(UroToday.com) The 2026 Advanced Prostate Cancer Consensus Conference (APCCC) meeting featured a high-risk and locally advanced prostate cancer session and a presentation by Dr. Bertrand Tombal discussing the importance of baseline testosterone and testosterone recovery in this setting. Dr. Tombal started his presentation by posing several clinically relevant questions regarding testosterone:
- Does baseline testosterone matter?
- Does on treatment testosterone matter?
- Does post-treatment testosterone matter?
- What do you do if testosterone does not recover after treatment?
The main reason to measure baseline testosterone is to predict testosterone recovery at the end of the treatment. However, the evidence for the prognostic value of baseline testosterone is remarkably low, but overall, there is no indication that it substantially influences cancer recurrence or mortality outcomes:
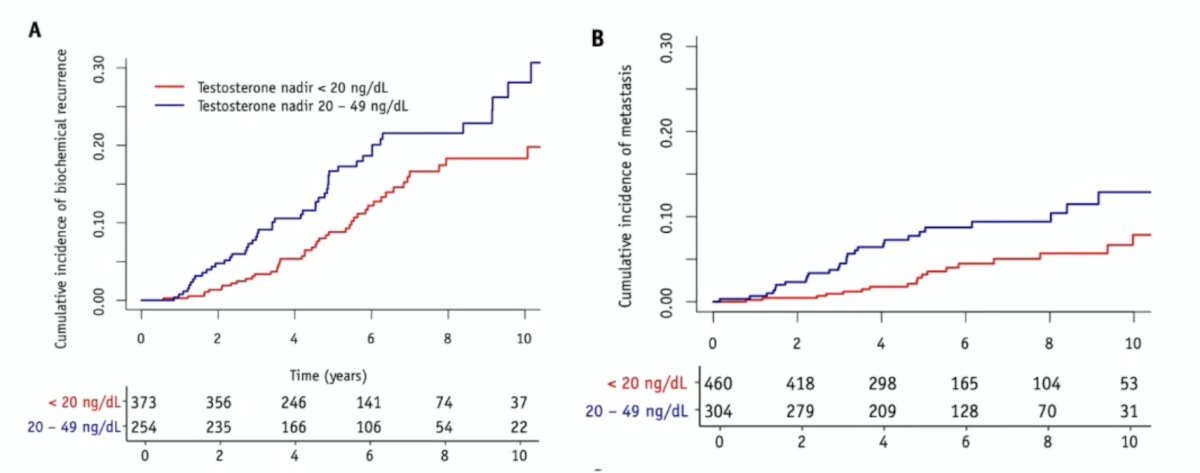
Regarding the importance of testosterone treatment, Bryant et al.1 assessed whether serum testosterone suppression below the castrate threshold of 50 ng/dL improves clinical outcomes in 764 U.S. veteran patients with localized prostate cancer undergoing definitive therapy. All patients in this study were treated with ADT + radiotherapy from 2000 to 2015, and the lowest testosterone value