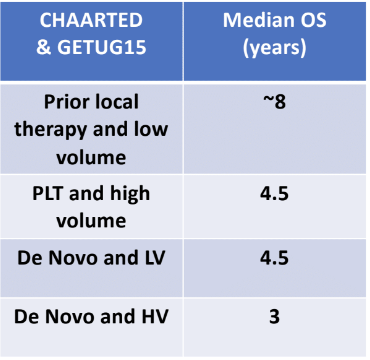
Metastatic hormone-sensitive prostate cancer (mHSPC) patients have a variable response to testosterone suppression, as can be seen in the CHAARTED1 and GETUG 15 trials.2 (Table 1)
Table 1- Different patients have variable response to testosterone suppression:
When assessing the quality of life of these patients – for the ones that received only ADT, the ones with the low-volume disease had no change in the quality of life over 12 months. However, in high volume metastatic disease patients, the quality of life declined, as the disease had progressed. In contrast, for patients who received both ADT and docetaxel: Patients who received ADT only there was a decline in the quality of life for those with low-volume metastatic disease, but for the ones with high-volume metastatic disease there was no decline in quality of life.4
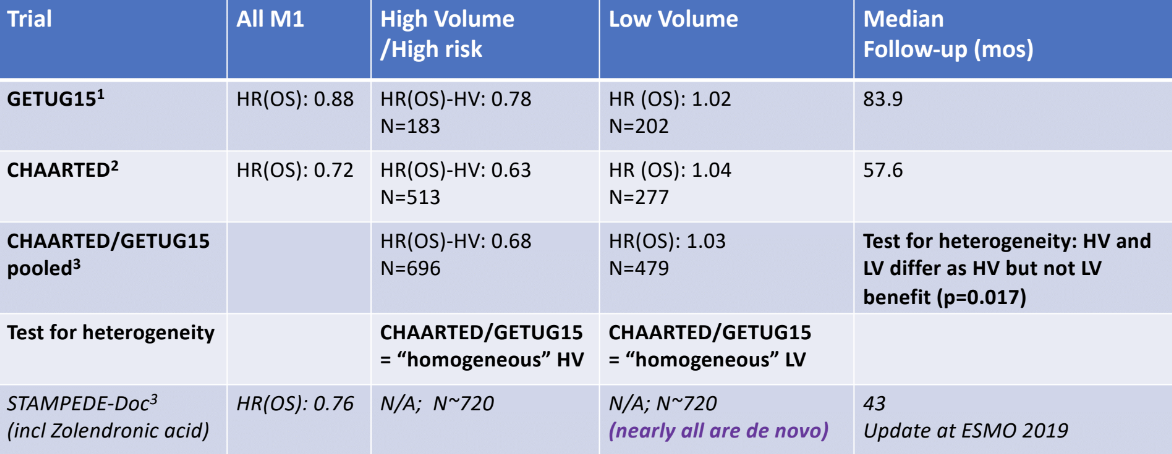
Dr. Sweeney further discussed the effect of these treatments on overall survival, as measured by hazard ratio (HR), which is summarized in Table 2. Docetaxel has a direct overall survival benefit for high-volume disease and there is documented improvement in the quality of life. However, for low-volume disease, there appears to be no overall survival benefit for docetaxel. Disease volume appears to be prognostic for the outcome on ADT and predictive for docetaxel benefit. Does this mean that there are different disease biology processes within mHSPC?
Table 2 – Summary of ADT +/- docetaxel treatment effect on overall survival:
Enzalutamide was the next medication discussed. The ENZAMET trial’s primary endpoint was overall survival difference between mHSPC patients treated with enzalutamide and ADT compared to those treated with ADT alone.7 This trial demonstrated a clear benefit for the enzalutamide treated patients (Figure 1). In this trial, there is a mixed bag of patients with low- and high-volume disease, de novo vs. metachronous metastases, and many permutations. Table 3 demonstrates the scorecard of other medications which are potent direct androgen receptor inhibitors in mHSPC. These include apalutamide and enzalutamide in the ARCHES trial.8
Figure 1 – Enzamet primary endpoint of overall survival showing the benefit in those treated with enzalutamide:
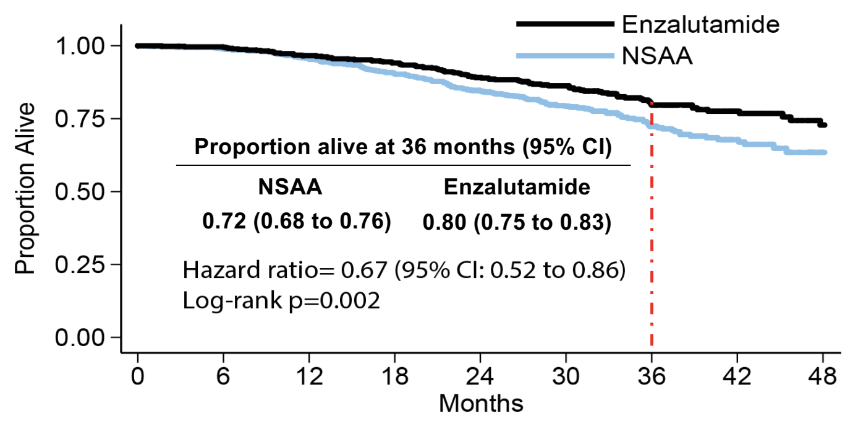
Table 3 – Scorecard of other trials of potent direct androgen receptor inhibitors in mHSPC:
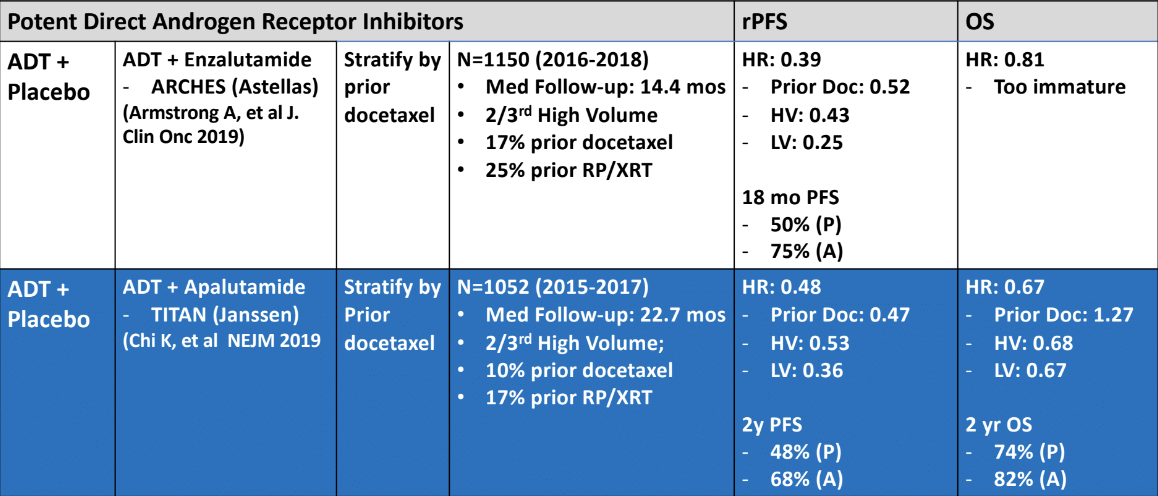
Table 4 – Overall survival treatment benefit in mHSPC patient as of August 2019:

Written by: Hanan Goldberg, MD, Urology Department, SUNY Upstate Medical University, Syracuse, New York, USA, Twitter: @GoldbergHanan, at the 2019 Advanced Prostate Cancer Consensus Conference (APCCC) #APCCC19, Aug 29 - 31, 2019 in Basel, Switzerland
References:
- Sweeney C. et al. Chemohormonal Therapy in Metastatic Hormone-Sensitive Prostate Cancer. New England Journal of Medicine. 2015; 373:737-746
DOI: 10.1056/NEJMoa1503747. - Gravis G. et al. Androgen-deprivation therapy alone or with docetaxel in non-castrate metastatic prostate cancer (GETUG-AFU 15): a randomised, open-label, phase 3 trial. Lancet Oncology. 2013 Feb;14(2):149-58. doi: 10.1016/S1470-2045(12)70560-0.
- Kyriakopolous et al. Chemohormonal Therapy in Metastatic Hormone-Sensitive Prostate Cancer: Long-Term Survival Analysis of the Randomized Phase III E3805 CHAARTED Trial. Journal of Clinical Oncology. 2018 DOI: 10.1200/JCO.2017.75.3657.
- Morgans et al. Quality of Life During Treatment With Chemohormonal Therapy: Analysis of E3805 Chemohormonal Androgen Ablation Randomized Trial in Prostate Cancer. Journal of Clinical Oncology. 2018 Apr 10;36(11):1088-1095. doi: 10.1200/JCO.2017.75.3335.
- Fizazi K. et al. Abiraterone plus Prednisone in Metastatic, Castration-Sensitive Prostate Cancer. New England Journal of Medicine. 2017; 377:352-360
DOI: 10.1056/NEJMoa1704174. - Chi K. et al. Patient-reported outcomes following abiraterone acetate plus prednisone added to androgen deprivation therapy in patients with newly diagnosed metastatic castration-naive prostate cancer (LATITUDE): an international, randomised phase 3 trial. Lancet Oncology. Feb;19(2):194-206. doi: 10.1016/S1470-2045(17)30911-7. 2018.
- Sweeney C. et al. Enzalutamide with Standard First-Line Therapy in Metastatic Prostate Cancer. New England Journal of Medicine. 2019; 381:121-131
DOI: 10.1056/NEJMoa1903835. - Armstrong A. et al. ARCHES: A Randomized, Phase III Study of Androgen Deprivation Therapy With Enzalutamide or Placebo in Men With Metastatic Hormone-Sensitive Prostate Cancer. Journal of Clinical Oncology. 2019 DOI: 10.1200/JCO.19.00799.
Further Related Content: Which Systemic Therapy for Which Patient with Newly Diagnosed Metastatic Prostate Cancer Presentation