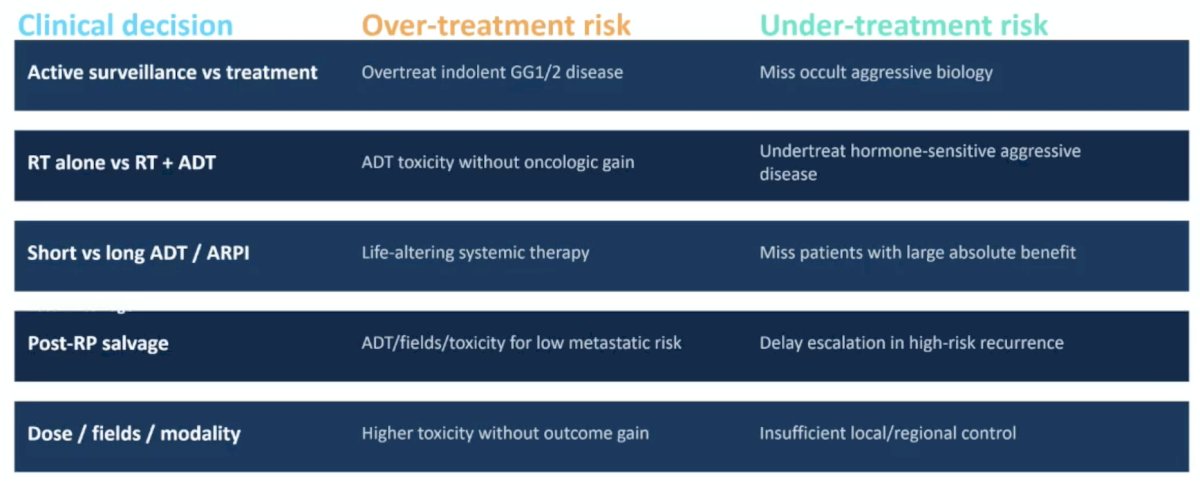
(UroToday.com) The 2026 Advanced Prostate Cancer Consensus Conference (APCCC) meeting featured a high-risk and locally advanced prostate cancer session and a presentation by Dr. Jason Efstathiou discussing whether genomics and artificial intelligence can help to minimize over- or undertreatment. Dr. Efstathiou started his presentation by demonstrating clinical decisions where we are over- and under-treating patients, including: (i) active surveillance versus treatment, (ii) radiotherapy alone versus radiotherapy + ADT, (iii) short versus long ADT/androgen receptor pathway inhibitors, (iv) post-radical prostatectomy salvage, and (v) dose/fields/modality of treatment:
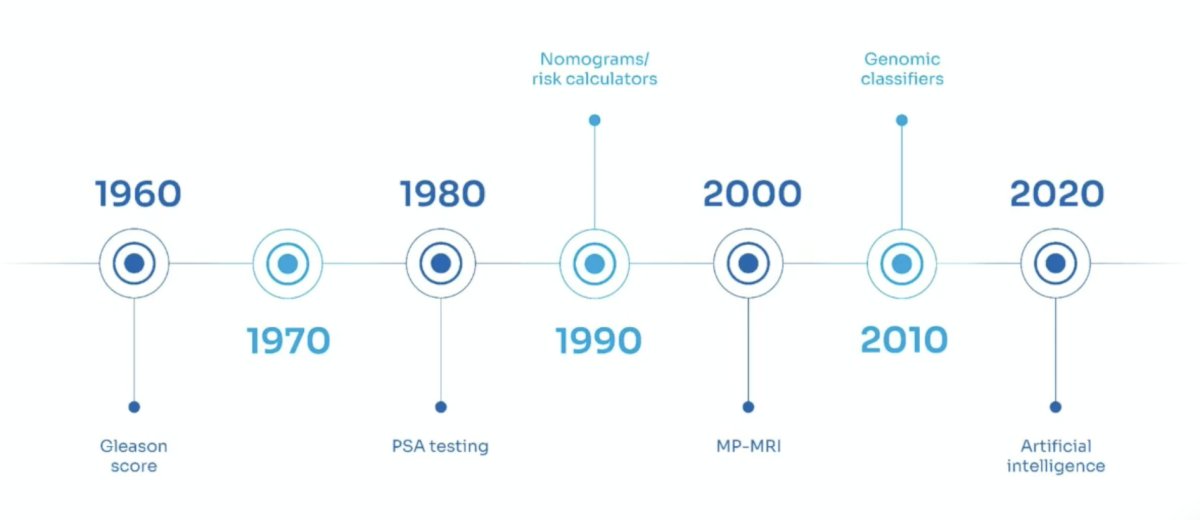
Since the 1960’s, we have had an evolution of risk stratification tools, including the Gleason Score in 1960, all the way to artificial intelligence in 2020:
Specific to genomic and MMAI biomarkers, are the following clinical options:

Of note, Decipher GC and MMAI (ArteraAI Prostate Test) are both highlighted in the 2026 NCCN Prostate Cancer guidelines. Dr. Efstathiou notes that genomics versus artificial intelligence are two very different biomarkers, both valid, but not interchangeable. Decipher GC is a 22-gene expression classifier, with a continuous 0-1 score. Decipher GC is prognostic for distant metastasis and prostate cancer mortality, and validated across biopsy, post-radical prostatectomy, high-risk, and salvage settings. The same assay is often used across different clinical scenarios. The ArteraAI Prostate Test is an MMAI model using H&E image features + clinical variables, with the model output depending on the case use. The MMAI model is both prognostic and predictive, and no extra tissue extraction is needed beyond the digitized slides. The model endpoint defines what the algorithm “cares” about:

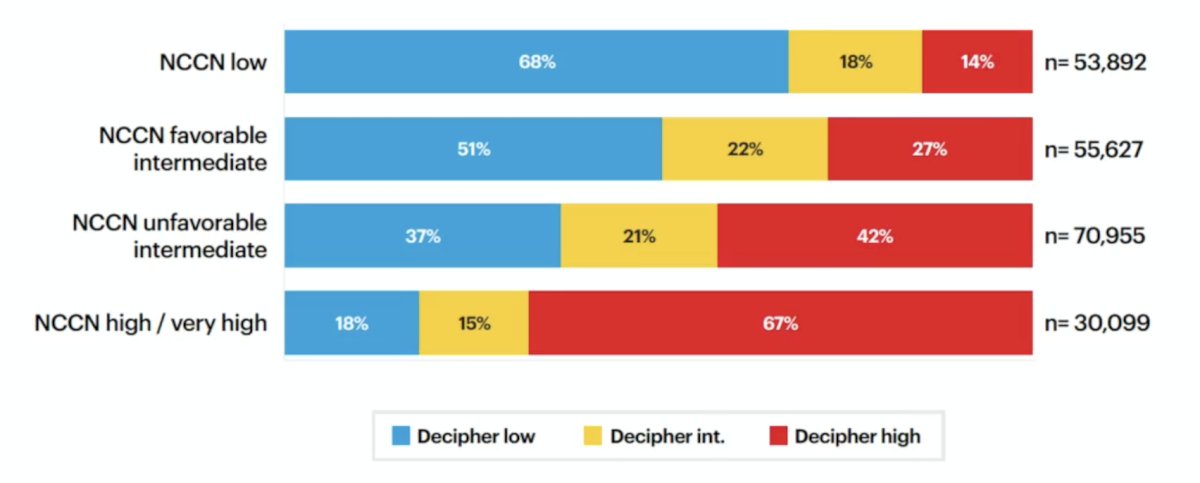
The Decipher GC risk distribution by NCCN risk group is highlighted in the following figure:
Regarding the ArteraAI Prostate MMAI model, within NCCN intermediate risk and high risk groups, the prognostic test reclassifies the majority of patients to a lower risk class:

Dr. Efstathiou cautions that prognosis is not the same as treatment selection. It is important to assess:
- Analytical validity: Can the test be run reproducibly?
- Prognostic validity: Does it predict the patient’s baseline risk?
- Predictive validity: Does it identify differential benefit from a therapy?
- Clinical utility: Does using it improve decisions and outcomes?
A practical rule is that a biomarker should change treatment only when it changes the estimated absolute benefit, harms, or patient preference enough to alter the decision.
Dr. Efstathiou then discussed each of the clinical decisions in more detail, starting with clinical decision #1: active surveillance versus definitive treatment, with the goal of avoiding treating indolent cancer while not missing occult aggressive biology:

The evidence for this approach is that a Decipher high-risk score is associated with higher upgrading/upstaging/adverse pathology risk in favorable risk cohorts. GPS and Prolaris have lower risk selection roles, but often rely on management change endpoints. Several points of caution are that active surveillance is not binary, and biomarkers may change surveillance intensity, not just treatment. Threshold should not override MRI information, biopsy grade, positive cores, life expectancy, or patient priorities.
