- Newly diagnosed high-risk metastatic hormone-sensitive prostate cancer (mHSPC), with prednisone 5 mg daily.
- For metastatic castration-resistant prostate cancer (mCRPC) with prednisone 10 mg daily.
The half-life of prednisone is less than 16 hours, while the half-life of dexamethasone is much longer (36-54 hours). Dexamethasone has a higher ratio of glucocorticoid to mineralocorticoid activity than prednisone. It also has greater activity as a single agent in mCRPC disease compared to prednisone.4 Approximately 25% of patients progressing on abiraterone with prednisone have a PSA decline after they are switched to dexamethasone.5,6
In a recently published study, various regimens of prednisone in combination with abiraterone were compared, including one arm with dexamethasone.7 The primary endpoint was no mineralocorticoid excess (grade ≥1 hypokalemia or grade ≥2 hypertension) through 24 weeks (6 cycles) from treatment. The study design is shown in Figure 1. The results are shown in Figure 2, including the rates of demonstrated hypokalemia. Of the 164 randomized men to prednisone 5 mg, twice daily, once daily, or 2.5 mg twice daily, or dexamethasone, 0.5 mg, once daily, 24/34 patients (70.6%, 95% CI, 53.8%-83.2%), 14/38 patients (36.8%, 95% CI, 23.4%-52.7%), 21/35 patients (60.0%, 95% CI, 43.6%-74.4%), and 26/37 patients (70.3%, 95% CI, 54.2%-82.5%), respectively, had no mineralocorticoid excess.
Interestingly, plasma adrenocorticotrophic hormone and urinary mineralocorticoid metabolites after 8 weeks of treatment were higher with prednisone, 2.5 mg, twice daily and 5 mg, once daily, than with 5 mg twice daily or dexamethasone, 0.5 mg, once daily. The level of urinary glucocorticoid metabolites appeared higher in patients who did not meet the primary endpoint, regardless of glucocorticoid regimen. It is important to note that the total lean body mass decreased in the prednisone groups and total body fat increased in the prednisone, 5 mg, twice daily and dexamethasone groups. In the dexamethasone group, there was an increase in serum insulin and insulin resistance, while total bone mineral density decreased.
