(UroToday.com) In this plenary session, Dr. Amy Krambeck, Dr. Thomas Tailly, and Dr. Daron Smith discussed whether there is utility in “chasing” residual fragments post-percutaneous nephrolithotomy (PCNL). Of note, Dr. Krambeck was arguing for removing all stone fragments to achieve stone free status in contrast to Dr. Tailly who was in favor of not “chasing” stone fragments.
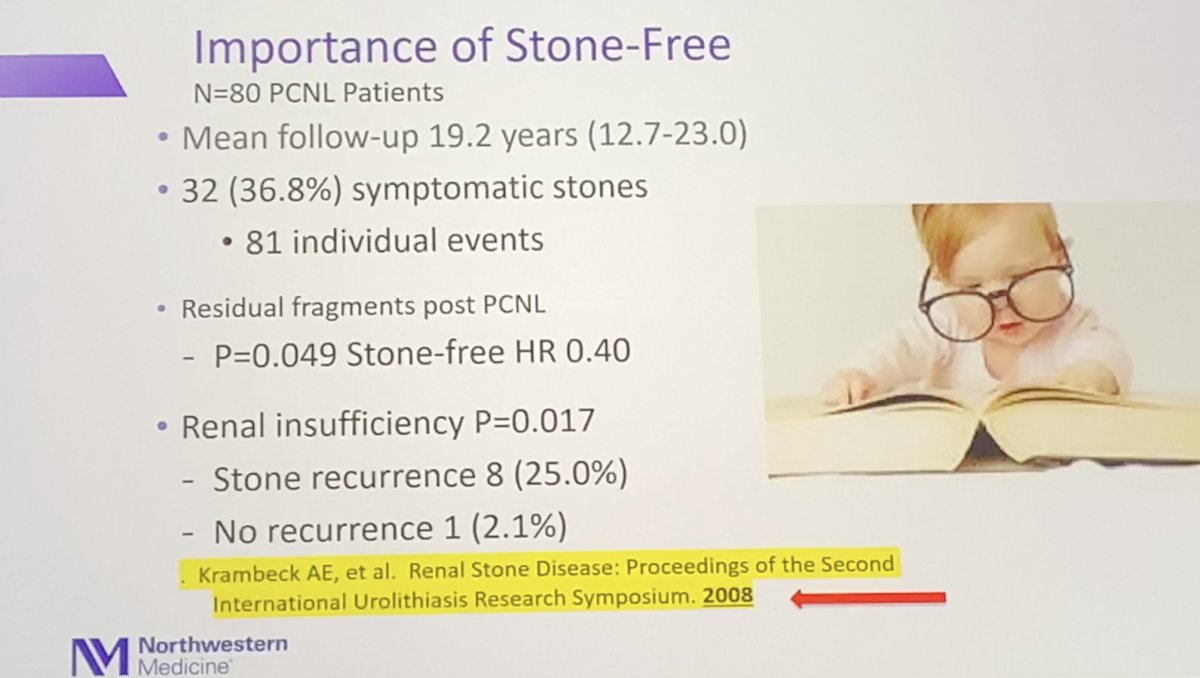
To start the discussion, Dr. Krambeck begins to emphasize the importance of achieving stone free status in all patients undergoing PCNL. From a study she conducted, a reported 32 patients (36.8%) out of 80 experience stone-related symptoms post-surgery with a mean follow-up of 19.2 years, of which 8 patients (25%) also developed renal insufficiency.1
A similar study by Raman et al with 728 PCNL patients demonstrated a cohort of 42 patients (8%) with residual stone, of whom 18 (43%) of them experienced stone-related symptoms. Eleven (61%) of these patients ended up requiring surgery. The median diameter of residual stone encountered in this study was 2 mm, indicating > 2 mm as a threshold for post-operative symptoms that may demand intervention.2 In another study by Altunrende et al, 430 patients who underwent PCNL were followed over a 3-year period. Defining < 4 mm stone residual fragments as “clinically insignificant fragments (CIRFs)”, 10 patients (26%) had reported symptoms post-surgery and 8 (21%) had an increase in their CIRFs.3
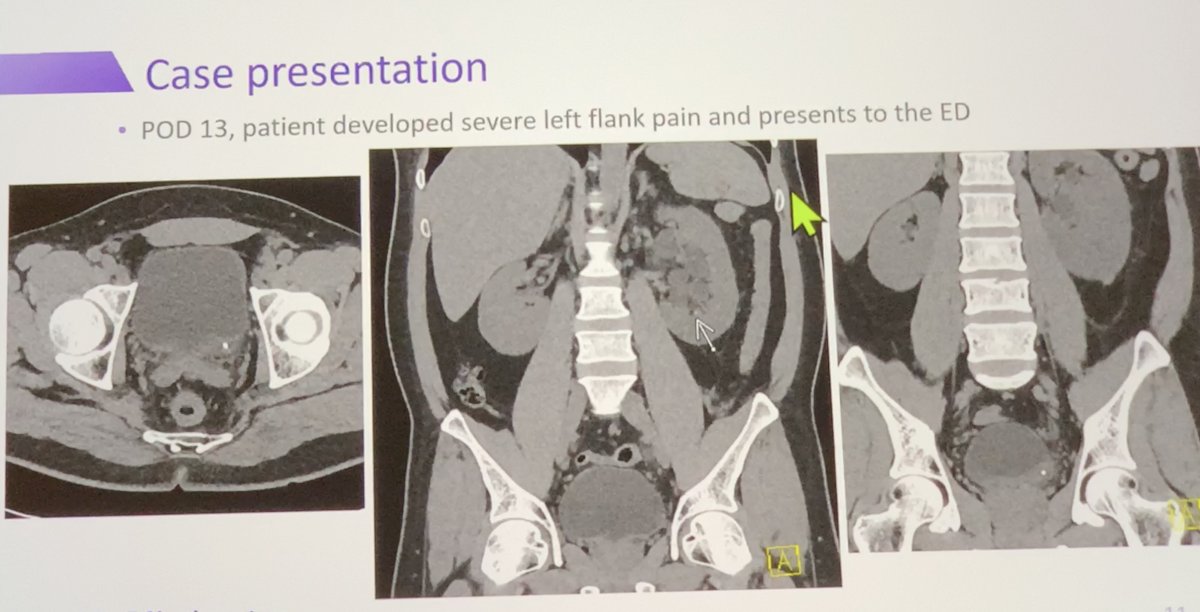
