(UroToday.com) The 2024 Advanced Prostate Cancer Consensus Conference (APCCC) meeting featured a session on the management of mHSPC, and a presentation by Dr. Christopher Sweeney discussing the management of patients with mHSPC and early progression on combination therapy. Dr. Sweeney notes that his assignment specifically is to discuss how to manage patients that have early progression after <6-12 months of combination therapy for mHSPC. The definition of combination therapy for mHSPC is defined as:
- Testosterone suppression (ADT) + abiraterone or enzalutamide/apalutamide/darolutamide
- +/- docetaxel
- +/- radiation to the prostate
Data from ENZAMET assessing outcomes for patients with mHSPC and early progression on therapy, notes several important findings:1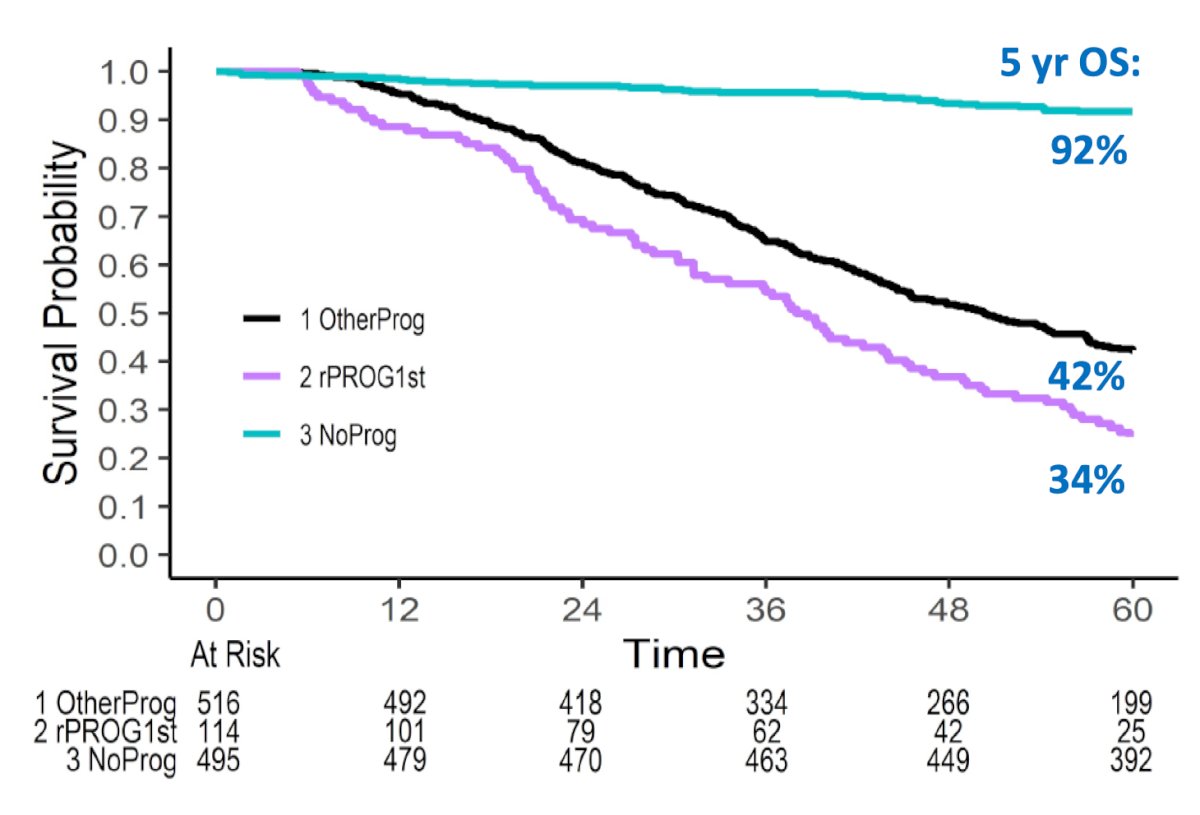
Among all patients in ENAZAMET (+/- enzalutamide), those without progression (teal line) had a 5-year overall survival rate of 92%, which includes 392 patients thus far, and 8% non-prostate cancer-related deaths. For those with PSA progression and subsequent radiographic progression (black line), the 5-year overall survival rate is 42%, and for those with radiographic progression without confirmed prior PSA progression (purple line), the 5-year overall survival rate is 34%. Although early enzalutamide decreased the rate of both types of progression, the hypothesis is that 5-year overall survival is even worse for patients with early disease progression on enzalutamide in the mHSPC setting.
