Dr. Beltran began by raising the question of the degree to which biology underlies known prognostic clinical features in mHSPC. It is well-established that de novo (synchronous) mHSPC is a poor prognostic feature relative to relapsed (metachronous) disease. Likewise, men with high-volume mHSPC have significantly worse prognosis relative to those with low-volume disease. She posed the question as to whether these clinical features are due to inherent biologic differences. Are some tumors more “pro-metastatic” from the start? Or are high-volume tumors just caught later? Developing biomarkers that better reflect biology will help elucidate the mHSPC landscape and guide clinical management.
Several studies provide estimates of genomic alterations in mHSPC, which Dr. Beltran summarized. The most common alterations occurred in TMPRSS2-ERG (40-50%), PTEN (40%), and TP53 (25-45%).

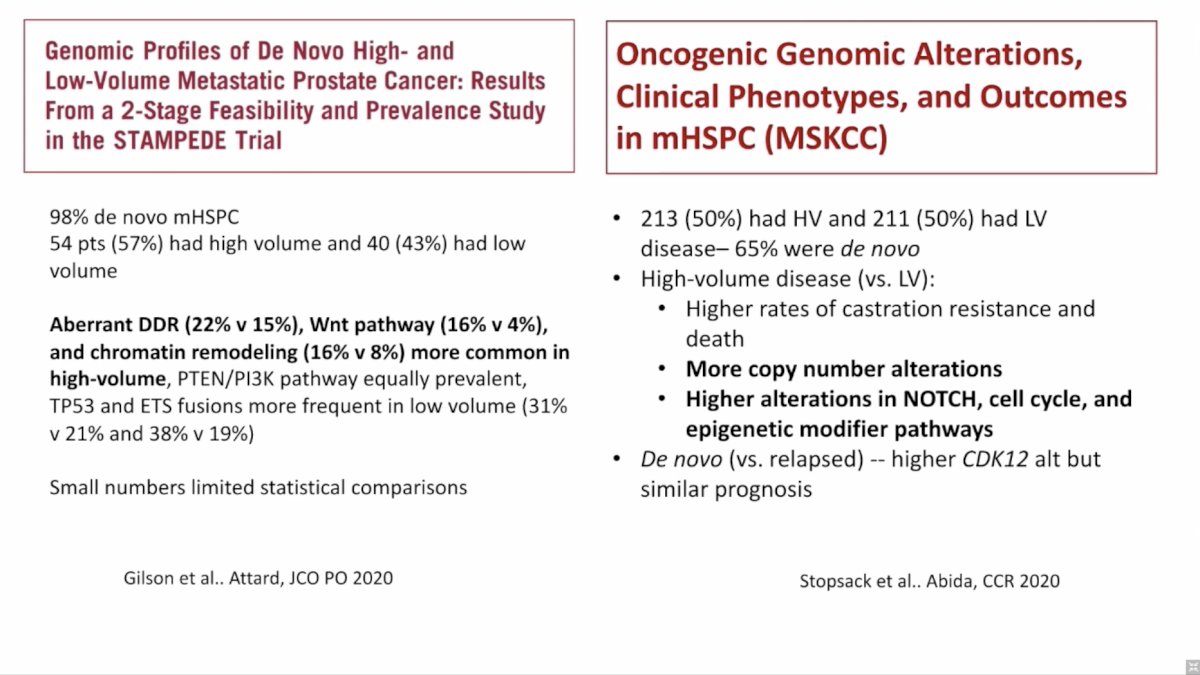
Other studies provide insight into genomic alterations enriched in high volume versus low volume mHSPC, however, there is no “smoking gun” or single molecular feature that underlies the poor prognosis. Alterations in genes involved in DNA damage repair (DDR), Wnt signaling, NOTCH signaling, cell cycle, and epigenetic modification are more common in high volume disease. Dr. Beltran also discussed early versus late (or acquired) genomic events, highlighting TMPRSS2-ERG and SPOP as early events. Alterations in DDR and tumor suppressor genes (RB1, TP53, PTEN) can be early or acquired.
Clinical trials of neoadjuvant therapy prior to radical prostatectomy in clinically localized high-risk prostate cancer provides an opportunity to understand alterations enriched post therapy through paired pre/post-treatment biopsy. For example, in a trial of neoadjuvant ADT plus docetaxel, residual tumors at the time of surgery were enriched for alterations in TP53 and PTEN.[2] Frequency of alterations in these residual tumors reflected those seen in the metastatic setting.

Summarizing available data, Dr. Beltran assigned prognostic impact to certain genomic alteration in mCRPC. SPOP mutations portend good prognosis and better response to AR targeted agents. CDK12 imparts a poor prognosis. Likewise, loss of tumor suppressor genes (RB1, TP53, PTEN) is bad and compound loss (more than one) is worse. Combined loss of RB1 and TP53 has been shown to lead to AR independence and lineage plasticity. While TP53 and PTEN can be early events that are selected for given the fitness they impart, RB1 alterations are often acquired.
Several studies have correlated gene expression profiles with clinical outcomes. The most robust finding is the predictive and prognostic associations of luminal versus basal signatures. Compared to the basal subtype, luminal subtype is associated with greater benefit from docetaxel in the mHSPC setting and greater benefit from AR targeted agents in the non-metastatic and metastatic CRPC setting. This raises the question of how do we best target the basal subtype?

Finally, Dr. Beltran discussed the new molecular data available with PSMA PET scans. PSMA is a cell-surface protein expressed in primary and metastatic prostate cancer. PSMA expression is dynamic and change with treatment and across disease states likely reflecting evolving tumor biology. PSMA-negative lesions have been associated with AR independence, lineage plasticity, and NEPC features. Understanding the biology based on PSMA PET imaging will be an evolving area over the coming years. Specifically, Dr. Beltran is interested to see the response to PSMA therapy in the mHSPC setting and how heterogeneity on PSMA PET impacts treatment response and outcomes.
Dr. Beltran concluded with several take-home points:
- Loss of tumor suppressor genes (RB1, TP53, PTEN) is associated with resistance to AR targeted therapies, but context likely matters (e.g., early versus late); it remains to be seen whether these alterations identify patients who may benefit from chemotherapy intensification (triplet therapy)
- SPOP mutations are associated with sensitivity to AR therapies
- BRCA2, CKD12, PTEN, and microsatellite instability are emerging predictive biomarkers in CRPC; there may be an opportunity to bring them to the earlier disease settings
- Clonal selection and/or acquired loss may occur with CRPC progression and requires further study in the context of AR targeted agents versus chemotherapy in mHSPC as it may impact subsequent therapy
- Gene expression profiles (luminal versus basal) and molecular imaging (PSMA) may help guide future biologic stratification
- Various biomarkers are being incorporated into trials for high-risk localized and mHSPC and integrating data will be critical
Presented by: Himisha Beltran, MD, Medical Oncologist, Dana Farber Cancer Institute, Harvard Medical School
Written by: Jacob Berchuck, MD, Genitourinary Medical Oncologist, Dana-Farber Cancer Institute (Twitter: @jberchuck) during the 2021 Advanced Prostate Cancer Consensus Conference, Saturday, October 9, 2021.
References:- Beltran H, et al. Impact of Therapy on Genomics and Transcriptomics in High-Risk Prostate Cancer Treated with Neoadjuvant Docetaxel and Androgen Deprivation Therapy. Clin Cancer Res. 2017 Nov 15;23(22):6802-6811.