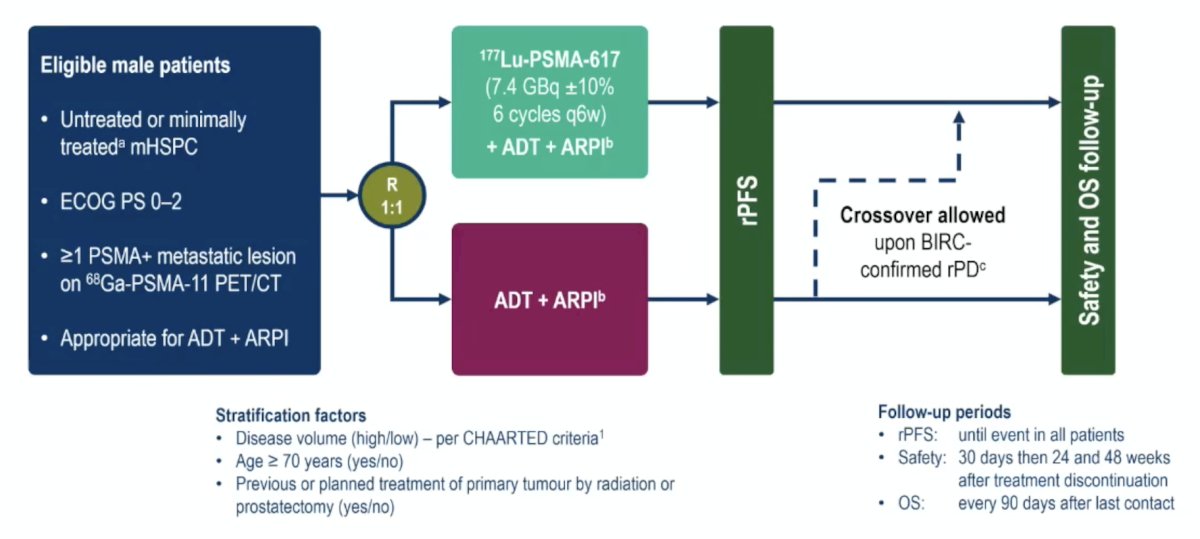
The PSMAddition trial randomized men with untreated or minimally treated mHSPC and ≥1 PSMA-positive metastatic lesion on 68Ga-PSMA-11 PET/CT to the experimental arm of 177Lu-PSMA 617 (7.4 GBq ±10% 6 cycles every 6 weeks) + ADT + androgen receptor pathway inhibitor versus the control arm of ADT + androgen receptor pathway inhibitor. Of note, crossover to the 177Lu-PSMA 617 arm was permitted upon radiographic progression:
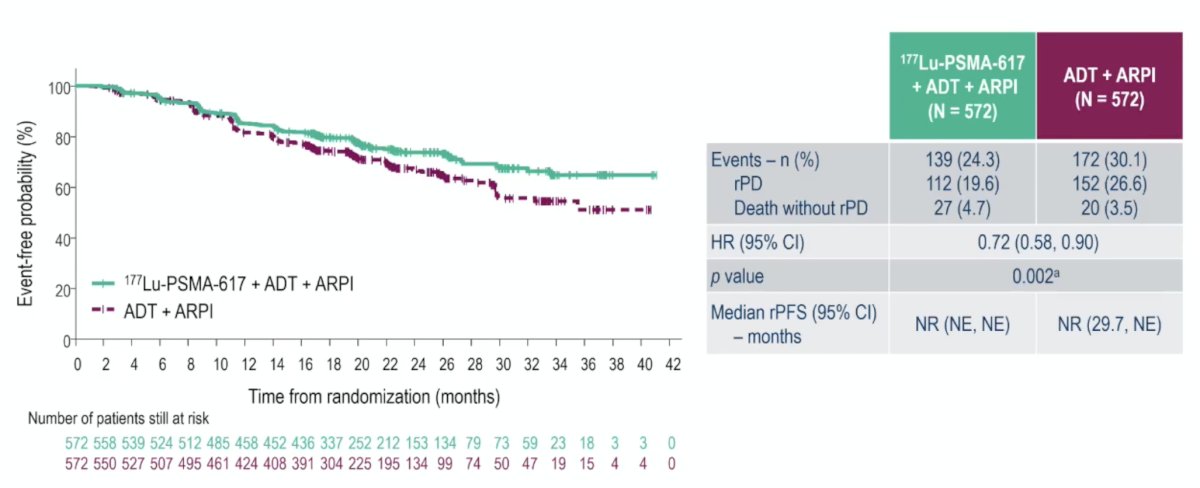
The study met its primary endpoint with radiographic progression free survival significantly prolonged with the addition of 177Lu-PSMA-617 (HR 0.72, 95% CI 0.58-0.90; p = 0.002). The median radiographic progression free survival has not been reached in either arm:
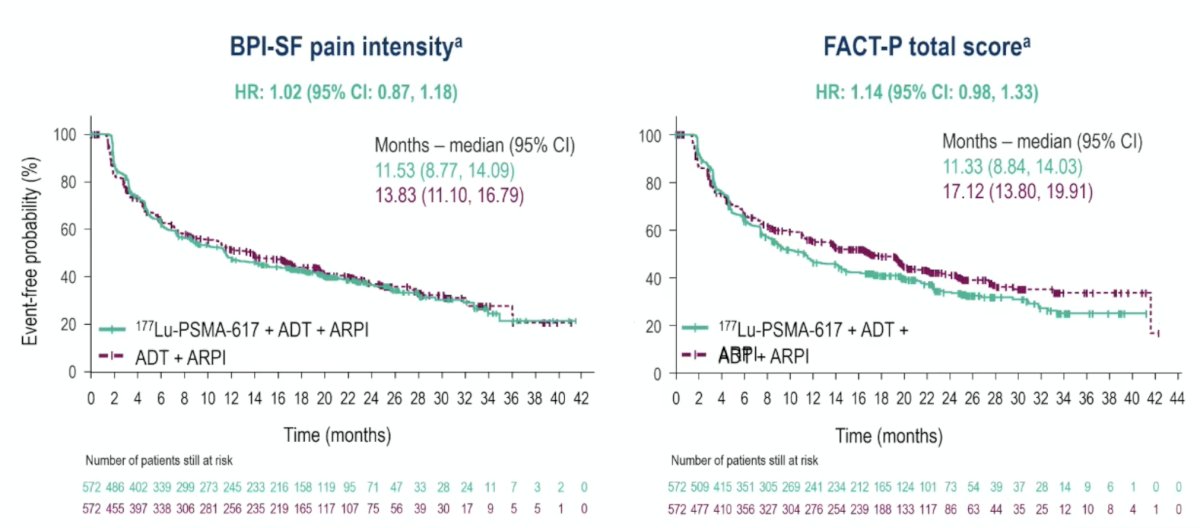
With regards to health related quality of life and pain, there were 1,144 patients randomized, with a median study treatment exposure of 20.6 months in the 177Lu-PSMA-617 arm and 19.94 months in the control arm. Hazard ratios for time to worsening in all FACT-P total score and BPI-SF scales/subscales were >1.0 but <1.2, and all 95% CIs included 1.0 (177Lu-PSMA-617 arm versus control arm):