Dr. Sweeney emphasized that it is imperative to define the best first-line mCRPC treatment option for each individual patient, given that no single therapy is best for all patients. Patient and tumor profiling is key, precisely deploying precision/targeted/personalized medicine. Ultimately, our goal is to use as many life-prolonging agents as possible. However, many patients are not able to go from first-line to second-line to third-line mCRPC treatment. For example, ~15% of patients in PSMAfore did not have early cross-over (perhaps secondary to clinical decline?) to LuPSMA in a very stringent clinical trial setting with patients selected as appropriate for hormone switch therapy for CRPC. Thus, it is critical to use the best treatment first in the front line. Profiling each situation is crucial, both at the patient and tumor level. For patient characteristics:
- What prior therapy have they had?
- Docetaxel Y/N
- Radiation to the prostate Y/N
- Are they suitable for docetaxel (or cabazitaxel if they received docetaxel in the mHSPC setting)?
- What access do they have to therapy?
- Assessing regional and personal finances
For tumor characteristics:
- What is the PSMA PET/CT profile?
- What is the tumor exome profile?
- BRCA1, BRCA2, DDR variants
- MSI
- p53, RB1, PTEN
- What is the extent of progression? Oligometastatic or diffuse?
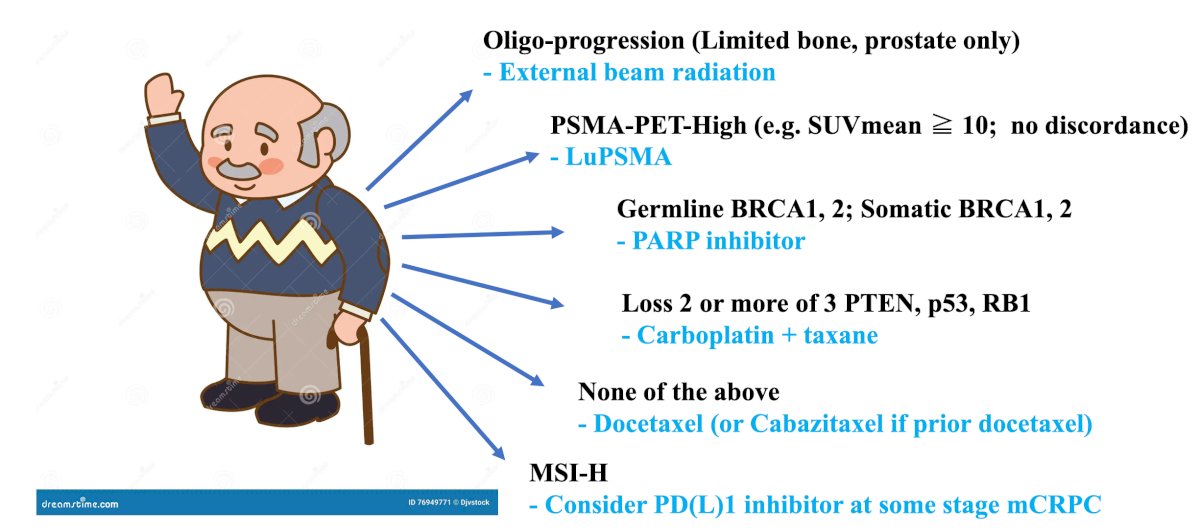
Dr. Sweeney then put forth the following proposal for deploying the best precision medicine as first-line mCRPC therapy:
- Assess for oligo-progression (limited to bone, prostate only): candidacy for external beam radiotherapy
- Assess for PSMA PET high (ie. SUVmean .>= 10, no discordance): candidacy for LuPSMA
- Assess for germline BRCA1/2 and somatic BRCA1/2: candidacy for a PARP inhibitor
- Assess for loss of 2 or more of PTEN, p53, and RB1: candidacy for carboplatin + taxane chemotherapy
- Assess for MSI-H: candidacy for a PD(L)1 inhibitor at some stage of mCRPC
- If they have none of the above: candidacy for docetaxel (or cabazitaxel if they have had prior docetaxel)
Previous work from the Dana Farber Cancer Institute provides evidence for external beam radiotherapy for oligoprogression. Brennan et al.2 evaluated the role of stereotactic body radiotherapy with respect to androgen receptor signaling