between 6 weeks and 6 months was recorded. A testosterone nadir of 20 to 49 ng/dL was associated with higher 3-month post-radiation therapy PSA compared to <20 ng/dL (p = 0.001) and higher 2-year PSA nadir (p = 0.005). Compared to the <20-ng/dL group, the 20 to 49-ng/dL group showed higher 10-year biochemical recurrence rates (28.1% versus 18.3%) and metastasis rates (12.9% versus 7.8%):
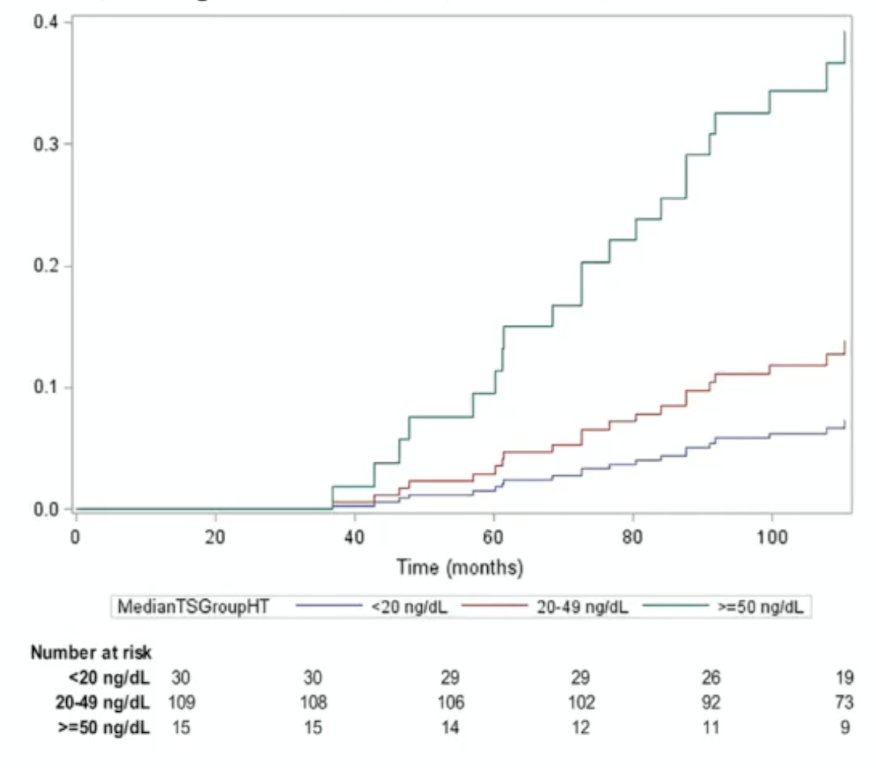
In the DART 01/05 trial, 355 men with intermediate and high-risk prostate cancer were randomized to 4 versus 28 months of ADT plus high-risk radiotherapy. Amongst testosterone subgroups, there were no statistically significant differences in 10-year biochemical disease-free survival, metastasis-free survival, or overall survival. However, a median testosterone >50 ng/dL was significantly associated with a decrease in biochemical disease-free survival (HR 6.58, 95% CI 1.28-33.76, p = 0.03):
Dr. Tombal notes that the results are divergent for whether an on-treatment testosterone matters, but generally, a testosterone level < 50 ng/mL should be achieved.
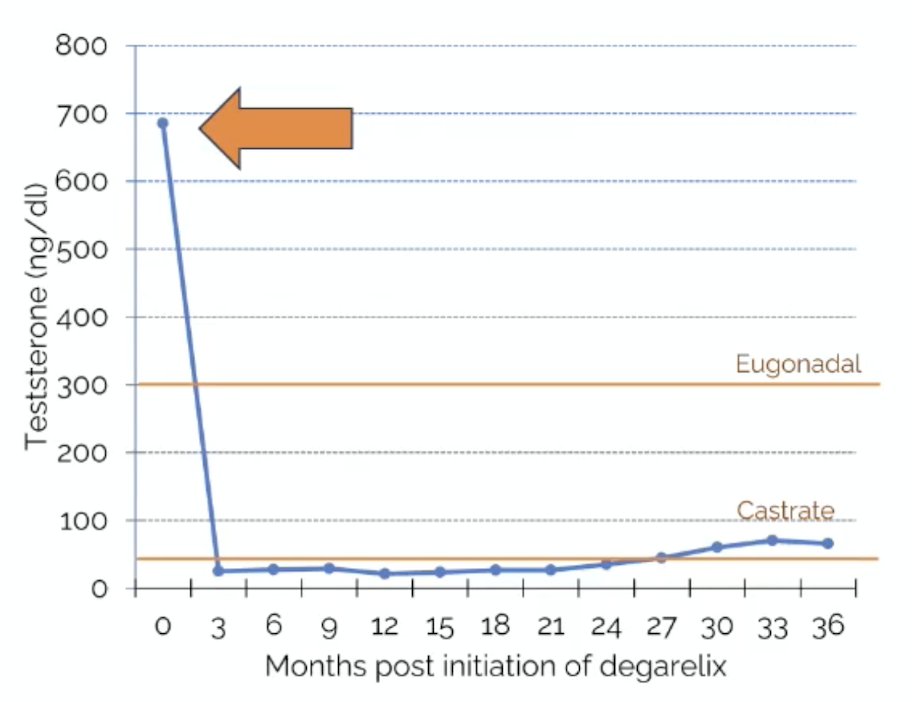
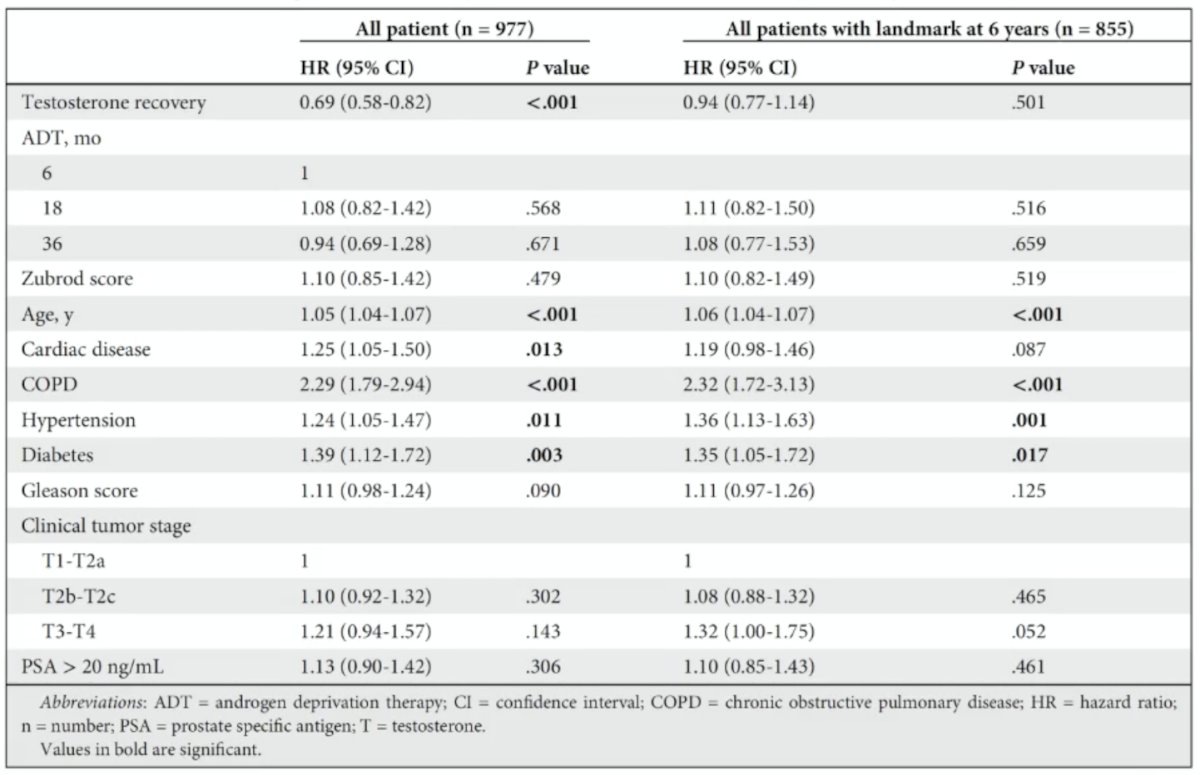
