(UroToday.com) The 2026 Advanced Prostate Cancer Consensus Conference (APCCC) meeting featured a high-risk and locally advanced prostate cancer session and a presentation by Dr. Declan Murphy discussing in which patients with high-risk disease surgery alone may be enough and whether there is any added value of surgery if done as part of multimodality treatment in this setting.
Dr. Murphy started his talk by emphasizing that his talk may soon be outdated pending the reporting of the PROTEUS trial at ASCO 2026. Nonetheless, he noted that there are two key questions regarding surgery in high-risk prostate cancer patients:
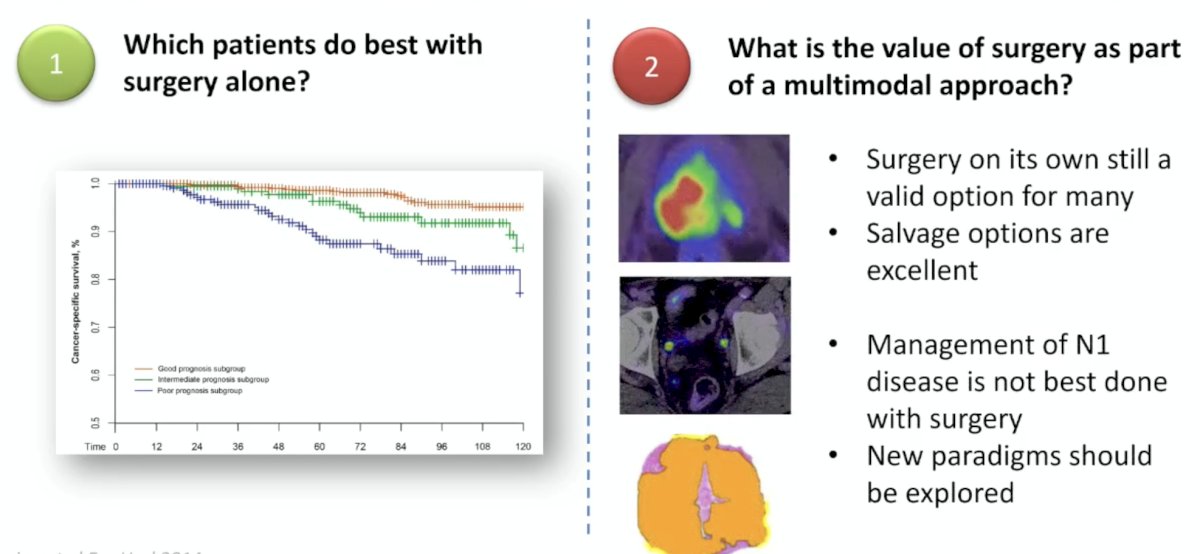
- Which patients do best with surgery alone?
- What is the value of surgery as part of a multimodal approach?
Based on data from the EMPaCT study,1 which assessed outcomes of 1,360 high-risk patients undergoing a radical prostatectomy + extended pelvic lymph node dissection at 8 high-volume centers, not all high-risk prostate cancer is the same:
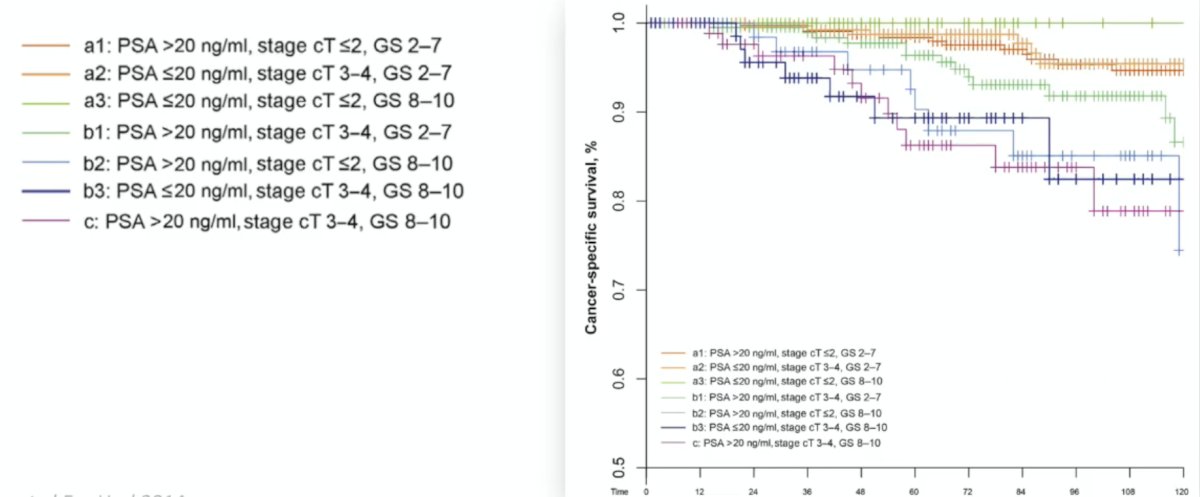
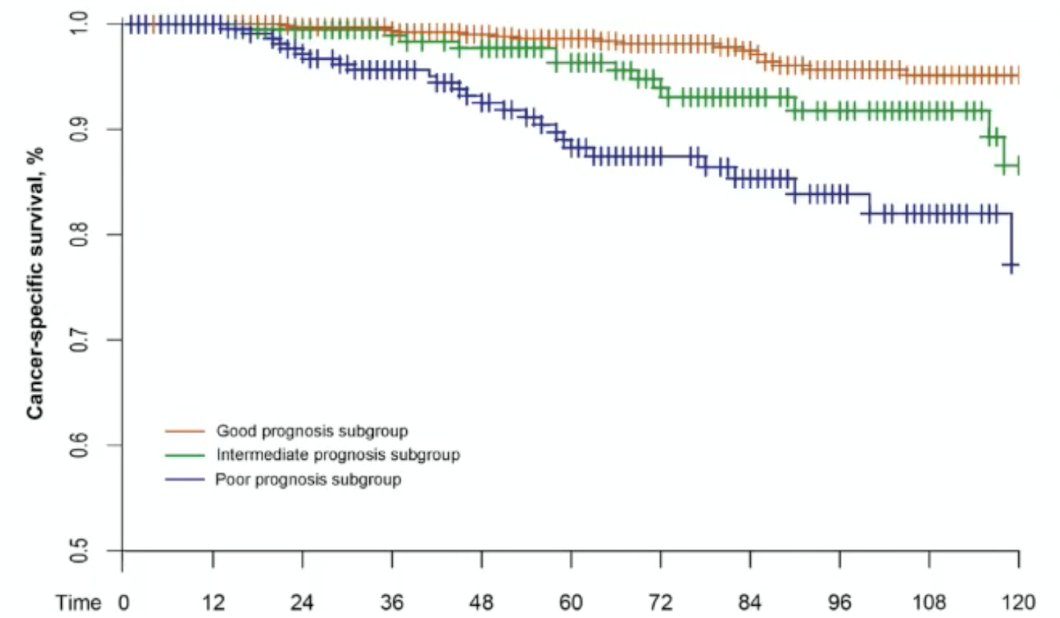
The best outcomes were for patients with a PSA > 20 ng/mL and a Gleason score < 8, whereas the worst outcomes were for a PSA >20 ng/mL, cT3-T4 disease, and a Gleason score 8-10. To simplify stratification further, Joniau and colleagues also stratified patients into tertiles: good, intermediate, and poor prognosis.
In Dr. Murphy’s opinion, there are several factors identifying which patients do best with surgery alone:
- Fit for surgery, accepting a multimodal approach
- Only one high-risk feature, not multiple