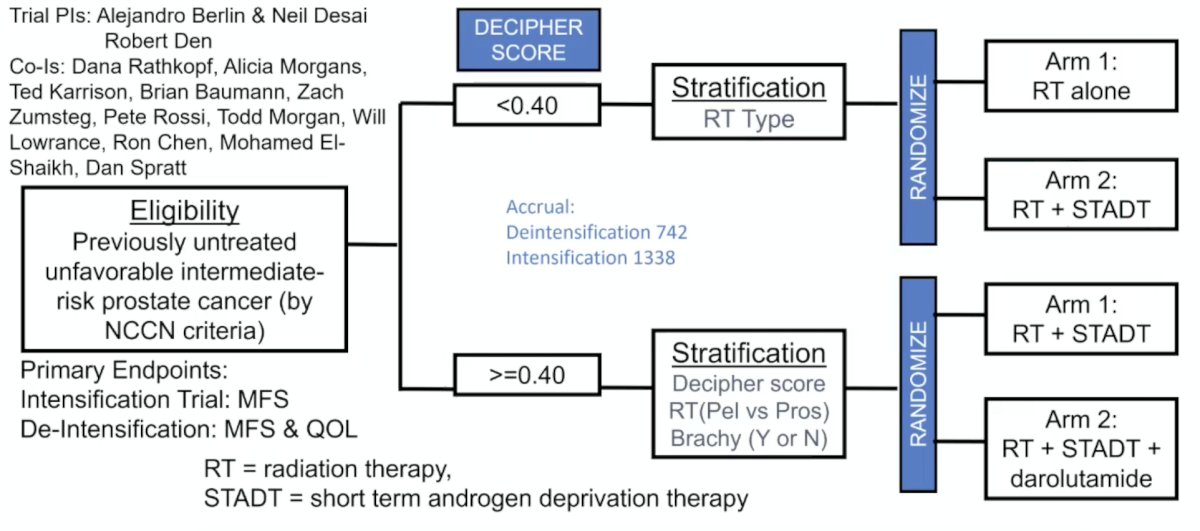
Clinical decision #2: Should intermediate risk patients receive short-term ADT? RTOG 9408 assessed radiotherapy +/- 4 months of ADT, with a primary endpoint of distant metastasis and a secondary endpoint of prostate cancer-specific mortality. The ArteraAI Prostate MMAI model showed that in the biomarker-negative subgroup, there was no clear outcome benefit from ADT, whereas for the biomarker-positive subgroup, there was a higher estimated absolute benefit. Dr. Efstathiou notes that this is commercially relevant because it addresses a common de-escalation question. Regarding Decipher GC, there are prospective trials underway, including the NRG-GU010 GUIDANCE trial among unfavorable intermediate risk disease. Decipher GC low score is testing de-intensification of treatment, whereas Decipher GC high score will test treatment intensification. The primary endpoint for this trial is distant metastasis. Dr. Efstathiou cautions that the endpoint matters: a model trained to avoid metastasis may not be designed to predict biochemical recurrence or ADT delayed PSA events. The trial schema for NRG-GU010 GUIDANCE is as follows:
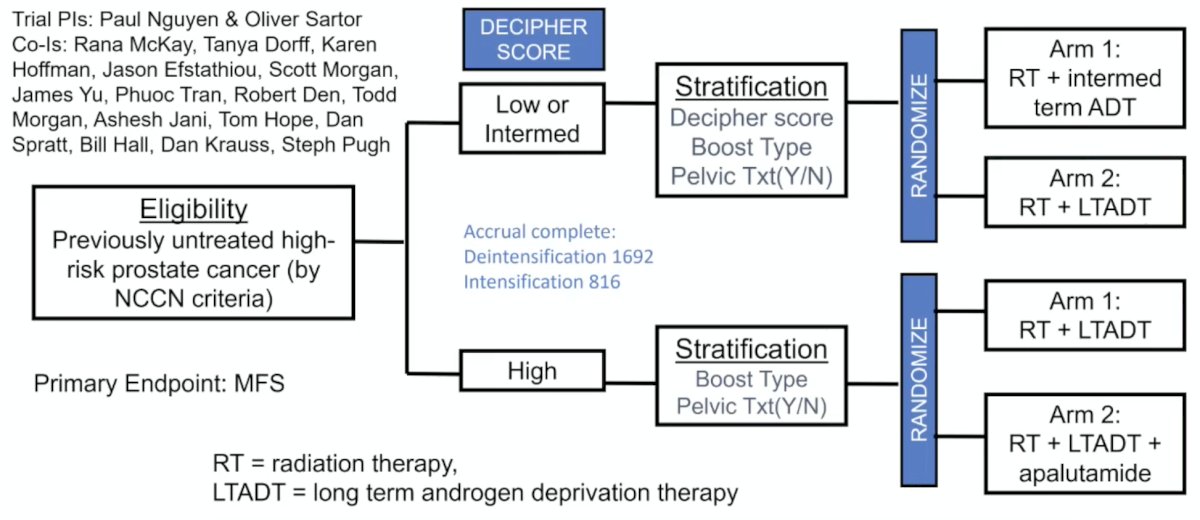
Clinical decision #3: high-risk therapy duration and intensification. In this context, Decipher GC has been validated in high-risk NRG/RTOG trial cohorts, and GU009 is assessing Decipher-guided de-/intensification, with accrual completed in August 2025. NRG GU009 (PREDICT-RT) is a parallel phase III randomized trial for high-risk prostate cancer testing treatment de-intensification for me with lower genomic risk and treatment intensification for men with higher genomic risk:
There are two ArteraAI Prostate MMAI studies in this disease space, including RTOG 9202 validation among high-risk/locally advanced prostate cancer, of which patients received 4 versus 28 months of ADT + radiotherapy.2 For biomarker-positive patients, long-term ADT improved metastasis-free survival and reduced distant metastasis; for biomarker-negative patients, there was no clear benefit observed. The second study assessed the artificial