inhibitors for oligometastatic prostate cancer, noting that complete ablation of lesions leads to improved progression-free survival, compared to incomplete ablation: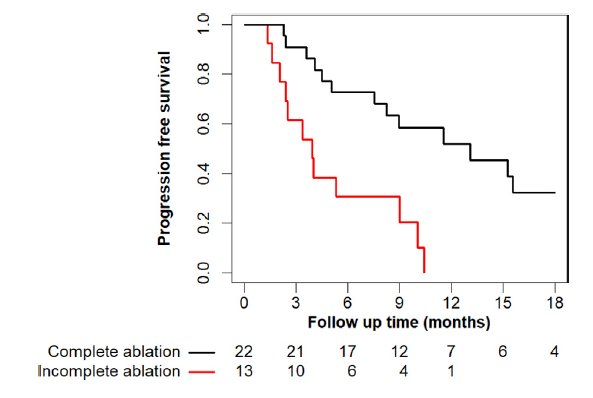
Post-hoc work from the TheraP trial assessed PSMA and FDG-PET as predictive and prognostic biomarkers in patients given LuPSMA versus cabazitaxel for mCRPC.3 There were 35 (35%) of 99 men who were assigned LuPSMA, and 30 (30%) of 101 men who were assigned cabazitaxel that had high PSMA uptake (SUVmean of ≥10). The odds of PSA response to LuPSMA versus cabazitaxel were significantly higher for men with SUVmean of 10 or higher compared with those with SUVmean of less than 10 (OR 12.19, 95% CI 3.42-58.76 vs OR 2.22, 95% CI 1.11-4.51; padj = 0.039 for treatment-by-SUVmean interaction). Among the SUVmean >= 10 patients, LuPSMA had significantly improved PSA progression-free survival compared to cabazitaxel (HR 0.45, 95% CI 0.25-0.80), which was not the case for SUVmean <10 (HR 0.77, 95% CI 0.53-1.12):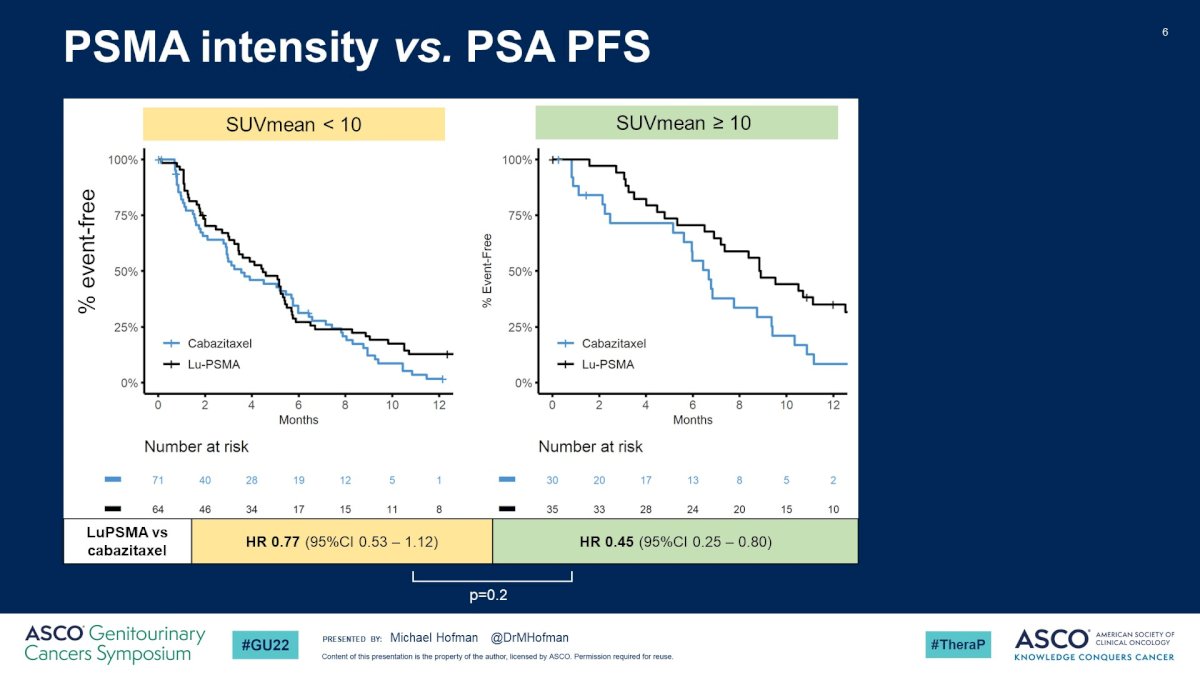