- Lower volume high-risk disease
- No very high-risk biology
- Favorable type of high-risk factors
- Negative metastatic staging, ideally with PSMA PET/CT
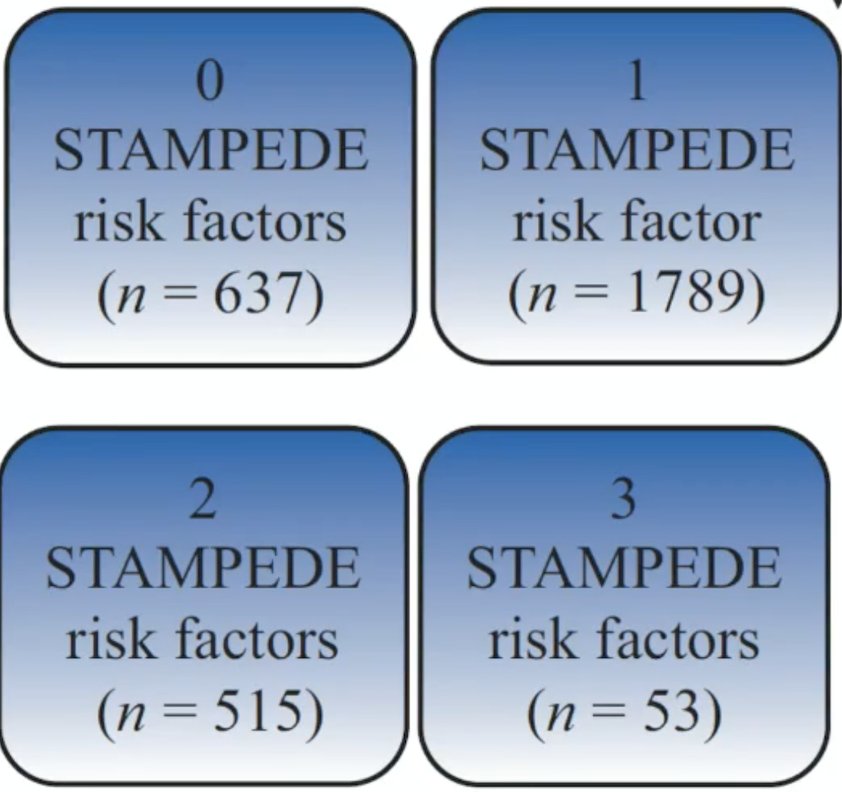
What is the value of surgery as part of a multimodal approach? These patients may be STAMPEDE very high risk, cN1 on conventional imaging, or miN1 based on PSMA PET/CT only. In a subsequent EMPaCT study, Milonas et al.2 assessed long-term cancer-specific survival and overall survival for surgically treated patients with newly diagnosed nonmetastatic node-negative prostate cancer meeting the STAMPEDE criteria for high risk. STAMPEDE high risk included at least two of: PSA > 40 ng/mL, cT3-T4, and Gleason 8-10. The breakdown by number of STAMPEDE risk factors in this study is as follows:
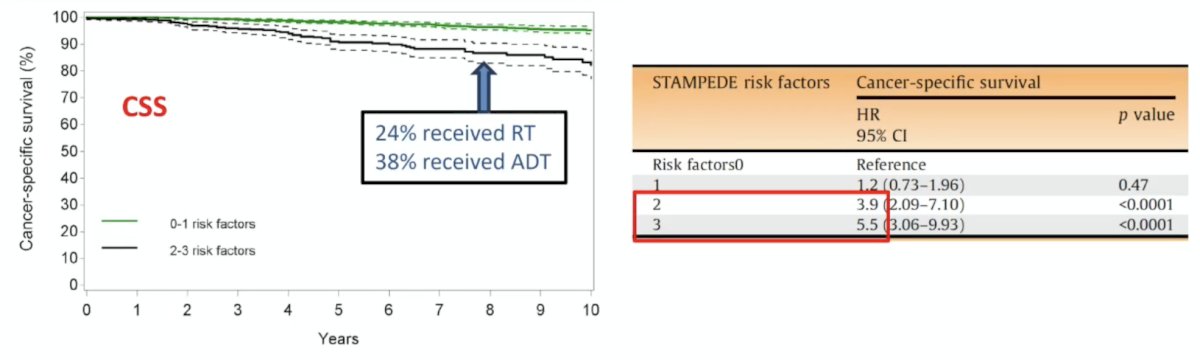
An increasing number of risk factors was significantly associated with worse outcomes:
In the EAU guidelines, the role of pelvic lymph node dissection has been dramatically de-emphasized. In 2023, there was a weak recommendation to perform an extended pelvic lymph node dissection based on the predicted risk of lymph node invasion, and a strong recommendation for performing an extended pelvic lymph node dissection in patients with high-risk prostate cancer. However, in 2024, this recommendation for high-risk patients was changed to “in patients undergoing a lymph node dissection, you should perform an extended pelvic lymph node dissection.” Thus, a pelvic lymph node dissection is no longer recommended for intermediate risk (regardless of PSMA PET/CT) patients, and is optional for high risk disease. For cN1 prostate cancer, the EAU guidelines no longer recommend surgery. The 2024 guidelines provide a weak recommendation for offering radical prostatectomy to patients with cN0 disease as part of multimodal therapy.