Regarding post-treatment testosterone, Nabid et al.2 used data from 1,230 patients from two phase III trials to determine the rate and time of testosterone recovery in patients with localized prostate cancer treated with radiotherapy + 0-, 6-, 18- or 36-months of ADT. In patients recovering normal testosterone, the median time to testosterone recovery increased with ADT duration, ranging from 0.31, 1.64, 3.06, to 5.0 years for the 0-, 6-, 18-, or 36-month schedules, respectively (p < 0.001), and was significantly faster for those with a normal testosterone at baseline (p < 0.001). On multivariable analysis, older age and longer ADT duration are associated with a lower testosterone recovery:
![Regarding post-treatment testosterone, Nabid et al. [2] used data from 1,230 patients from two phase III trials to determine the rate and time of testosterone recovery in patients with localized prostate cancer treated with radiotherapy + 0-, 6-, 18- or 36-month of ADT. In patients recovering normal testosterone, the median time to testosterone recovery increased with ADT duration, ranging from 0.31, 1.64, 3.06 to 5.0 years for the 0-, 6-, 18- or 36-month schedules, respectively (p < 0.001), and was significantly faster for those with a normal testosterone at baseline (p < 0.001). On multivariable analysis, older age and longer ADT duration are associated with a lower testosterone recovery:](/images/com-doc-importer/262-apccc-2026/apccc-2026-the-importance-of-baseline-testosterone-and-testosterone-recovery-in-high-risk-and-locally-advanced-prostate-cancer/image-3.jpg)