Similar findings were also noted in the VISION trial,4 and presented at ASCO 2022, showing that higher whole-body SUVmean was associated with prolonged radiographic progression-free survival (stratified by SUVmean quartiles):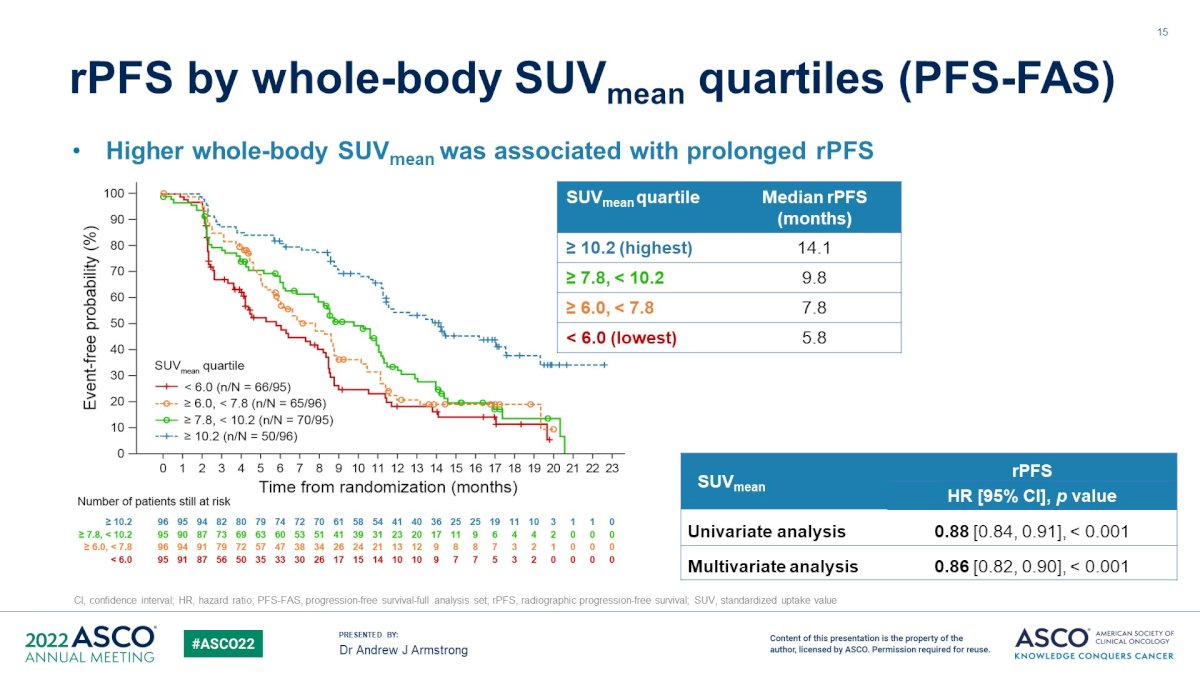
Extended follow-up of the PROfound trial recently published in Journal of Clinical Oncology shows that the clearest overall survival benefit for olaparib is in patients with BRCA1/2 mutations (HR 0.63, 95% CI 0.42 – 0.95):5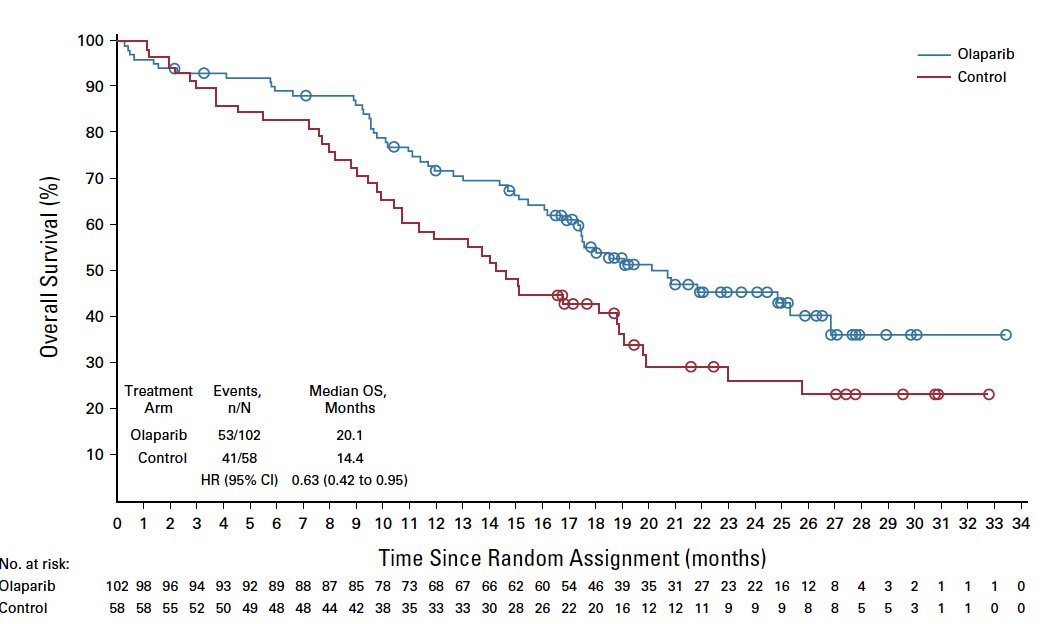
Although an old drug and often overlooked, docetaxel has proven benefit for patients that have no biomarker for guiding therapy. In the TAX-327 trial assessing docetaxel + prednisone versus mitoxantrone + prednisone, more than 90% of patients had two or more hormone manipulations for mCRPC, with docetaxel in this setting having a survival benefit:6![TAX-327 trial [6] assessing docetaxel + prednisone versus mitoxantrone + prednisone](/images/com-doc-importer/156-apccc-2024/apccc-2024-management-of-patients-with-mhspc-and-early-progression-on-combination-therapy/image-6.jpg)
Moreover, both the TROPIC trial7 and the CARD trial8 have shown the benefit of cabazitaxel in the mCRPC setting, with both trials having an overall survival benefit: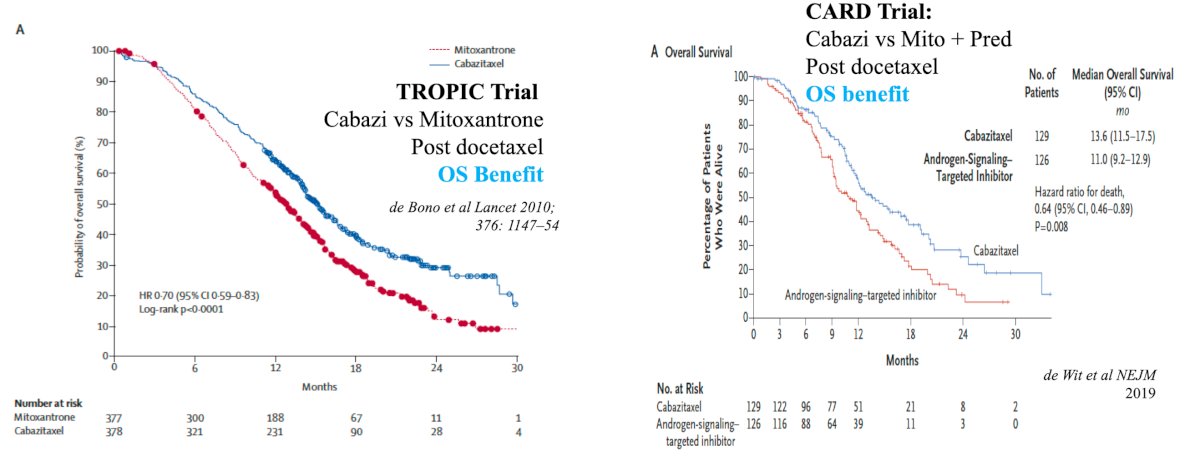
