(UroToday.com) The 2026 PSMA and Beyond conference featured an approaches to combination therapies session and presentation by Dr. Lawrence Fong discussing immunotherapy with checkpoint inhibitors and beyond. Dr. Fong started with an old quote “Prostate cancer is a cold tumor. Immunotherapy will never work…” Until recently, this has for the most part been true. Dr. Fong noted that there have been many negative trials, including two phase 3 trials of ipilimumab (anti-CTLA-4), three phase 3 trials with pembrolizumab (anti-PD-1), one phase 3 trial of nivolumab (anti-PD-1), and two phase 3 trials of atezolizumab (anti-PD-L1). This is due in part because there are immunosuppressive myeloid cells in tumors. Dr. Fong’s work at the University of Washington has focused on single-cell assessment of prostate cancer, with a specific interest in myeloid cells1:
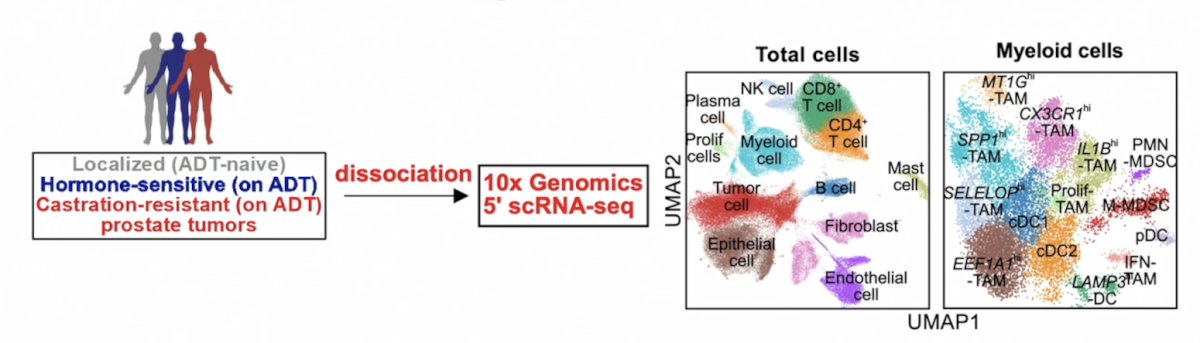
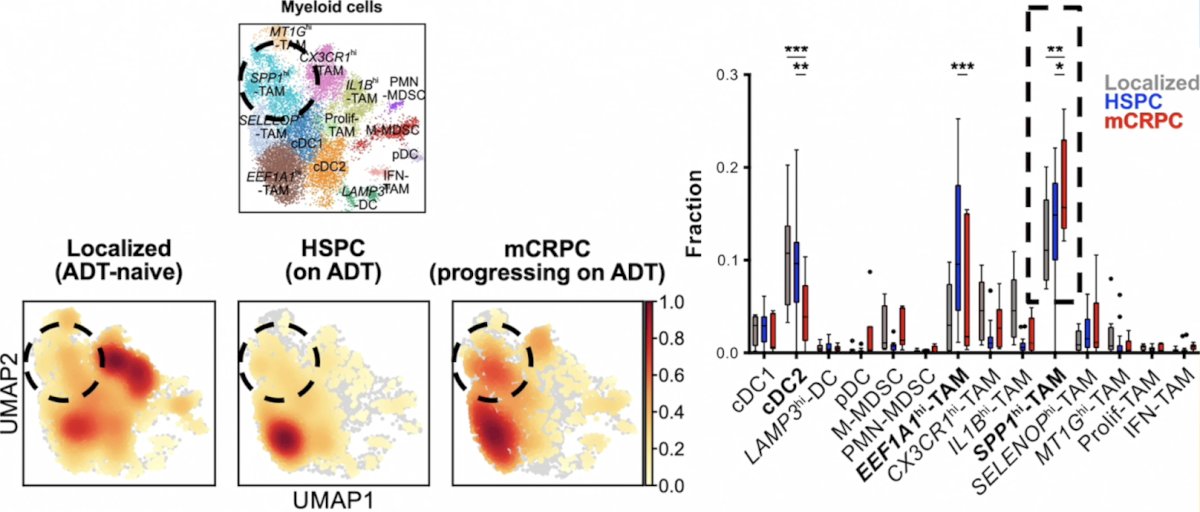
In Dr. Fong’s lab, they used single-cell profiling on patient biopsies across the disease continuum and found that a distinct population of tumor-associated macrophages with elevated levels of SPP1 transcripts (SPP1hi-TAMs) become enriched with the progression of prostate cancer to mCRPC:
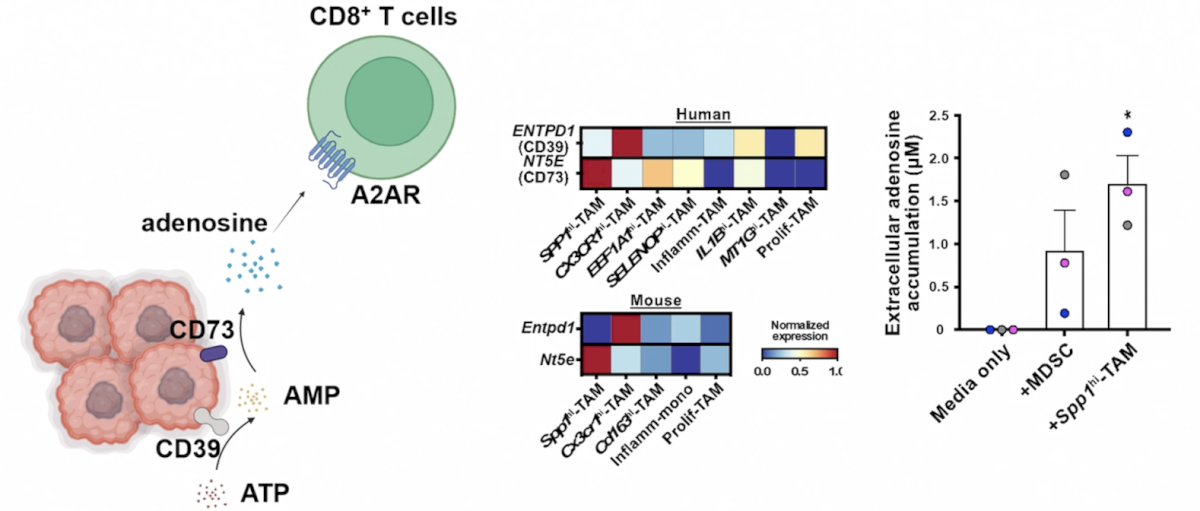
Pathway analysis also identified adenosine signaling as a potential mechanism for SPP1hi-TAM-mediated immunotherapeutic resistance:
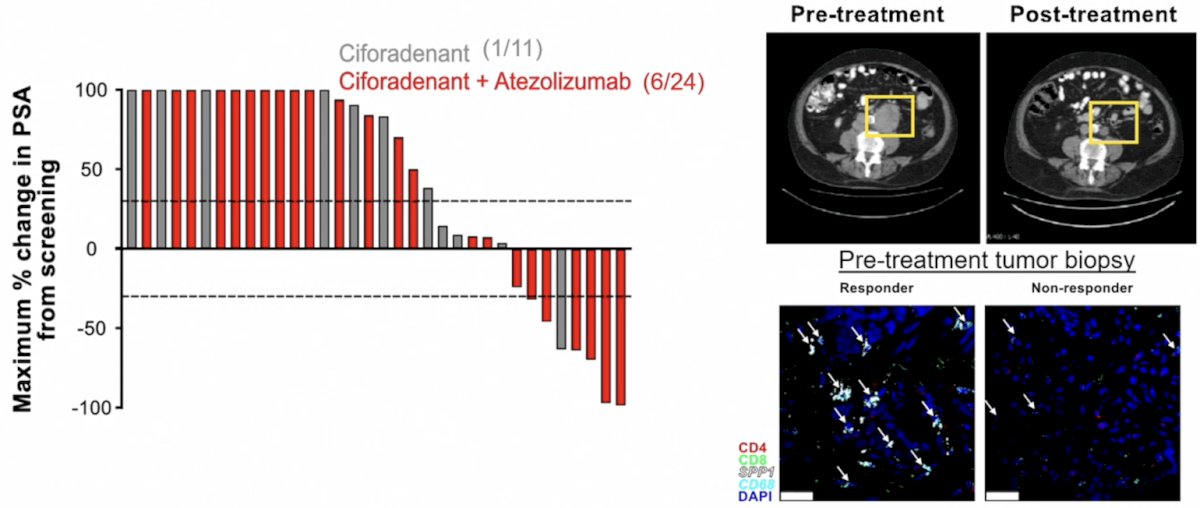
Consistent with preclinical results, inhibition of adenosine A2A receptors using ciforadenant in combination with atezolizumab induces clinical responses in patients with mCRPC. Moreover, inhibiting adenosine A2A receptors results in a significant decrease in SPP1hi-TAM abundance in CRPC, indicating that this pathway is involved in both induction and downstream immunosuppression:
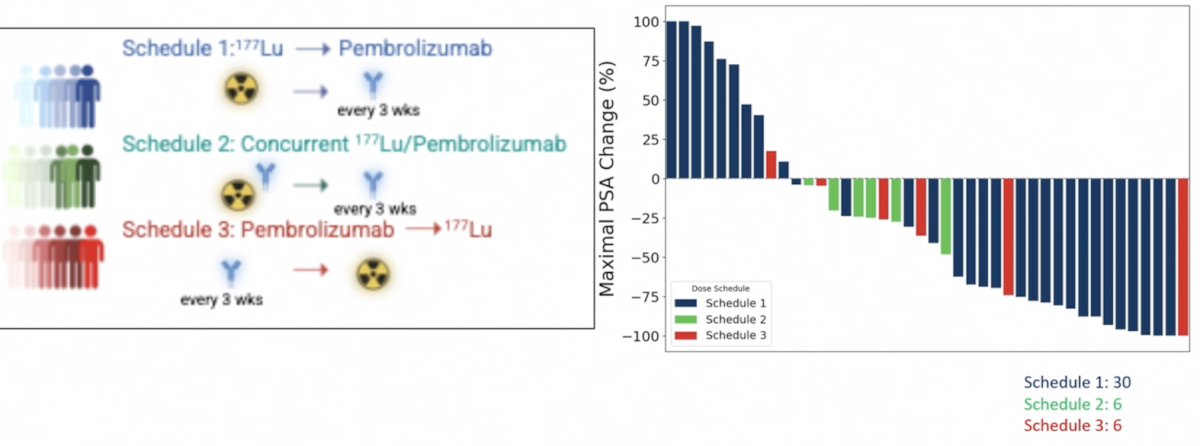
In 2023, Dr. Fong and colleagues2 published results of a phase 1 dose expansion trial assessing a single dose of 177Lu-PSMA617 followed by maintenance pembrolizumab in mCRPC patients. They found that 14 of 25 patients (56%, 95% CI 35-76) had an objective response rate, with 5% of patients having a grade 3+ treatment related adverse event:
For the remainder of his presentation, Dr. Fong highlighted that immunotherapy can work in prostate cancer. This includes multiple T-cell engagers that are showing clinical activity:
- STEAP-1 x CD3 (xaluritamig)
- KLK2 x CD3 (pasritamig)
- PSMA x CD3 (VIR-5500)
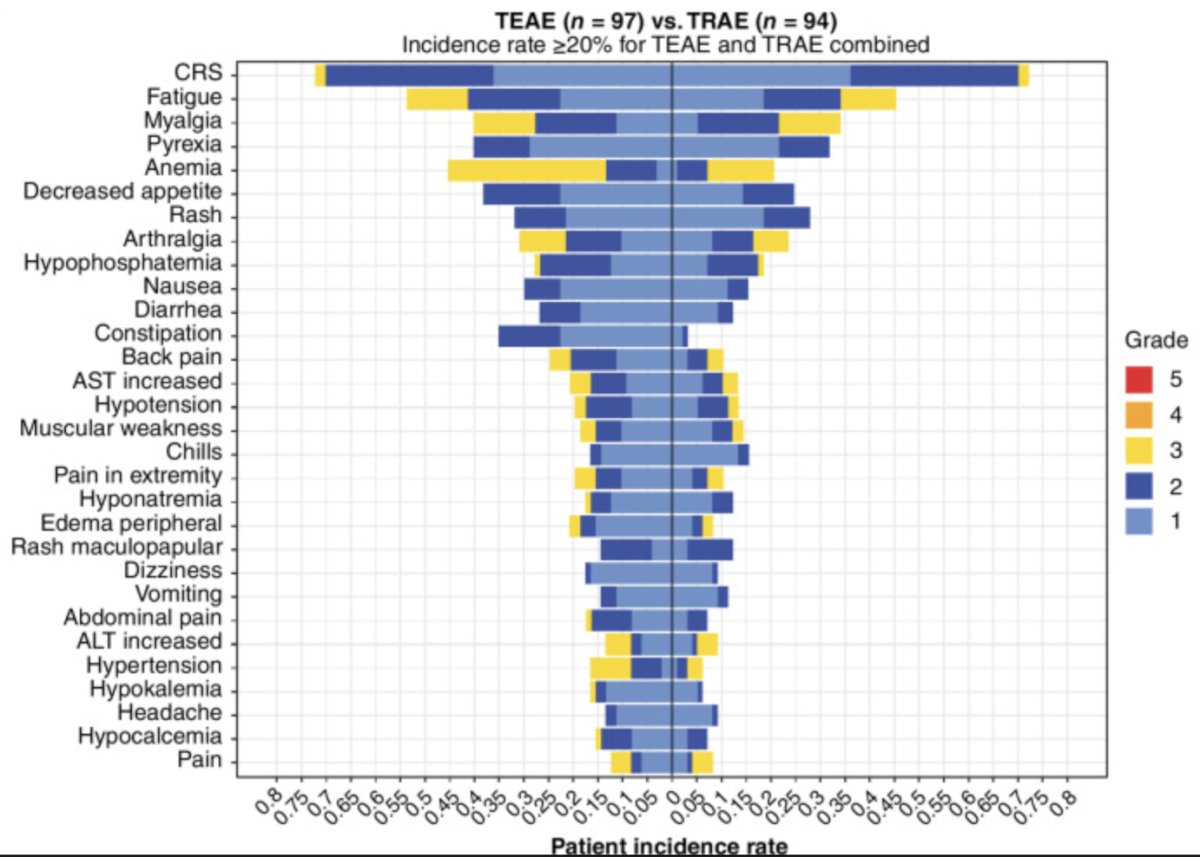
In 2024, Kelly et al.3 reported the first in human study of xaluritamig monotherapy dose exploration for patients with mCRPC, primarily taxane pretreated patients. There were 97 patients that received ≥1 IV dose ranging from 0.001 to 2.0 mg weekly or every 2 weeks. The maximal tolerated dose was identified as 1.5 mg IV weekly via a 3-step dose. The most common treatment-related adverse events were cytokine release syndrome (72%), fatigue (45%), and myalgia (34%). Cytokine release syndrome occurred primarily during cycle 1 and improved with premedication and step dosing:
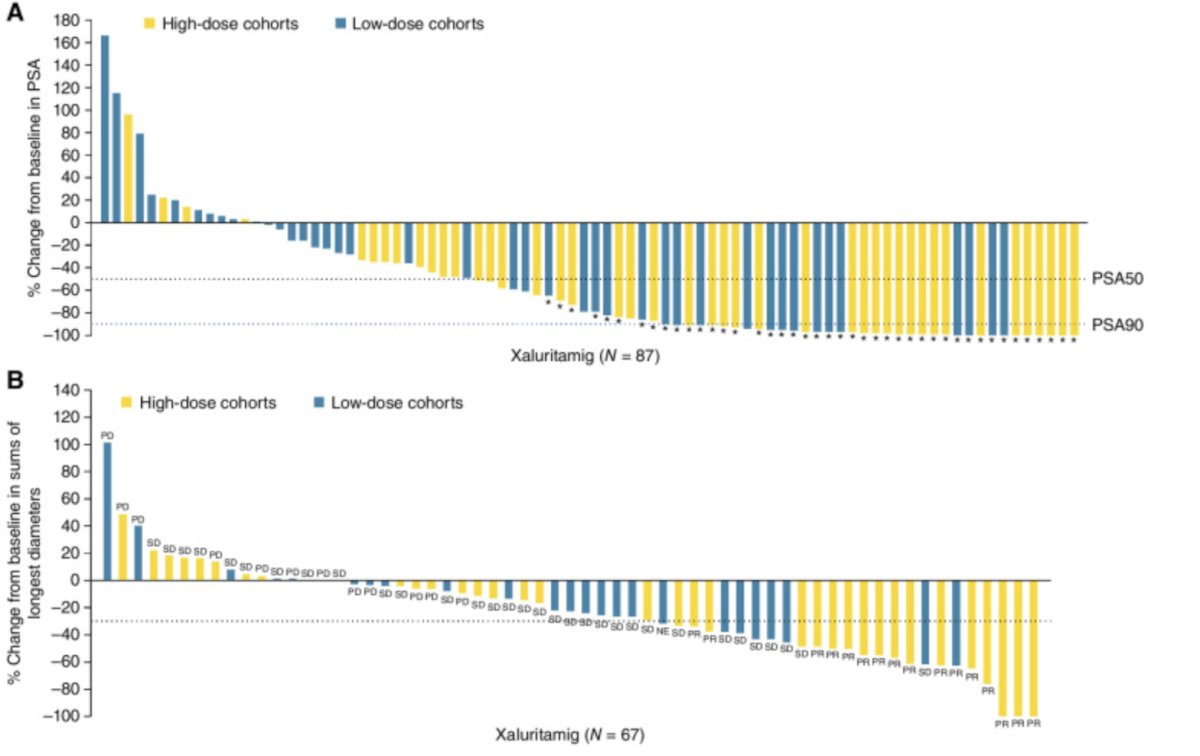
PSA and RECIST responses across cohorts were encouraging, with a 49% PSA50, 24% objective response rate, and with greater frequency at target doses ≥0.75 mg (59% PSA50, 41% objective response rate). The following represents the best PSA percentage change from baseline and the best percentage change in tumor size:
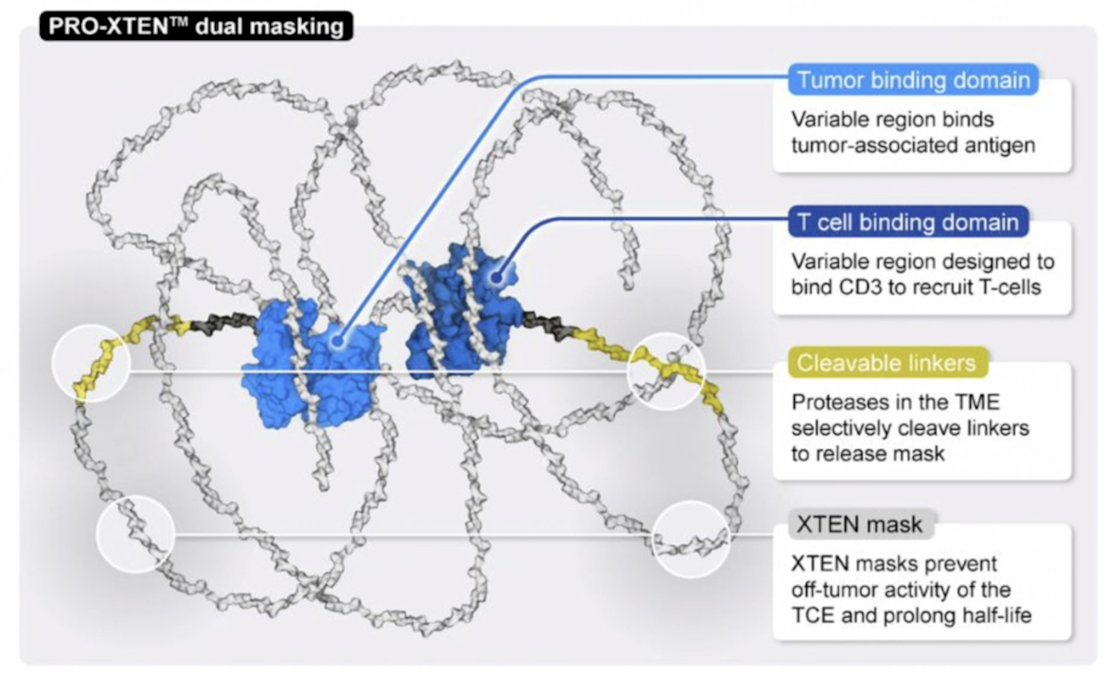
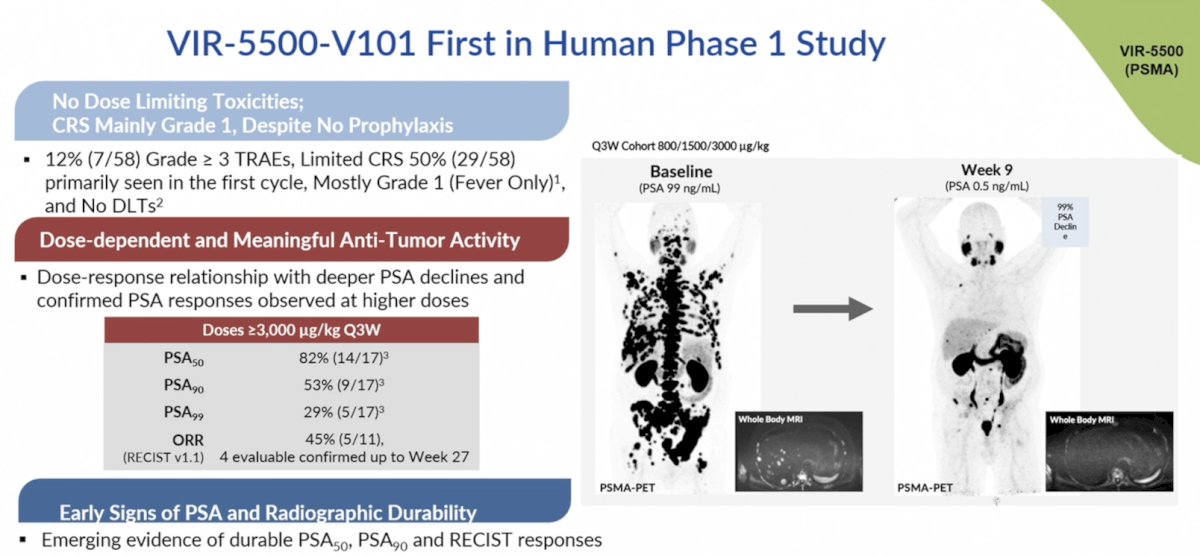
At ASCO GU 2026, Dr. de Bono presented the preliminary phase 1 dose escalation results of VIR-5500, a dual-masked PRO-XTEN T-cell engager for patients with mCRPC. PRO-XTEN masks T-cell engagers and has the best in class therapeutic index and long-term durability in oncology. This is secondary to (i) maximizing the tumor environment, (ii) less toxicity, (iii) longer half life and every 3 week dosing, (iv) clinically validated masking, and (v) providing a universal masking platform:
In this phase 1 study, VIR-5500 was administered IV weekly (QW) and every 3 weeks (Q3W) at doses of 30 - 4000 ug/kg to eligible participants with progressive mCRPC after receiving standard of care. As of January 9, 2026, 58 heavily pretreated mCRPC participants (94.8% post-taxane; median 4 prior lines of therapy) received ≥ 1 dose of VIR-5500. There were no dose limiting toxicities (pre-defined toxicities occurring during cycle 1) reported. The incidence of related grade ≥ 3 adverse events was 12% and cytokine release syndrome was mostly limited to grade 1 and 2. PSA declines were noted in all participants dosed at ≥ 3000 ug/kg Q3W, including clinically significant and deep PSA reductions (82% PSA50 and 53% PSA90). Preliminary evidence of durable PSA responses lasting over one year was noted in select patients undergoing intra-patient dose escalation. An objective response rate of 45% was observed in 5 out of 11 RECIST-evaluable patients treated at doses ≥ 3000 µg/kg Q3W:
Dr. Fong concluded his presentation discussing immunotherapy with checkpoint inhibitors and beyond with the following take-home points:
- Immune checkpoint inhibitors by themselves have limited efficacy in prostate cancer
- Immunosuppressive myeloid cells (SPP1hi-TAMs) restrict the activity of immune checkpoint inhibitors
- Targeting myeloid-mediated mechanisms of resistance can sensitize some patients to this approach
- T cell engagers have significant clinical efficacy in prostate cancer
- By targeting the mechanism of therapeutic resistance, we may realize the full potential of immunotherapy in prostate cancer
Presented by: Lawrence Fong, MD, University of Washington, Fred Hutchinson Cancer Center, Seattle, WA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 PSMA & Beyond Conference, Los Angeles, CA, Thurs, Mar 26 – Fri, Mar 27, 2026.
Related content: Immunotherapy Beyond Checkpoint Inhibitors "Presentation" - Lawrence Fong
References:
- Lyu A, Fan Z, Clark M, et al. Evolution of myeloid-mediated immunotherapy resistance in prostate cancer. Nature. 2025 Jan;637(8048):1207-1217.
- Aggarwal R, Starzinski S, de Kouchkovsky I, et al. Single-dose 177Lu-PSMA617 followed by maintenance pembrolizumab in patients with metastatic castration-resistant prostate cancer: An open-label, dose-expansion, phase 1 trial. Lancet Oncol. 2023 Nov;24(11):1266-1276.
- Kelly WK, Danila DC, Lin CC, et al. Xaluritamig, a STEAP1 x CD3 XmAb 2+1 Immune Therapy for Metastatic Castration-Resistant Prostate Cancer: Results from Dose Exploration in a First-in-Human Study. Cancer Discov. 2024 Jan 12;14(1):76-89.