To further bolster her stance, Dr. Krambeck discussed a patient case of her own to highlight the importance of making patients truly stone free. Briefly, a 33-year-old patient with a large renal stone volume underwent PCNL. Post-operative CT identified three 1-2 mm small residual stone fragments with 1 week of surgery. After being discharged, patient presented to the ED at approximately 2 weeks for severe flank pain that required Toradol and alpha-antagonists to help pass the stone.
It is important to note how the presence of larger residual fragments is a strong determinant for early stone disease recurrence. A study by Emmott et. al with 658 patients enrolled demonstrated that patients with residual fragments > 4 mm had earlier recurrence than those with residuals < 4 mm. 4 Lastly, the presence of residual fragments has been linked to post-operative systematic inflammatory response syndrome. A recent study of 729 PCNL patients demonstrated 94 patients (13%) who ultimately developed SIRS postoperatively.5 Moreover, residual fragments also have been shown to be an individual risk factor for recurrent urinary tract infections (p < 0.046).6 Treating residual calculi can result in reduced risk of UTIs, but also improve overall QOL in the form benefits such as reduced financial burden associated with stone treatment and reduced pain.
To kick off his discussion, Dr. Tailly begins his counterpoint with refocusing our argument through various questions which include:
- Any residual fragment = unsuccessful treatment?
- When and how can we identify residual fragments?
- What size of fragment is acceptable to leave?
- Are all stone/patients equal?
- Is stone free the most important outcome?
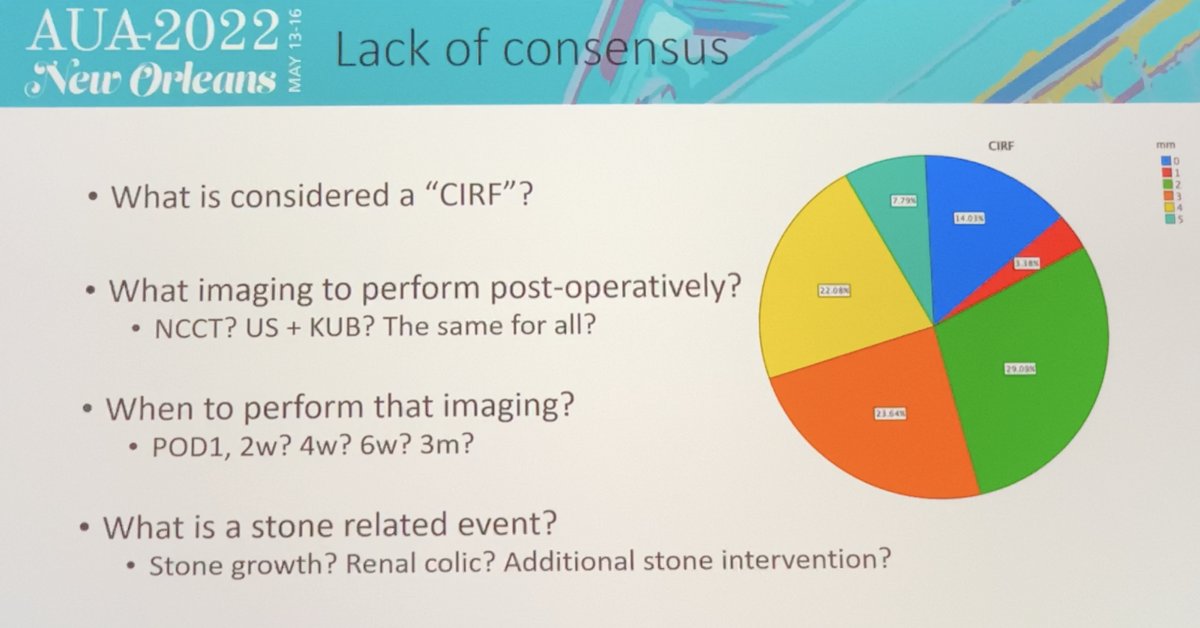
To better understand the controversy behind stone free status, Dr. Tailly wanted to remind the audience on the persistent incongruity in the definition of “stone free”. This definition can vary in regard to the size of stone (< 1 mm, < 2 mm, < 4 mm, etc), imaging modality used to identify fragments, and the width of imaging cuts (2 mm cuts, 4 mm cuts, etc). Without consensus, we cannot design strong prospective studies investigating residual fragments and their complications.
Even with significant heterogeneity amongst stone free definitions, a recent 2021 study highlights that there is no difference in disease progression amongst patients with residual fragments > 4 mm vs. those with < 4 mm.7 In terms of costs, “chasing” residual fragments are only cost-effective if fragments post-PCNL are > 4 mm (second look nephroscopy $2,475 vs. long-term management $4,674).
Lastly, Dr. Tailly mentions that quality of life in patients with residual fragments vs. no residual fragments is not significantly different. In fact, those that underwent a re-intervention fared worse in terms of quality of life compared to those with actively surveilled fragments.8

Concluding remarks:
Obtaining stone-free status for patients is an ongoing battle for our patients. It is further muddled by the inconsistency amongst the Urological community in terms of defining what “stone free” really means. Residual fragments can be a nidus of recurrent stone formation and painful symptoms which result in a large financial burden for patients. On the flip side, discrepant data has also shown residual fragments having no significant impact on quality of life with re-intervention being associated with worsening of quality of life. Given the incongruity, more data must be collected before definitive conclusions can be made in regard to the management of residual fragments.
Presented by:
Daron Smith, MD, University College Hospital, London, United Kingdom
Amy Krambeck, MD, Northwestern University, Chicago, Illinois, USA
Thomas Tailly, MD, MSc, FEBU, PhD, University Hospital Gent, Ghent, Belgium
Written by: Rohit Bhatt, Leadership and Innovation Research Fellow, Department of Urology, University of California Irvine, @RohitBhatt_ on Twitter during the 2022 American Urological Association (AUA) Annual Meeting, New Orleans, LA, Fri, May 13 – Mon, May 16, 2022.
References:
1. Krambeck AE, et al. Renal Stone Disease: Proceedings of the Second International Urolithiasis Research Symposium. 2008
2. Raman JD, Bagrodia A, Gupta A, Bensalah K, Cadeddu JA, Lotan Y, Pearle MS. Natural history of residual fragments following percutaneous nephrostolithotomy. J Urol. 2009 Mar;181(3):1163-8. doi: 10.1016/j.juro.2008.10.162. Epub 2009 Jan 18. PMID: 19152935.
3. Altunrende F, Tefekli A, Stein RJ, Autorino R, Yuruk E, Laydner H, Binbay M, Muslumanoglu AY. Clinically insignificant residual fragments after percutaneous nephrolithotomy: medium-term follow-up. J Endourol. 2011 Jun;25(6):941-5. doi: 10.1089/end.2010.0491. Epub 2011 May 20. PMID: 21599528.
4. Emmott AS, Brotherhood HL, Paterson RF, Lange D, Chew BH. Complications, Re-Intervention Rates, and Natural History of Residual Stone Fragments After Percutaneous Nephrolithotomy. J Endourol. 2018 Jan;32(1):28-32. doi: 10.1089/end.2017.0618. Epub 2017 Nov 17. PMID: 29037066.
5. Degirmenci T, Bozkurt IH, Celik S, Yarimoglu S, Basmaci I, Sefik E. Does leaving residual fragments after percutaneous nephrolithotomy in patients with positive stone culture and/or renal pelvic urine culture increase the risk of infectious complications? Urolithiasis. 2019 Aug;47(4):371-375. doi: 10.1007/s00240-018-1063-9. Epub 2018 Jun 4. PMID: 29869167.
6. Agarwal DK, Krambeck AE, Sharma V, Maldonado FJ, Westerman ME, Knoedler JJ, Rivera ME. Treatment of non-obstructive, non-struvite urolithiasis is effective in treatment of recurrent urinary tract infections. World J Urol. 2020 Aug;38(8):2029-2033. doi: 10.1007/s00345-019-02977-3. Epub 2019 Oct 23. PMID: 31646382.
7. Brain E, Geraghty RM, Lovegrove CE, Yang B, Somani BK. Natural History of Post-Treatment Kidney Stone Fragments: A Systematic Review and Meta-Analysis. J Urol. 2021 Sep;206(3):526-538. doi: 10.1097/JU.0000000000001836. Epub 2021 Apr 27. PMID: 33904756.
8. Streeper NM, Galida M, Boltz S, Li S, Nakada SY, Raffin EP, Brown DR, Pais VM, Chan JYH, Scotland KB, Chew BH, Penniston KL. Is Stone-free Status After Surgical Intervention for Kidney Stones Associated With Better Health-related Quality of Life? - A Multicenter Study From the North American Stone Quality of Life Consortium. Urology. 2021 Feb;148:77-82. doi: 10.1016/j.urology.2020.09.058. Epub 2020 Dec 5. PMID: 33290774.