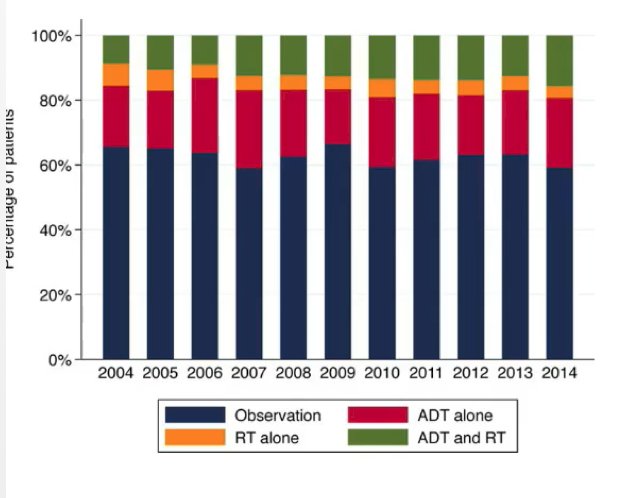
(UroToday.com) The 2022 Advanced Prostate Cancer Consensus Conference (APCCC) Hybrid Meeting included a session on high-risk and locally advanced prostate cancer and a presentation by Dr. Derya Tilki discussing the management of pathologic N1 (pN1) prostate cancer. Dr. Tilki notes that the rates of patients with positive lymph nodes at the time of radical prostatectomy have increased from 3.7% to 10.5% in 2000-2012 compared to 2013-2020. When looking at the distribution of post-RP management strategies for pN1 patients by year of diagnosis, (i) men with higher grade tumors were more likely to be treated with ADT alone than observation, radiotherapy alone, or combination therapy; (ii) men with higher stage tumors +/- positive surgical margins were more likely to receive any treatment than undergo observation, and (iii) men with a higher positive lymph node count were more likely to receive ADT alone compared to all other management strategies:
The premise of ADT alone for pN1 disease is secondary to lymph node metastases at the time of radical prostatectomy traditionally thought to be a manifestation of widely disseminated disease and consequently poor prognosis. This paradigm was the basis for the ECOG randomized trial,1 which showed higher OS among men who received immediate as opposed to delayed ADT. However, recent observational studies have shown the heterogeneity of pN1 prostate cancer, where not all node-positive patients may be affected by systemic disease. This suggests that immediate and lifelong ADT represents overtreatment in many men and that further treatment must be individualized based on risk factors.
In a study by Touijer et al.2 looking at the long-term outcomes of patients with lymph node metastasis treated with radical prostatectomy without adjuvant ADT, they found that 28% of pN1 patients remained free of BCR at 10 years. For patients with recurrence, most recurrences occurred within the first 5 years after surgery. Higher pathological Gleason score and three or more positive lymph nodes were significantly associated with increased risk of BCR and metastasis. Furthermore, the 10-year probability of freedom from distant metastasis was 65%. As follows is the Kaplan-Meier curve for MFS stratified by number of positive lymph nodes:

Additional work from Touijer et al.3 evaluated the association between three different management strategies and survival in prostate cancer with lymph node metastasis after radical prostatectomy. Among 1,338 patients, ADT + EBRT was associated with better OS than ADT alone (HR 0.46, 95% CI 0.32-0.66) or observation (HR 0.41, 95% CI 0.27-0.64). Ten-year mortality risk difference between ADT + EBRT, observation, or ADT alone ranged from 5% in low-risk patients to 40% in high-risk patients. Adjuvant ADT + EBRT was also associated with better CSS than observation or ADT alone (p<0.0001), ADT had better CSS compared to observation (HR 0.64, 95% CI 0.43-0.95):

Given the worse prognosis with the increasing number of positive lymph nodes, whether the association of reduction in mortality risk applies irrespective of the number of positive lymph nodes when using adjuvant radiotherapy was explored after adjusting for the time dependent use and duration of ADT by Dr. Tilki and colleagues in a recent publication in JCO.4 After a median follow-up of 7.02 years, 986 (5.50%) men died, with 223 (22.62%) of prostate cancer. Adjuvant compared with early salvage radiotherapy was associated with a significantly lower ACM risk per unit increase in positive pelvic lymph nodes (adjusted HR 0.92, 95% CI 0.85 to 0.99). Additionally, a significant difference in the 7-year adjusted ACM estimates favoring adjuvant radiotherapy versus early salvage radiotherapy was observed in men with four or more positive lymph nodes (7.74% vs 23.36%), however this was not true for men with 1-3 positive lymph nodes (14.27% vs 13.89):