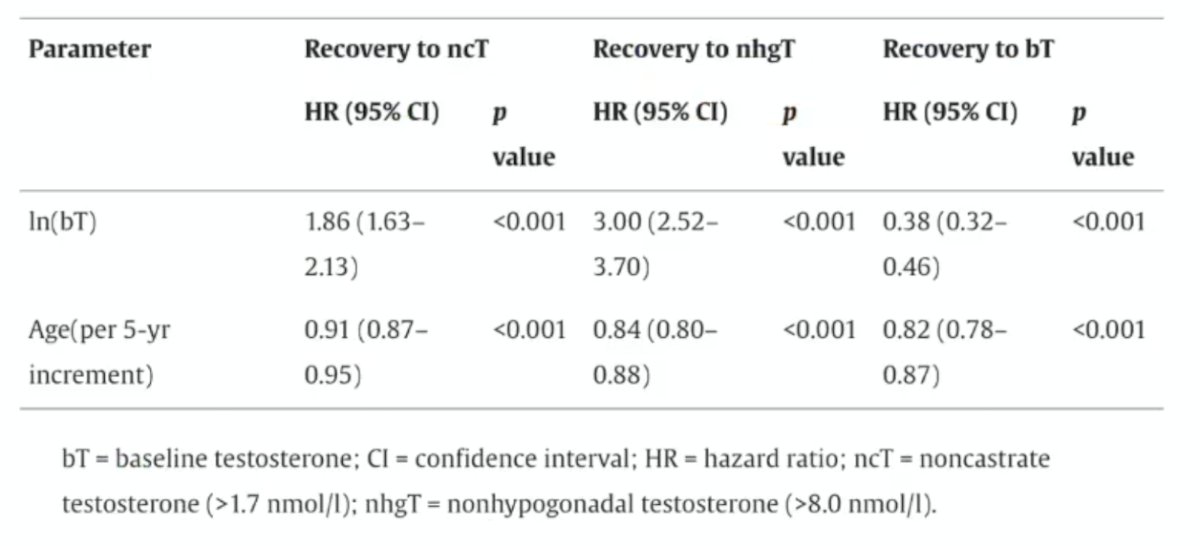
Published in 2025, the TRANSPORT study assessed testosterone recovery following ADT and prostate radiotherapy as a pooled analysis from five randomized trials.3 Among 1,444 men, 115 received 4 months, 880 received 6 months, 353 received 18 months, 36 received 28 months, and 60 received 36 months of ADT. Times to non-castrate testosterone recovery and to non-hypogonadal testosterone recovery varied considerably by ADT duration:
![Published in 2025, the TRANSPORT study assessed testosterone recovery following ADT and prostate radiotherapy as a pooled analysis from five randomized trials [3]. Among 1,444 men, 115 received 4 months, 880 received 6 months, 353 received 18 months, 36 received 28 months, and 60 received 36 months of ADT. Times to non-castrate testosterone recovery and to non-hypogonadal testosterone recovery varied considerably by ADT duration:](/images/com-doc-importer/262-apccc-2026/apccc-2026-the-importance-of-baseline-testosterone-and-testosterone-recovery-in-high-risk-and-locally-advanced-prostate-cancer/image-4.jpg)
Higher baseline testosterone and younger age were associated with a higher likelihood of testosterone recovery (p < 0.001 for both):
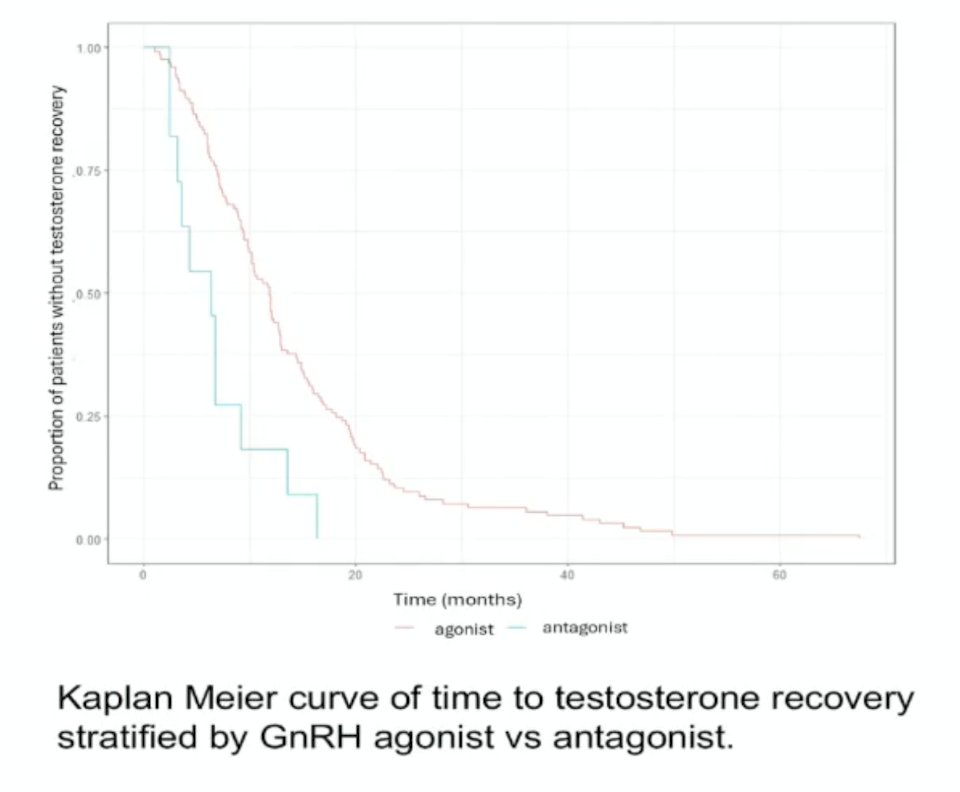