What about patients with miN1 prostate cancer? An alternative for surgery and N1 prostate cancer may be to perform a radical prostatectomy, leave the lymph nodes, and then re-stage with PSA and PSMA PET/CT. If the lymph nodes need treatment, patients could then receive pelvic radiotherapy +/- systemic therapy.
Dr. Murphy concluded his presentation discussing in which patients with high-risk disease surgery alone may be enough, and whether there is any added value of surgery if done as part of multimodality treatment in this setting by highlighting his answers to these two key surgical questions:
Presented by: Declan Murphy, Urologist and Director of Genitourinary Oncology, Peter MacCallum Cancer Center, Honorary Clinical Professor of Urology, Melbourne University, Melbourne, Australia
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 Advanced Prostate Cancer Consensus Conference (APCCC), Lugano, Switzerland, Thurs, April 30 – Sat, May 2, 2026.
- Joniau S, Briganti A, Gontero P, et al. Stratification of high-risk prostate cancer into prognostic categories: A European multi-institutional study. Eur Urol. 2015 Jan;67(1):157-164.
- Milonas D, Giesen A, Laenen A, et al. Effect of radical prostatectomy on survival for men with high-risk nonmetastatic prostate cancer features selected according to STAMPEDE criteria: An EMPaCT study. Eur Urol Oncol. 2024 Dec;7(6):1478-1486.