CAPItello-281, presented at ESMO 2025, is a global, multicenter, randomized, double-blind, phase III trial that included patients meeting the following eligibility criteria: (i) de novo mHSPC and (ii) PTEN deficiency (≤10% of cells expressing PTEN by IHC). Eligible participants (n = 1,012) were randomized 1:1 to capivasertib (400 mg BID, 4 days on and 3 days off) + abiraterone acetate (1,000 mg daily) + prednisone (5 mg daily) + ADT versus placebo + abiraterone acetate + prednisone + ADT:
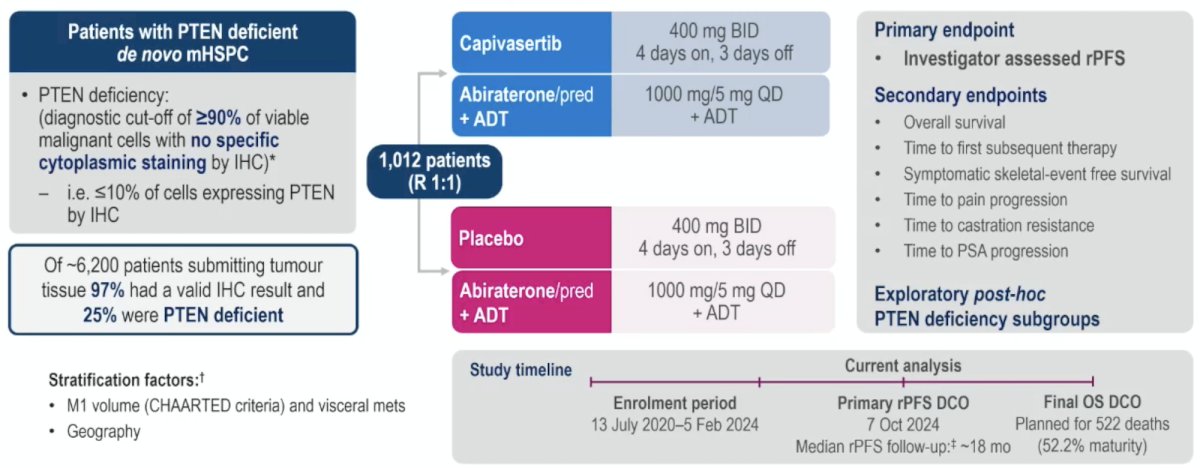
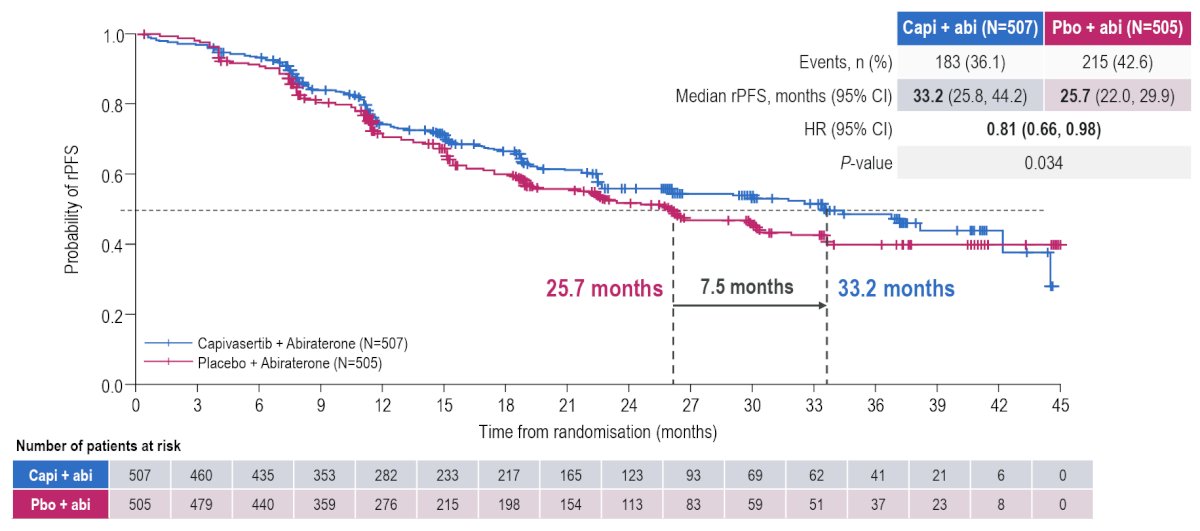
The study met its primary endpoint with capivasertib prolonging radiographic progression free survival by 7.5 months (median: 33.2 versus 25.7 months; HR 0.81, 95% CI 0.66-0.98, p = 0.034):
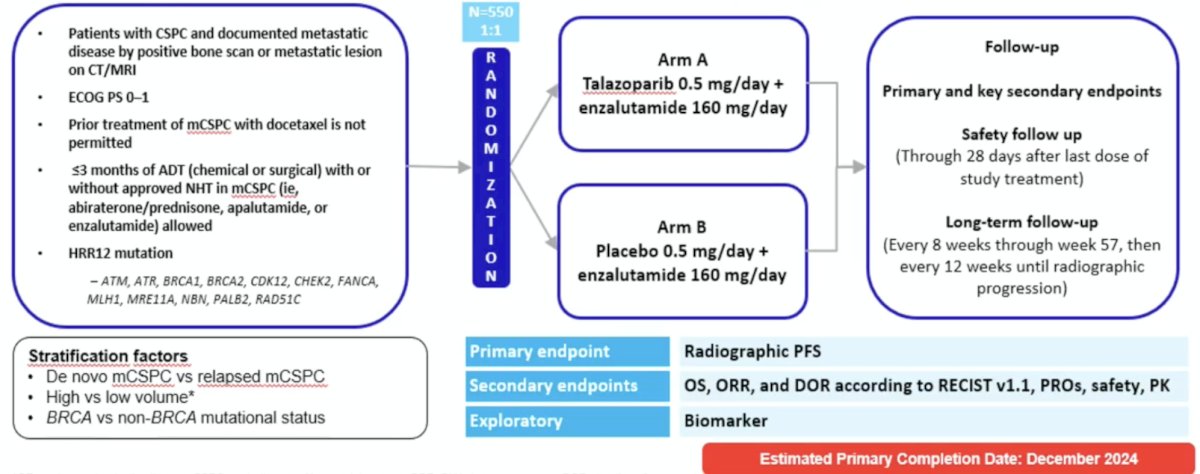
Furthermore, more data is coming soon with the expected reporting of the TALAPRO-3 trial assessing the safety and efficacy of talazoparib in combination with enzalutamide compared with placebo in combination with enzalutamide in men with mHSPC with DNA damage repair HRR alterations:
Dr. Fizazi concluded his presentation discussing patients that should receive triplet systemic therapy with the following take-home points:
- 2 drugs are better than 1 drug, and 3 drugs are better than 2 drugs
- The benefit of triplet therapy is seen independent of volume/risk and should be favored when doable
- Biology matters: there are emerging biomarkers for selecting docetaxel triplet therapies (ie. BRCA, PSMA, PTEN)
- Further intensification is currently being tested in poor responders (6-8 months, PSA > 0.2 ng/mL)
Presented by: Karim Fizazi, MD, PhD, Centre Oscar Lambret, Institut Gustave Roussy, University of Paris-Saclay, Lille, France
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 Advanced Prostate Cancer Consensus Conference (APCCC), Lugano, Switzerland, Thurs, April 30 – Sat, May 2, 2026.
References:
- Fizazi K, Foulon S, Carles J, Roubaud G, et al. Abiraterone plus prednisone added to androgen deprivation therapy and docetaxel in de novo metastatic castration-sensitive prostate cancer (PEACE-1): A multicentre, open-label, randomized, phase 3 study with a 2 x 2 factorial design. Lancet. 2022 Apr 30;399(10336):1695-1707.
- Smith MR, Hussain M, Saad F, et al. Darolutamide and Survival in Metastatic, Hormone-Sensitive Prostate Cancer. N Engl J Med. 2022 Mar 24;386(12):1132-1142.
- Sydes MR, Spears MR, Mason MD, Clarke NW, Dearnaley DP, de Bono JS, et al. Adding abiraterone or docetaxel to long-term hormone therapy for prostate cancer: directly randomised data from the STAMPEDE multi-arm, multi-stage platform protocol. Ann Oncol. 2018;29:1235-48.
- Vale CL, Fisher DJ, Godolphin PJ, et al. Which patients with metastatic hormone sensitive prostate cancer benefit from docetaxel: A systematic review and meta-analysis of individual participant data from randomized trials. Lancet Oncol. 2023 Jul(7):783-797.
- Attard G, Agarwal N, Graff JN, et al. Niraparib and abiraterone acetate plus prednisone for HRR-deficient metastatic castration-sensitive prostate cancer: A randomized phase 3 trial. Nat Med. 2025 Dec;31(12):4109-4118.