Can post-treatment testosterone recovery be optimized? Presented at ASCO GU 2026, Dr. Gurnani and colleagues performed a retrospective chart review on 191 patients treated with ADT and radiation for localized or regionally advanced prostate cancer at an urban, safety-net hospital between 2013 and 2024. Overall, 91.2% of patients received a GnRH agonist (versus an antagonist). Patients receiving an antagonist had a shorter time to testosterone recovery:
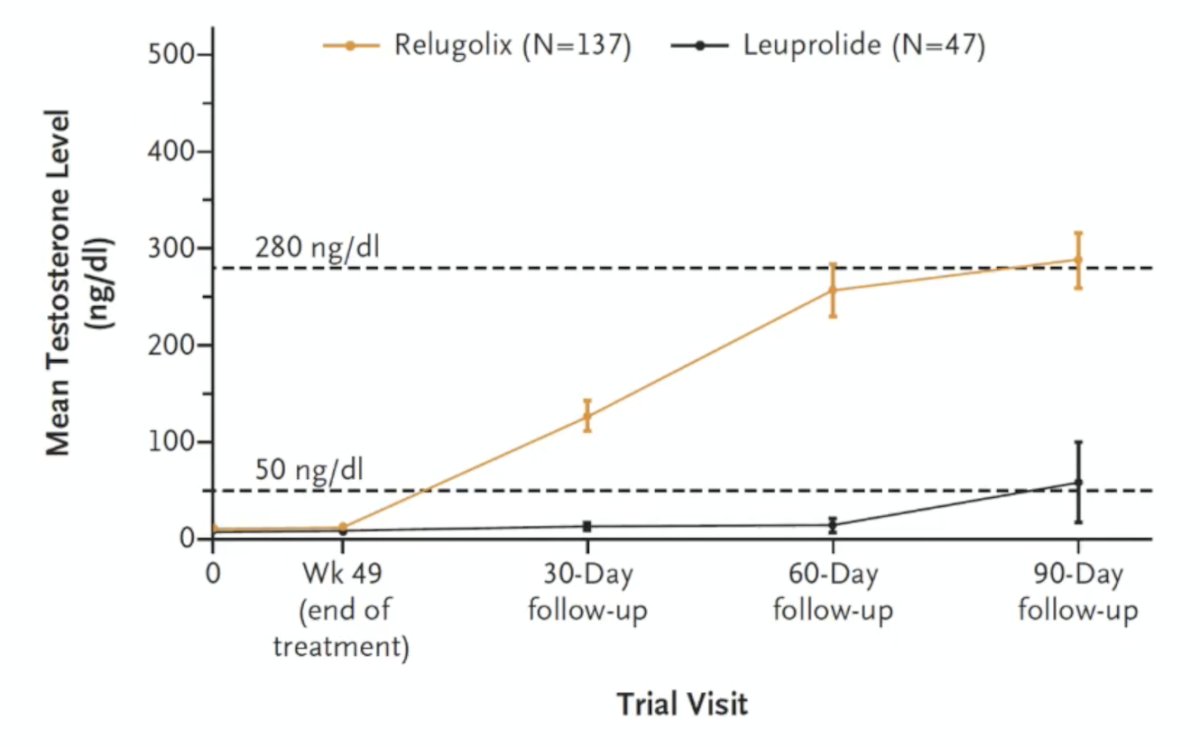
These results were corroborated in the HERO trial,4 whereby patients receiving relugolix had much quicker testosterone recovery compared to those receiving leuprolide:
In 2020, Dearnaley et al.5 assessed relugolix as neoadjuvant/adjuvant ADT to external beam radiotherapy in patients with localized intermediate-risk prostate cancer in a phase 2 trial. They found that 3 months after discontinuing treatment, 52% of men on relugolix and 16% on degarelix experienced testosterone recovery.
Does post-treatment testosterone recovery impact quality of life? Based on the HERO trial, quality of life improves with testosterone recovery, as expected from the intermittent ADT trials: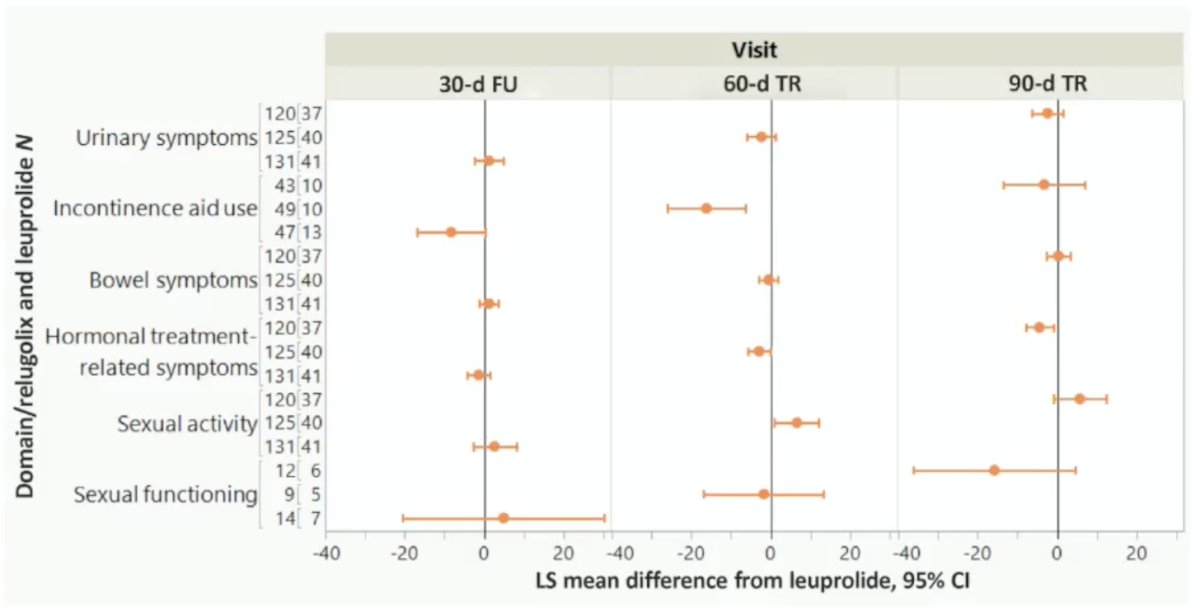
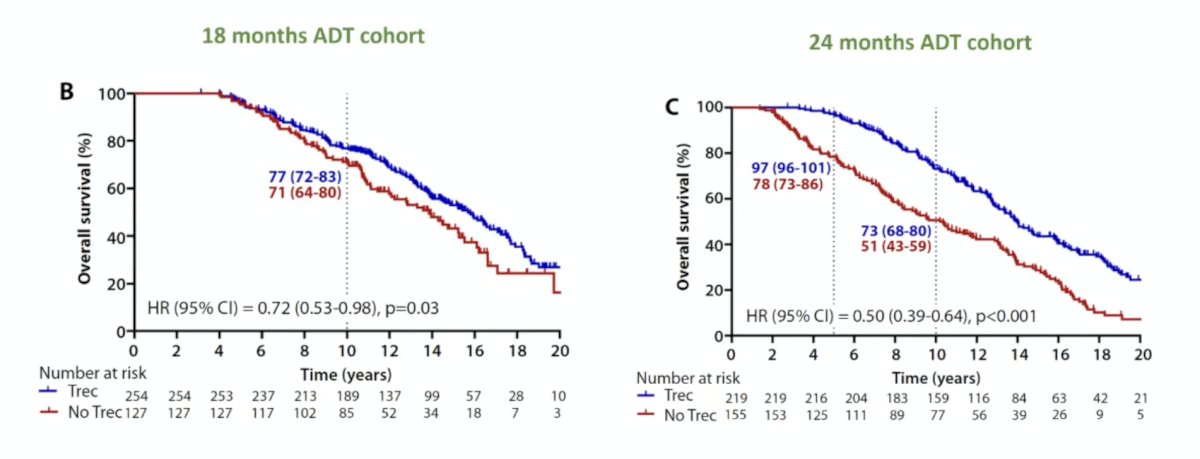
