(UroToday.com) In the session of the 2022 Advanced Prostate Cancer Consensus Conference focusing on the treatment of patients with metastatic castration-resistant prostate cancer (mCRPC), Dr. Pritchard presented on the role of tumor genomic profiling, and the potential pitfalls. He first enumerated a potentially emerging model for patients with prostate cancer in which germline, tumor-, and liquid-biopsies are evaluated in order to inform treatment decisions (guided by germline and somatic findings). Further, these findings allow for genetic counselling of family members.
He noted that, in the context of prostate cancer, there are two relevant subtypes of DNA repair defects: homologous recombination repair (HRR) and mismatch repair (dMMR). Each of these are associated with different gene alterations, associated syndromes, and therapeutic approaches.

There are three relevant FDA-approved agents, based on these DNA repair mutations: the PARP inhibitors rucaparib and olaparib and the immune checkpoint inhibitor pembrolizumab. In each case, these treatments are indicated for advanced disease that has progressed on standard treatment approaches including novel hormonal therapy or taxane chemotherapy. Among patients with metastatic prostate cancer, BRCA2 is the most commonly identified germline mutation, and second only to TP53 when considering somatic mutations. Certain characteristics including family history as well as histologic findings (such as ductal and intraductal histology) may be enriched in patients with particular genetic changes.

He noted, however, that these DDR genes are not created equal: while some are strongly associated with prostate cancer risk, others are not. Further, the strength of data to support specific therapeutic interventions varies between each of these genes. For mismatch repair genes, this is unlikely to be therapeutically actionable in the absence of microsatellite instability.
Dr. Pritchard emphasized the importance of genomic pre-analytic processes and services. In particular, the involvement of a pathologist to review and ensure the quality of data is critical to ensuring reliable and actionable results. He emphasized that this is of particular importance in the assessment of liquid biopsy. Considering the integration of these pre-analytic processes, he emphasized that “garbage in” to the genomic analysis will lead to “garbage out”, limiting the clinical actionability of the testing.
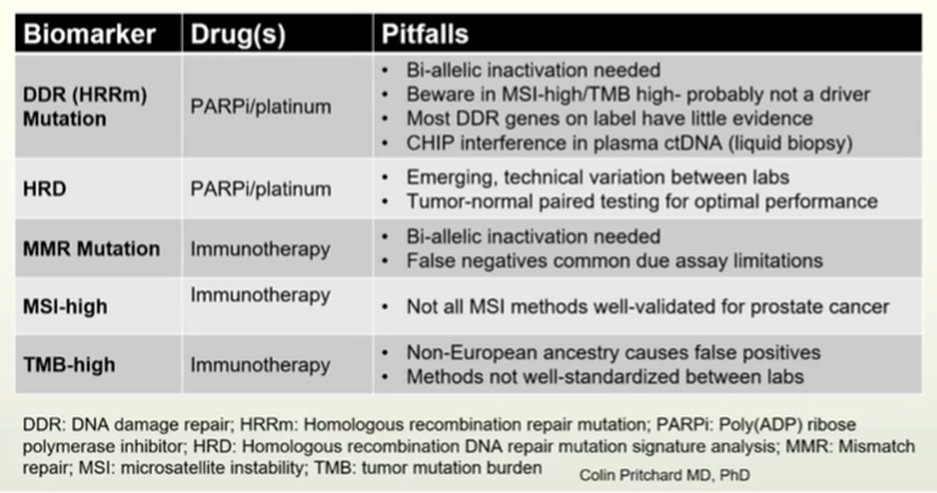
He then specifically discussed some pitfalls in the testing of DNA damage repair (homologous recombination repair) genes, particularly emphasizing the important (but difficult) task of identifying and confirming bi-allelic inactivation. He noted that an HRD signature, while somewhat difficult to measure, can support bi-allelic activation. Further, he noted that (unlike ATM), there is no immunohistochemical assay. Further, he noted that among patients with microsatellite instability (MSI-high), when BRCA1 or 2 are detected, these are typically mono-allelic as a passenger mutation. Therapeutically, these patients are typically non-responsive to PARP inhibitors.

Dr. Pritchard noted that this HRD signature is optimally tested using paired tumor and normal tissue. A high level of loss of heterozygosity is noted in these “BRCA-like” tumors. He then provided an example of an HRD test, UW-OncoPlex, highlighting the difference between those with low and high levels of loss of heterozygosity.

He noted that testing methods are more mature for the assessment of microsatellite instability than for HRD. However, while these have been developed and validated in other tumor types such as colon and endometrial cancer, different regions are affected in prostate cancer and there are more complicated underlying genetic changes which can be technically challenging to detect. Because of this difficulty detecting the underlying mutations, he emphasized that a validated next generation sequencing approach for MSI testing outperforms traditional approaches.
In terms of tumor mutational burden, he emphasized the need for prostate cancer specific validation. He noted numerous pitfalls, including false positives among patients with non-European ancestry. In this context, he noted that germline variants may be miscalled as mutations. Thus, tumor only testing will falsely elevate TMB. He further noted the lack of gold standard calibrators for TMB, with varying methods between labs.
He then moved to a discussion of pitfalls related to liquid biopsy. First and foremost, he highlighted the importance of an adequate sample. The ability to obtain an adequate liquid biopsy sample depends on disease burden. He highlighted this point by emphasizing that PSA levels correlate with the likelihood of having an adequate sample. Another major concern is that of CHIP (clonal hematopoiesis of indeterminant potential) interference – a problem that is more common in older patients, driven by mutations in white blood cells. When a plasma only test is performed, it is difficult to distinguish between mutations found in the tumor or in white blood cells. However, if whole blood is tested or a white blood cell control is used, CHIP interference may be accounted for. Dr. Pritchard noted that CHIP may affect PARP inhibitor genes (including ATM and BRCA2) commonly. Thus, when not properly accounted for, patients may appear to be eligible for therapy that they will not benefit from.
Presented by: Colin C. Pritchard, MD, PhD, Professor and Co-Director, Genetics And Solid Tumors Laboratory, Precision Diagnostics Platform Head, Brotman Baty Institute For Precision Medicine, UW Medicine