(UroToday.com) The 2025 PSMA and Beyond annual meeting featured a LuPSMA therapy session and a presentation by Dr. Matthew Rettig discussing real world experience in the US and how PSMA radioligand therapy is being used post VISION.1 Dr. Rettig started his presentation by highlighting the FDA-approved agents for mCRPC:
- Hormonal (androgen receptor pathway blockers): abiraterone and enzalutamide
- Cytotoxic: docetaxel and cabazitaxel
- Immunotherapeutic: sipuleucel-T
- DNA damage: radium-223 (radiopharmaceutical)
- Biomarker directed: pembrolizumab, olaparib, rucaparib, Lu177-vipivotide tetraxetan (PSMA targeting)
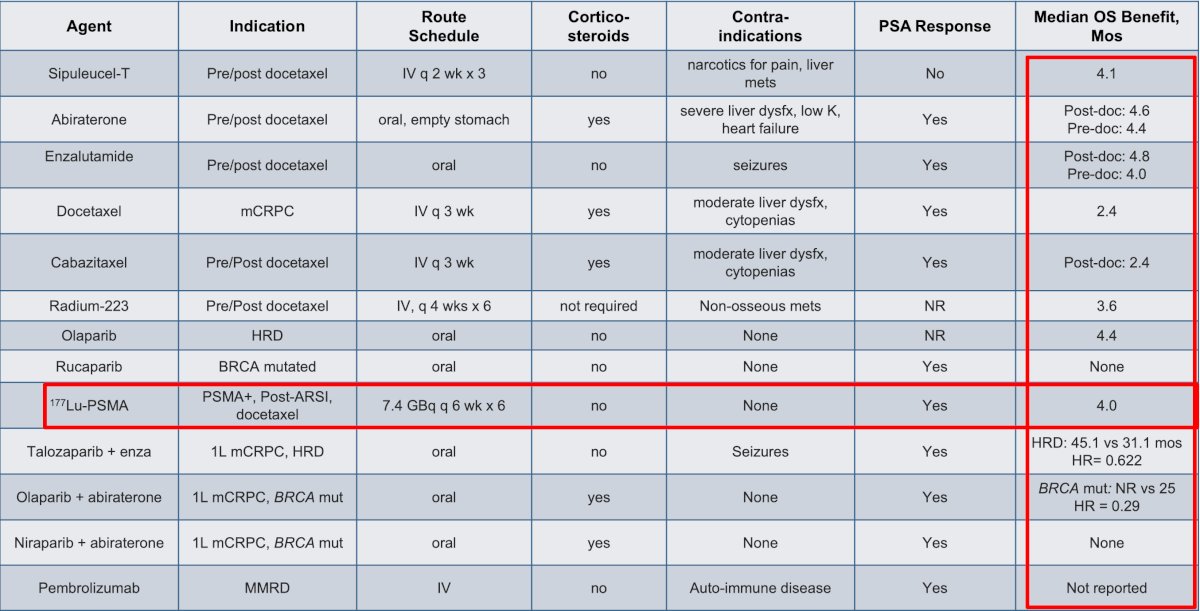
The following table demonstrates the mCRPC overall survival benefit of FDA approved treatments:
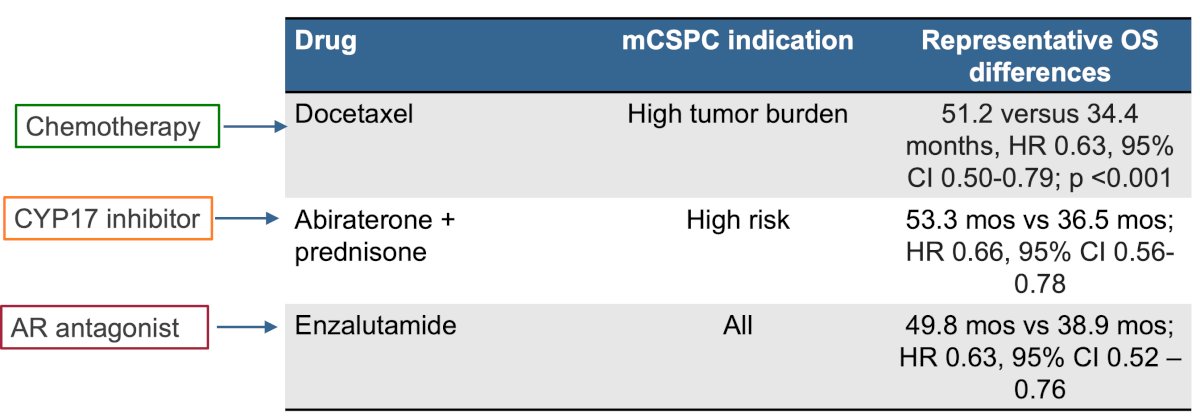
What’s notable is that drugs approved for mCRPC have a greater impact on absolute overall survival when used for metastatic castration sensitive prostate cancer. This includes chemotherapy, abiraterone + pembrolizumab, and enzalutamide:
Dr. Rettig notes that the US Veterans Affairs medical system is the largest integrated healthcare system in the United States. Approximately 9 million veterans are enrolled, with a median age of 57 years compared to a median 38 years for the US population as a whole. Moreover, there are 40,000 new cancer cases/year in the VA with a median age of 66 years (which is the same for the US population as a whole), with 1/3 of all new cancer cases being prostate cancer. The VA has a unified electronic medical record, which captures the 1.2 million Veterans with prostate cancer diagnosed since 2000. Clinical and pathologic data are readily accessible for analysis through the VINCI platform. Dr. Rettig and his group have assessed the utilization of 177Lu-PSMA-617 in the VA system, results of which are forthcoming and will be presented at the upcoming ASCO 2025 annual meeting.
There are several real world studies correlating genomics with outcomes. Presented at ASCO 2024, Gauntner et al. investigated the association of genomic variants with clinical outcomes in men with mCRPC treated with 177Lu-PSMA-617. Specifically, the impact of genomic variants on PSA50 response was evaluated. Among 153 patients treated with 177Lu-PSMA-617, 120 underwent genomic sequencing. Patients with amplification of cell cycle genes (n = 8) had poorer overall survival of 5.1 months versus 13.4 months for those without amplification (HR 4.26, 95% CI 1.79-10.11), and shorter progression free survival of 4.3 versus 7.4 months (HR 2.40, 95% CI 1.10-5.22). Patients with loss or mutation of HRR genes (n = 32) had an overall survival of 13.7 months versus 12.2 months for those with no HRR alterations, but this was not significant (HR 0.57, 95% CI 0.29-1.12).
A second study from Raychaudhuri et al.2 evaluated associations between mCRPC mutational profile with 177Lu-PSMA-617 clinical outcomes. There were 126 patients with next generation sequencing results who received at least 1 cycle of 177Lu-PSMA-617, including 58 (46%) patients with a DNA damage repair gene mutation (DNA damage response group) and 59 (46.8%) with a mutation in TP53, RB1, or PTEN tumor suppressor genes (TSG group). The presence of ≥1 TSG mutation was associated with shorter PSA progression free survival (HR 1.93, 95% CI 1.05 to 3.54) and overall survival (HR 2.65, 95% CI 1.15 to 6.11). There was also improved overall survival favoring the DNA damage response group (HR 0.37, 95% CI 0.14 to 0.97) on multivariable analysis.
Finally, Wenzel and colleagues3 assessed individual response to 177Lu-PSMA-617 regarding the genomic profile of patients with mCRPC. Of 194 patients with mCRPC, 22% were BRCA1/2 versus 14% PTEN/TP53/RB1 versus 63% without one of these mutations. Among 87 patients with 177Lu-PSMA-617 for mCRPC, significant differences in progression free survival and overall survival were observed (both p ≤ 0.02).
Dr. Rettig concluded his presentation discussing real world experience in the US and how PSMA radioligand therapy is being used post VISION with the following take home points:
- Usage of 177Lu-PSMA-617 radioligand therapy is increasing with time
- Genomic factors may be prognostic, although results vary
- We need better genomic predictive biomarkers that should be incorporated into prospective clinical trials when feasible
- We need novel approaches to improve overall survival in of mCRPC. Combinations that may have a synergistic effect (ie. PARP inhibitors + androgen receptor pathway inhibitors) should be pursued
- Bringing therapies from the mCRPC to the mHSPC space generally results in greater absolute benefit on overall survival
Presented by: Matthew Rettig, MD, University of California, Los Angeles, Los Angeles, CA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 PSMA and Beyond Annual Meeting, Los Angeles, CA, Fri, Mar 28 – Sat, Mar 29, 2025.
References:
- Sartor O, de Bono J, Chi KN et al. Lutetium-177-PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. N Engl J Med. 2021 Sep 16;385(12):1091-1103.
- Raychaudhuri R, Mo G, Tuchayi AM, et al. Genomic correlates of prostate-specific membrane antigen expression and response to 177Lu-PSMA-617: A retrospective multicenter cohort study. JCO Precis Oncol. 2024 Apr:8:e2300634.
- Wenzel M, Koll F, Hoeh B, et al. Cancer-control outcomes of patients with metastatic castration-resistant prostate cancer with BRCA gene or tumor suppressor mutations undergoing 177-Lutetium Prostate-Specific Membrane Antigen Radioligand Therapy. JCO Precis Oncol. 2024 Dec:8:e2400645.