Does post-treatment testosterone recovery impact overall survival? Nabid et al.6 recently reported long-term data from 2 randomized trials with a median follow-up of 16.6 years. Among 6-, 18-, and 36-month ADT cohorts, the 10-year overall survival rates were significantly higher in patients recovering testosterone: 77% versus 61%, p < 0.001; 73% versus 51%, p < 0.001; and 78% versus 62%, p < 0.001:
However, multivariable analyses with landmark time points failed to show testosterone recovery as an independent predictor:
Taken together, the absence of testosterone recovery seems to be associated with worse overall survival.
Dr. Tombal concluded his presentation discussing the importance of baseline testosterone and testosterone recovery by emphasizing that testosterone matters and we should be measuring it at baseline, at least once during treatment, and post-treatment.
Presented by: Bertrand Tombal, MD, PhD, Chairman of the Department of Surgery and Professor of Urology, Université Catholique de Louvain (UCL), Cliniques Universitaires Saint-Luc, Woluwe-Saint-Lambert, Belgium
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 Advanced Prostate Cancer Consensus Conference (APCCC), Lugano, Switzerland, Thurs, April 30 – Sat, May 2, 2026.
- Bryant AK, McKay RR, Kader AK, et al. Subcastrate testosterone nadir and clinical outcomes in intermediate- or high-risk localized prostate cancer. Int J Radiat Oncol Biol Phys. 2019 Apr 1;103(5):1068-1076.