With regards to evidence for carboplatin + taxane chemotherapy, if there is a loss of 2 or 3 tumor suppressor genes (ie. p53, PTEN, RB1), Dr. Sweeney highlighted the MD Anderson Cancer Center study led by Corn et al.9 for patients with mCRPC and mutations in at least two of these three genes. Among the 160 patients in phase 2 portion of the trial, ~30% had prior docetaxel and were subsequently randomized to cabazitaxel plus carboplatin versus cabazitaxel alone. At a median follow-up of 31.0 months (IQR 20.5-37.1), the combination improved the median progression-free survival from 4.5 months (95% CI 3.5-5.7) to 7.3 months (95% CI 5.5-8.2; HR 0.69, 95% CI 0.50-0.95, p = 0.018):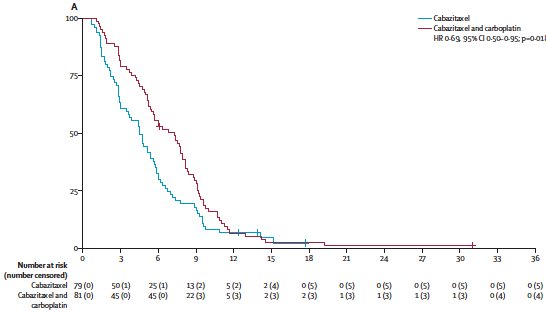
Finally, the evidence for PD1 inhibition in MSI-H CRPC can be derived from the MSKCC IMPACT study,10 which had 23 of 1,033 patients (2.2%) with mCRPC and MSI-H/dMMR mutations. Overall, 11 received anti-PD-1/PD-L1 therapy, six (54.5%) had a greater than 50% PSA decline, and four of whom had radiographic responses. Of the 11 patients, five (45.5%) were still on therapy up to 89 weeks.