intelligence biomarker in STAMPEDE, with STAMPEDE M0 patients who are treatment-intensified having a clinical benefit for very high-risk patients.3 Biomarkers may identify clinically high-risk, but biologically very high-risk patients. However, prospective androgen receptor pathway inhibitor treatment biomarker trials are still key.
Clinical decision #4: post-prostatectomy salvage – when is “more” justified? Decipher GC has been tested in RTOG 9601, where the genomic classifier is independently associated with distant metastasis, prostate cancer-specific mortality, and overall survival. A higher genomic classifier score demonstrated a larger estimated absolute benefit from adding bicalutamide. The ArteraAI Prostate MMAI model improved prognostic discrimination,4 and PAM50 luminal B showed a predictive signal for apalutamide, benefiting these patients in the BALANCE trial (presented at ASTRO 2025). Dr. Efstathiou’s clinical takeaway is that we should use biomarkers to estimate absolute recurrence/metastasis risk and systemic therapy benefit. We should also avoid treating every PSA risk as biologically identical.
Clinical decision #5: beyond systemic therapy – radiation dose, fields, and toxicity. PORTOS is a predictive 24-gene signature for radiation response, which may identify who benefits from dose escalation. PROSTOX is a germline miRNA toxicity biomarker with the potential to identify patients at higher genitourinary toxicity risk after stereotactic body radiotherapy.
To date, Decipher GC versus ArteraAI Prostate MMAI only shows moderate concordance:
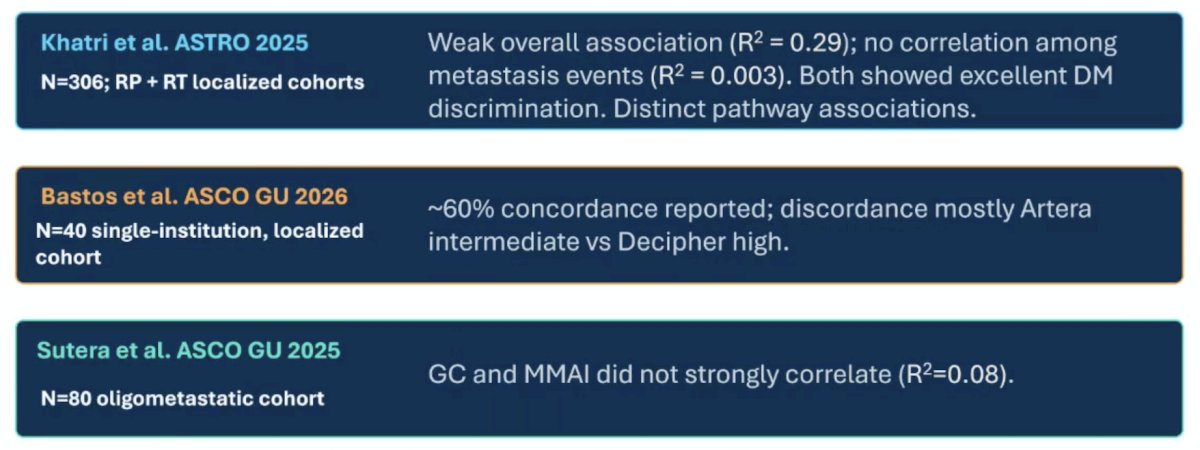
Dr. Efstathiou’s interpretation is that discordance is not necessarily an error – it may be complementary biology, but discordance creates a treatment dilemma that requires endpoint-specific reasoning. For clinical integration, he notes the following 4-step clinical algorithm:
- Start with clinical risk: NCCN risk, MRI, PET where indicated, age, comorbidity, patient goals
- Choose the biomarker for the decision: prognosis? ADT benefit? Long-term ADT? Androgen receptor pathway inhibitor? Radiotherapy dose? Toxicity?