The authors concluded that abiraterone acetate with prednisone, 5 mg, twice daily, or dexamethasone, 0.5 mg, once daily, met the prespecified threshold for the primary endpoint (95% CI excluded 50% mineralocorticoid excess). In contrast, abiraterone acetate with prednisone, 5 mg, once daily, or 2.5 mg, twice daily, did not meet the threshold. Abiraterone acetate in combination with dexamethasone appeared to be especially active but may be associated with adverse metabolic consequences.
Figure 1 – Study design comparing various regimens of prednisone in combination with abiraterone:
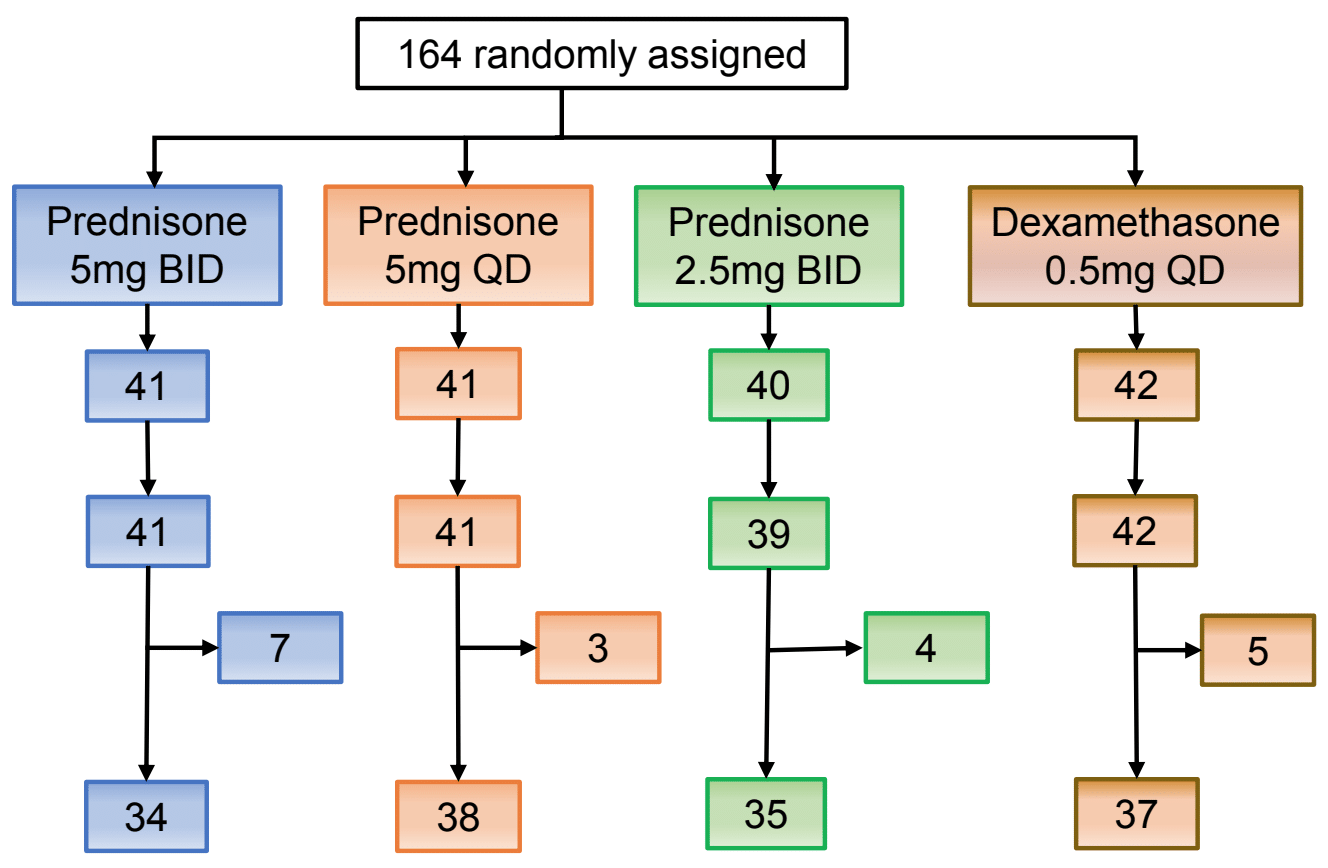
Figure 2 – Final results of the study:

Dr. Attard concluded his talk stating that prednisone 5 mg BID and dexamethasone 0.5 mg once a day can minimize mineralocorticoid excess. However, this came at the cost of increased body fat for prednisone, and an increase in serum insulin and insulin resistance for dexamethasone. Prednisone 5 mg once daily minimizes the long-term physiological side effects but with a greater risk of mineralocorticoid excess. Dr. Attard emphasized that lower steroid doses require careful monitoring and ensuring that patients are medically optimized prior to beginning abiraterone.
Presented by: Gerhardt Attard, MD, PhD, FRCP, John Black Charitable Foundation Endowed Chair in Urological Cancer Research, University College London Cancer Institute, London, UK
Written by: Hanan Goldberg, MD, Urology Department, SUNY Upstate Medical University, Syracuse, New York, USA, Twitter: @GoldbergHanan, at the 2019 Advanced Prostate Cancer Consensus Conference (APCCC) #APCCC19, Aug 29 - 31, 2019 in Basel, Switzerland
References:
- Fizazi K1, Tran N1, Fein L1, Matsubara N1, Rodriguez-Antolin A1, Alekseev BY1, Özgüroğlu M1, Ye D1, Feyerabend S1, Protheroe A1, De Porre P1, Kheoh T1, Park YC1, Todd MB1, Chi KN1; LATITUDE Investigators. Abiraterone plus Prednisone in Metastatic, Castration-Sensitive Prostate Cancer. N Engl J Med. 2017 Jul 27;377(4):352-360. doi: 10.1056/NEJMoa1704174. Epub 2017 Jun 4.
