(UroToday.com) The ANZUP annual scientific meeting’s clinical trials session included an update in renal cell carcinoma (RCC) provided by Dr. David Pook and Dr. Craig Gedye. Dr. Pook started by highlighting that non-clear cell RCC account for ~25% of RCC cases with less clear treatment guidelines compared to clear cell RCC. The UNISON trial is evaluating nivolumab followed by ipilimumab + nivolumab in advanced non-clear cell RCC (ANZUP 1602). The hypothesis of this trial is that patients are treated with nivolumab monotherapy upfront and that those who are nivolumab refractory may benefit from nivolumab + ipilimumab combination therapy.
The trial is aiming to accrue 86 participants, powered to distinguish an objective response rate of 15% versus 30% in participants treated with nivolumab + ipilimumab in part 2 of the trial.
The KeyPAD trial is a phase II trial of denosumab and pembrolizumab in patients with clear cell RCC (ANZUP 1601). The aim is to determine the activity and safety of combining the RANKL inhibitor denosumab with the anti-PD1 inhibitor pembrolizumab in advanced clear cell RCC:

Thus far, 54 of 70 patients have been recruited, with an aim to complete enrollment in mid-2022.
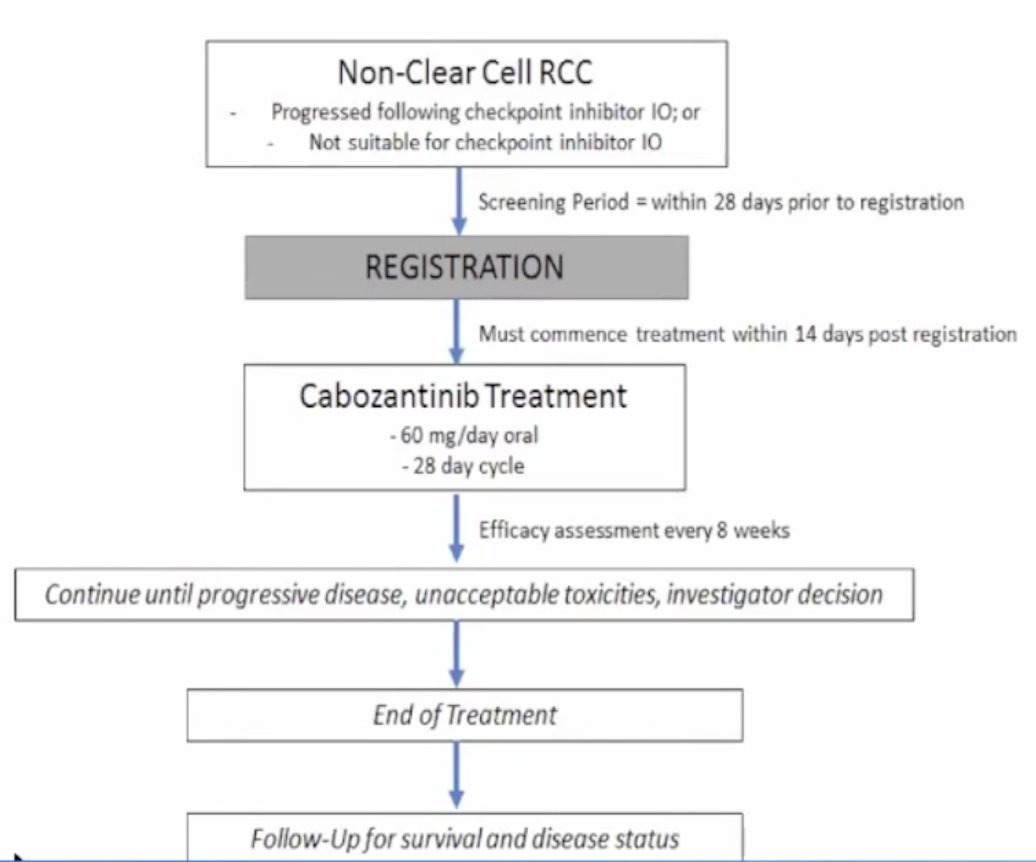
The third trial discussed by Dr. Pook was the UNICAB trial evaluating non-clear cell RCC post immunotherapy patients treated with cabozantinib. The aim of this trial is to determine the activity and safety of cabozantinib in participants with metastatic or locally advanced/unresectable non clear cell RCC who have progressed on or are unsuitable for treatment with immunotherapy. To date, 24 of 48 patients have been recruited, with an aim to complete recruitment by mid-2022. The trial design for UNICAB is as follows:
The RAMPART trial is the Renal Adjuvant Multiple Arm Randomized Trial with three groups of patients including: Group A - active monitoring for 1 year, Group B – durvalumab every 4 weeks for 1 year, and Group C – durvalumab every 4 weeks for 1 year and tremelimumab at day 1 and week 4:

This trial will include 1,750 participants (200 from Australia) with intermediate/high-risk RCC (all histology) randomized 3:2:2 with a primary outcome of disease-free survival and overall survival, and secondary outcomes of metastasis-free survival and disease-specific survival.
Dr. Gedye notes that according to Canadian goals for research priorities for kidney cancer, the following three proposals were amongst the top priority: (i) development and evaluation of new effective treatment for patients with advanced kidney cancer of the non-clear-cell variety/subtype, (ii) identification and validation of biomarkers that may be used to predict the response to a treatment for kidney cancer, and (iii) identification and validation of biomarkers that may be used for the detection of kidney cancer. British research priorities for patients with RCC are as follows:
- Selecting the right targeted therapies and immunotherapies, combination of therapies and optimal therapeutic sequence for individual patients to maximize the quality of life and minimize side effects
- Management for patient groups that are difficult to treat, and in particular non-clear cell RCC subtypes
- Maximize quality of life in all domains
- Early detection and screening for RCC
- Personalized treatment to minimize side effects of therapy, increase effectiveness and maximize quality of life
- Optimizing and personalizing follow up after treatment for RCC
- Improved prognostic tools
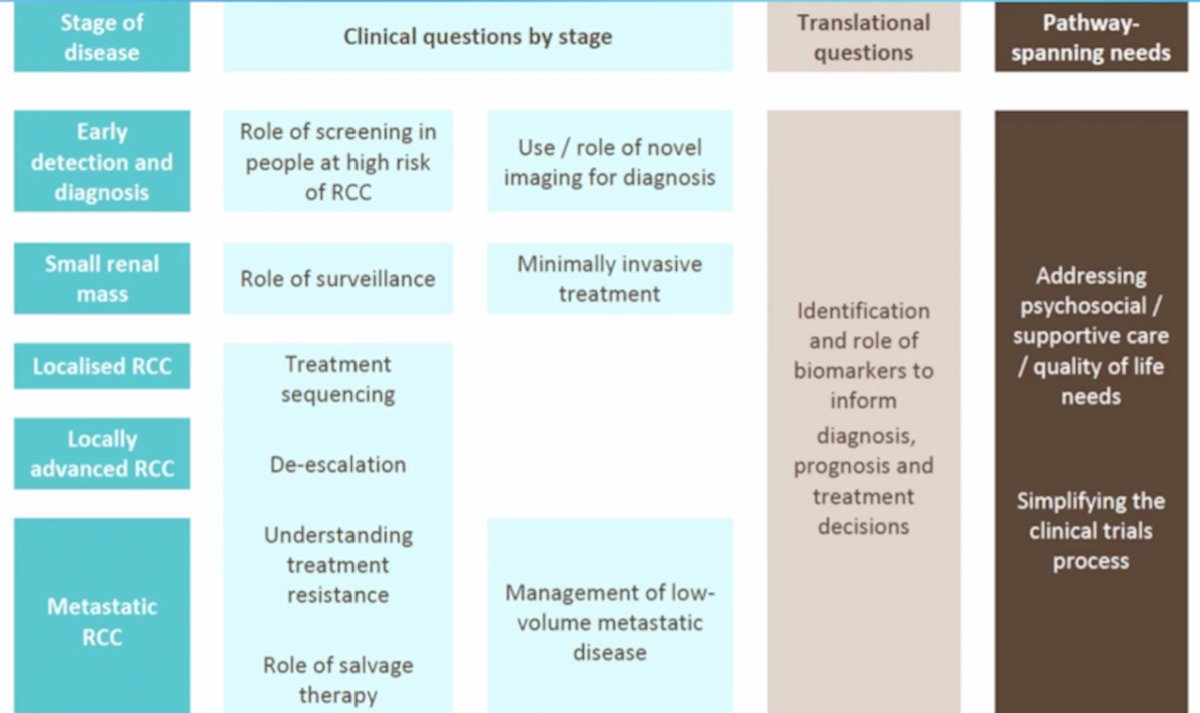
The following are clinical questions by stage, translational questions, and pathway-spanning needs as highlighted by Dr. Gedye:
Ideas and next steps for research in RCC are as follows:
- Functional imaging and theranostics
- De-escalation of systemic therapy
- Management of small renal masses
- Management of oligometastases
- Unmet supportive care needs
Dr. Gedye emphasizes that for patients with metastatic RCC, perhaps there is a role for an initial period of active surveillance as highlighted in the following figure:

However, there are several outstanding questions to this approach, which Dr. Gedye used to conclude this presentation:
- Who is eligible for active surveillance?
- Can we predict who needs immediate treatment and who can wait?
- What predicts success of active surveillance?
- Clinical features beyond IMDC criteria? Lymphocyte-neutrophil ratio? Late relapse? Low grade disease? Sites of metastasis?
- When do we stop active surveillance and offer treatment?
- Grow velocity? New lesions? How long can patients stay on active surveillance?
- Can we extend the duration of active surveillance?
- What are the psychological needs of active surveillance?
- What is the best clinical practice for active surveillance?
- What is the follow-up schedule? Imaging schedule? Which scans should we use?
Presented by: Craig Gedye, BSc(Hons) MBChB FRACP PhD, Medical Oncology, Calvary Mater Newcastle, Hunter Medical Research Institute New Lambton Heights, New South Wales, Australia and David Pook, BMedSci (Hons) MBBS FRACP MD, Medical Oncology, Monash University, Melbourne, Australia
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, @zklaassen_md on Twitter during the 2021 Australian and New Zealand Urogenital and Prostate (ANZUP) Cancer Trials Group Annual Scientific Meeting (ASM), Sunday, Oct 17 – Monday, Oct 18, 2021.