- Translate to absolute benefit: estimate distant metastasis/metastasis-free survival/prostate cancer-specific mortality benefit and competing harms; avoid binary threshold overreach
- Act with confidence only where evidence fits: escalate/de-escalate when validation, endpoint, and patient preference align
Dr. Efstathiou also provided the following cautions before using genomics and artificial intelligence to de-escalate:
- Continuous scores become imprecise when forced into binary (arbitrary) cutoffs: ask where the patient sits within the score distribution.
- Endpoint mismatch can mislead: distant metastasis/metastasis-free survival, prostate cancer-specific mortality, biochemical recurrence, toxicity, and quality of life answer different questions
- Training data define the population: archived trials, older radiotherapy doses, race/ancestry representation, and tissue availability can affect calibration
- Treatment was not always randomized for the biomarker question: Post-hoc and retrospective analyses are hypothesis-generating unless tested prospectively
- Discordance requires humility: a “low” result in one model can coexist with high risk in another because biology and endpoints differ
Dr. Efstathiou concluded his presentation discussing whether genomics or artificial intelligence can help to minimize over- or undertreatment with the following take-home points:
- Reduce overtreatment: when low absolute benefit and high harm are both credible
- Reduce undertreatment: when biology indicates a higher risk than clinical staging alone
- Improve discussions: when uncertainty and absolute benefit are transparent
- Genomics and artificial intelligence can personalize prostate cancer care, but the next advance is not a universal winner test. It is integrated, endpoint-aware decision support, ideally confirmed prospectively
Presented by: Jason Efstathiou, MD, DPhil, FASTRO, FACRO, Professor of Radiation Oncology, Harvard Medical School, Vice-Chair of Faculty & Academic Affairs and Director of the Genitourinary (GU) Division in the Department of Radiation Oncology, Clinical Co-Director of The Claire and John Bertucci Center for Genitourinary Cancers, Massachusetts General Hospital, Boston, MA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 Advanced Prostate Cancer Consensus Conference (APCCC), Lugano, Switzerland, Thurs, April 30 – Sat, May 2, 2026.
- Spratt DE, Tang S, Sun Y, et al. Artificial Intelligence Predictive Model for Hormone Therapy Use in Prostate Cancer. NEJM Evid 2023;2(8).
- Armstrong AJ, Liu VYT, Selvaraju RR, et al. Development and validation of an artificial intelligence digital pathology biomarkers to predict benefit of long-term hormonal therapy and radiotherapy in men with high-risk prostate cancer across multiple phase III trials. J Clin Oncol. 2025 Nov 10;43(32):3494-3504.
- Parker CTA, Mendes L, Liu VYT, et al. External validation of a digital pathology-based multimodal artificial intelligence-derived prognostic model in patients with advanced prostate cancer starting long-term androgen deprivation therapy: A post-hoc ancillary biomarkers study of four phase 3 randomized controlled trials of the STAMPEDE platform protocol. Lancet Digital Health. 2025 Jul;7(7):100885.
- Morgan TM, Ren Y, Tang S, et al. Development and validation of a multimodal artificial intelligence-derived digital pathology-based biomarker predicting metastasis among patients with biochemical recurrence after radical prostatectomy in NRG/RTOG trials. Eur Urol. 2025 Dec 22 [Epub ahead of print].