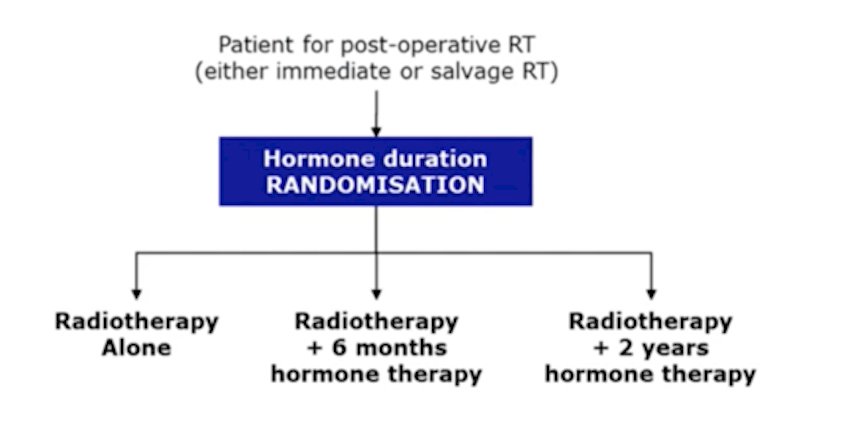
Dr. Tilki notes that the RADICALS-HD trial will assess the optimal duration of ADT for patients treated with post-operative radiotherapy, with the following trial schema:
Chemotherapy has also been assessed in high risk patients (including pN1) in the SPCG-12 trial.5 This trial randomized 459 patients (12% with pN1) after radical prostatectomy to six cycles of docetaxel or surveillance. Over a median follow-up of 56.8 months, there was no improvement in biochemical disease-free survival, defined as a rising PSA of >0.5 ng/mL. The lack of combination of docetaxel to ADT in this trial and the inclusion of patients not classically considered as very high risk for relapse (ie. those with pT2, Gleason 7 cancers) may explain these negative findings.
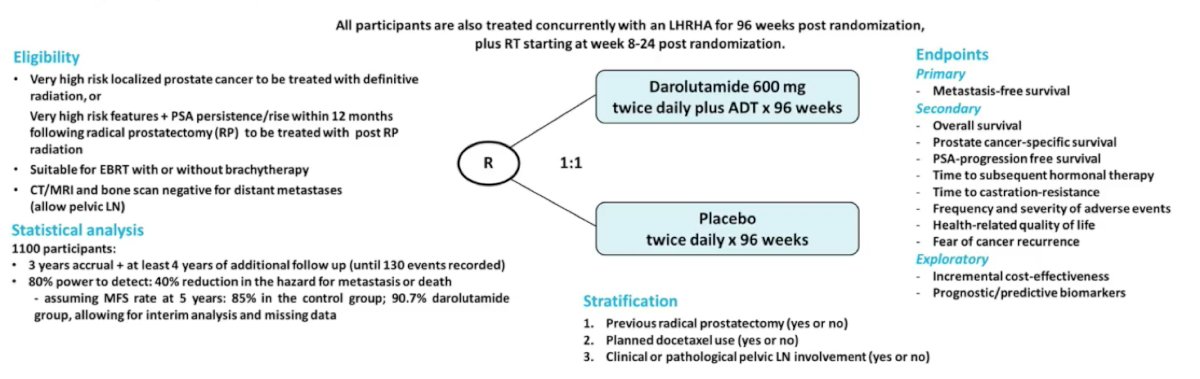
Dr. Tilki notes that the DASL-HiCaP trial (ANZUP 1801) is a randomized, phase 3, placebo-controlled international trial that is testing the addition of darolutamide to ADT and definitive or salvage radiation in very high-risk prostate cancer. This will include men that are planned for radiotherapy who have very high-risk localized prostate cancer on conventional imaging, or very-high risk features with PSA persistence or rise within 1 year following radical prostatectomy. The primary endpoint for this trial is MFS and the trial schema is as follows:
Finally, Dr. Tilki highlighted a systematic review from Marra et al.,6 which included 26 studies with 12,537 men assessing the management of pN1 patients. The 10-year BCR-free rates ranged from 28%-56%, CSS rates from 72%-98%, and the OS rates from 60%-87.6%. While the majority of men with pN1 disease experienced BCR after surgery, long-term disease-free survival has been reported in selected patients. The use of adjuvant radiotherapy with or without ADT has been shown to improve survival in men with locally advanced disease and a higher number of positive lymph nodes. Risk stratification according to pathological Gleason score, number of positive nodes, and pathological stage is key for selection of the optimal postoperative therapy.
Dr. Tilki concluded her presentation by discussing the management of pN1 prostate cancer by noting that according to the EAU guidelines, the uncertainty regarding the optimal management of pN1 disease is reflected in these guidelines, which list observation, adjuvant ADT, and radiotherapy ADT as management options.
Presented by: Derya Tilki, MD, Martini-Klinik Prostate Cancer Center, University Hospital Hamburg-Eppendorf, Hamburg, Germany
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, @zklaassen_md on Twitter during the 2022 Advanced Prostate Cancer Consensus Conference (APCCC) Annual Hybrid Meeting, Lugano, Switzerland, Thurs, Apr 28 – Sat, Apr 30, 2022.
References:- Messing EM, Manola J, Yao J, et al. Immediate versus deferred androgen deprivation treatment in patients with node-positive prostate cancer after radical prostatectomy and pelvic lymphadenectomy. Lancet Oncol 2006 Jun;7(6):472-479.
- Touijer KA, Mazzola CR, Sjoberg DD, et al. Long-term outcomes of patients with lymph node metastasis treated with radical prostatectomy without adjuvant androgen-deprivation therapy. Eur Urol. 2014 Jan;65(1):20-25.
- Touijer KA, Karnes RJ, Passoni N, et al. Survival Outcomes of Men with Lymph Node-positive prostate cancer after radical prostatectomy: A comparative analysis of different postoperative management strategies. Eur Urol. 2018 Jun; 73(6):890-896.
- Tilki D, Chen MH, Wu J, et al. Adjuvant versus early salvage radiation therapy afer radical prostatectomy for pN1 prostate cancer and the risk of death. J Clin Oncol. 2022 March 15 [Epub ahead of print].
- Ahlgren GM, Flodgren P, Tammela TL, et al. Docetaxel versus surveillance after radical prostatectomy for high-risk prostate cancer: Results from the prospective randomized, open-label phase 3 Scandinavian Prostate Cancer Group 12 Trial. Eur Urol. 2018 Jun;73(6):870-876.
- Marra G, Valerio M, Heidegger I, et al. Management of patients with node-positive prostate cancer at radical prostatectomy and pelvic lymph node dissection: A systematic review. Eur Urol Oncol. 2020 Oct;3(5):565-581.