- Ryan CJ1, Smith MR, de Bono JS, Molina A, Logothetis CJ, de Souza P, Fizazi K, Mainwaring P, Piulats JM, Ng S, Carles J, Mulders PF, Basch E, Small EJ, Saad F, Schrijvers D, Van Poppel H, Mukherjee SD, Suttmann H, Gerritsen WR, Flaig TW, George DJ, Yu EY, Efstathiou E, Pantuck A, Winquist E, Higano CS, Taplin ME, Park Y, Kheoh T, Griffin T, Scher HI, Rathkopf DE; COU-AA-302 Investigators. Abiraterone in metastatic prostate cancer without previous chemotherapy. N Engl J Med. 2013 Jan 10;368(2):138-48. doi: 10.1056/NEJMoa1209096. Epub 2012 Dec 10.
- de Bono JS1, Logothetis CJ, Molina A, Fizazi K, North S, Chu L, Chi KN, Jones RJ, Goodman OB Jr, Saad F, Staffurth JN, Mainwaring P, Harland S, Flaig TW, Hutson TE, Cheng T, Patterson H, Hainsworth JD, Ryan CJ, Sternberg CN, Ellard SL, Fléchon A, Saleh M, Scholz M, Efstathiou E, Zivi A, Bianchini D, Loriot Y, Chieffo N, Kheoh T, Haqq CM, Scher HI; COU-AA-301 Investigators. Abiraterone and increased survival in metastatic prostate cancer. N Engl J Med. 2011 May 26;364(21):1995-2005. doi: 10.1056/NEJMoa1014618.
- Venkitaraman R1, Lorente D2, Murthy V3, Thomas K4, Parker L2, Ahiabor R2, Dearnaley D2, Huddart R2, De Bono J2, Parker C5. A randomised phase 2 trial of dexamethasone versus prednisolone in castration-resistant prostate cancer. Eur Urol. 2015 Apr;67(4):673-9. doi: 10.1016/j.eururo.2014.10.004. Epub 2014 Oct 16.
- Romero-Laorden N1,2, Lozano R1,3,4, Jayaram A5,6, López-Campos F1,7, Saez MI4,8, Montesa A4,8, Gutierrez-Pecharoman A2,9, Villatoro R4,10, Herrera B4,11, Correa R4,12, Rosero A1,13, Pacheco MI1,4, Garcés T1,4, Cendón Y1,14, Nombela MP1, Van de Poll F1, Grau G1,4, Rivera L1,4, López PP1, Cruz JJ3, Lorente D15, Attard G5,6, Castro E16,17, Olmos D1,4,8. Phase II pilot study of the prednisone to dexamethasone switch in metastatic castration-resistant prostate cancer (mCRPC) patients with limited progression on abiraterone plus prednisone (SWITCH study). Br J Cancer. 2018 Oct;119(9):1052-1059. doi: 10.1038/s41416-018-0123-9. Epub 2018 Aug 21.
- Lorente D1, Omlin A2, Ferraldeschi R1, Pezaro C1, Perez R1, Mateo J1, Altavilla A1, Zafeirou Z1, Tunariu N1, Parker C3, Dearnaley D3, Gillessen S4, de Bono J1, Attard G1. Tumour responses following a steroid switch from prednisone to dexamethasone in castration-resistant prostate cancer patients progressing on abiraterone. Br J Cancer. 2014 Dec 9;111(12):2248-53. doi: 10.1038/bjc.2014.531. Epub 2014 Oct 14
- Gerhardt Attard, MD, PhD,corresponding author1 Axel S Merseburger, MD,2 Wiebke Arlt, MD, DSc,3 Cora N Sternberg, MD,4 Susan Feyerabend, MD,5 Alfredo Berruti, MD,6 Steven Joniau, MD, PhD,7 Lajos Géczi, MD,8 Florence Lefresne, MD,9 Marjolein Lahaye, MSc,9 Florence Nave Shelby, PhD,9 Geneviève Pissart, MSc,9 Sue Chua, MBBS,10 Robert J Jones, MBChB, PhD,11 and Bertrand Tombal, MD, PhD12 Assessment of the Safety of Glucocorticoid Regimens in Combination With Abiraterone Acetate for Metastatic Castration-Resistant Prostate Cancer A Randomized, Open-label Phase 2 Study. JAMA Oncol. 2019 Aug; 5(8): 1159–1167.
Further Related Content: Optimal Glucocorticoid Regimen with Abiraterone Acetate Presentation