- Nabid A, Carrier N, Vigneault E, et al. Testosterone recovery after androgen deprivation therapy in localized prostate cancer: Long-term data from two randomized trials. Radiother Oncol. 2024 Jun:195:110256.
- Ong WL, Romero T, Roy S, et al. Testosterone recovery following androgen suppression and prostate radiotherapy (TRANSPORT): A pooled analysis of five randomized trials from a meta-analysis of randomized trials in cancer of the prostate (MARCAP) consortium. Eur Urol. 2025 Jan;87(1):49-57).
- Shore ND, Saad F, Cookson MS, et al. Oral Relugolix for Androgen-Deprivation Therapy in Advanced Prostate Cancer. N Engl J Med. 2020 Jun 4;382(23):2187-2196.
- Dearnaley DP, Saltzstein DR, Sylvester JE, et al. The oral gonadotropic-releasing hormone receptor antagonist relugolix as neoadjuvant/adjuvant androgen deprivation therapy to external beam radiotherapy in patients with localized intermediate-risk prostate cancer: A randomized, open-label, parallel-group phase 2 trial. Eur Urol. 2020 Aug;78(2):184-192.
- Nabid A, Carrier N, Vigneault E, et al. Impact of persistent hypogonadism on overall survival after androgen deprivation therapy in localized prostate cancer patients: Long-term prospective data. Int J Radiat Biol Phys. 2026 Mar 1;124(3):654-661.