Dr. Sweeney concluded his presentation discussing management of patients with mHSPC and early progression on combination therapy by again highlighting the imperativeness of profiling for maximal patient benefit: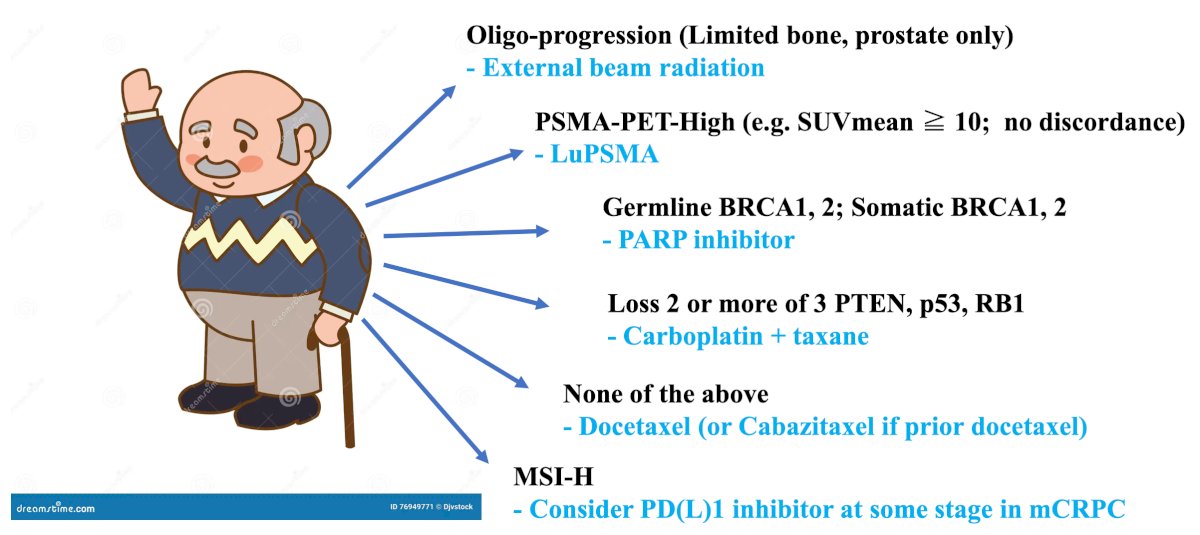
Presented by: Professor Christopher Sweeney, MBBS, Director, South Australian Immunogenomics Cancer Institute, University of Adelaide, Adelaide, Australia
Written by: Zachary Klaassen, MD, MSc - Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2024 Advanced Prostate Cancer Consensus Conference (APCCC) Meeting, Lugano, Switzerland, Thurs, Apr 25 - Sat, Apr 27, 2024.
References:
- Davis ID, Martin AJ, Stockler MR, et al. Enzalutamide with Standard First-Line Therapy in Metastatic Prostate Cancer. N Engl J Med 2019 Jul 11;381(2):121-131.
- Brennan V, Spektor A, Sweeney C, et al. Evaluating the role of stereotactic body radiotherapy with respect to androgen receptor signaling inhibitors for oligometastatic prostate cancer. Adv Rad Oncol. 2022:7:100808.
- Buteau JP, Martin AJ, Emmett L, et al. PSMA and FDG-PET as predictive and prognostic biomarkers in patients given [177Lu]Lu-PSMA-617 versus cabazitaxel for metastatic castration-resistant prostate cancer (TheraP): A biomarker analysis from a randomized, open-label, phase 2 trial. Lancet Oncol. 2022 Nov;23(11):1389-1397.
- Sartor O, de Bono J, Chi KN et al. Lutetium-177-PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. N Engl J Med. 2021 Sep 16;385(12):1091-1103.
- Mateo J, de Bono JS, Fizazi K, et al. Olaparib for the treatment of patients with metastatic-castration-resistant prostate cancer and alterations in BRCA1 and/or BRCA2 in the PROfound trial. J Clin Oncol. 2024 Feb 10;42(5):571-583.
- Tannock IF, de Wit R, Berry WR, et al. Docetaxel plus prednisone or mitoxantrone plus prednisone for advanced prostate cancer. N Engl J Med 2004;351:1502-1512.
- de Bono JS, Oudard S, Ozguroglu M, et al. Prednisone plus cabazitaxel or mitoxantrone for metastatic castration-resistant prostate cancer progressing after docetaxel treatment: A randomised open-label trial. Lancet 2010;376(9747):1147-1154.
- de Wit R, de Bono J, Sternberg CN, et al. Cabazitaxel versus Abiraterone or Enzalutamide in Metastatic Prostate Cancer. N Engl J Med 2019 Dec 26;381(26):2506-2518.
- Corn PG, Heath EI, Zurita A, et al. Cabazitaxel plus carboplatin for the treatment of men with metastatic castration-resistant prostate cancers: A randomized, open-label, phase 1-2 trial. Lancet Oncol. 2019 Oct;20(10):1432-1443.
- Abida W, Cheng ML, Armenia J, et al. Analysis of the prevalence of microsatellite instability in prostate cancer and response to immune checkpoint blockade. JAMA Oncol. 2019 Apr 1;5(4):471-478.
Related Content: