(UroToday.com) In a moderated poster presentation at the 2022 American Urologic Association Annual Meeting held in New Orleans and virtually, Dr. Lowentritt presented results of a real world study assessing the association between risk factors for cardiovascular (CV) disease and future CV events among men receiving androgen deprivation therapy (ADT) for prostate cancer. While ADT has been the foundation of advanced prostate cancer treatment for decades, since 2010, the FDA has required warnings for risk of cardiovascular (CV) disease in the labeling of Gonadotropin-Releasing Hormone (GnRH) receptor agonists. More recently, in 2021, the American Heart Association recommended a baseline assessment of CV risk in men starting ADT. However, the best approach to operationalize this in practice remains to be assessed.
The authors used a US claims dataset to identify men diagnosed with prostate cancer and receiving ADT between 2010-2019. The authors required continuous enrollment for at least 12 pre- and ≥6 months following the first ADT claim.

The authors examined CV events following initiation of ADT including hospital admission or emergency department visit with ICD-9/10 or CPT codes for either a cerebrovascular accident, coronary bypass graft, myocardial infarction, percutaneous coronary intervention, thrombosis, and/or unstable angina. The authors used a Cox regression model including pre-index covariates of age, CV history, radiation or prostate cancer surgery, or other metastatic drug therapy, and time on GnRH agonist to identify predictors of the time to first CV event up to 3 years following the initiation of ADT. Additionally, CV risk based on comorbidities and CV-related treatments were evaluated by groupings of high, moderate, and low risk scores.
The authors identified 10,530 men with prostate cancer who were treated with ADT, of whom 10,008 (95.5%) received a GnRH agonist during the 3-year observation period and 899 (8.98%) of whom experienced a CV event following the start of ADT. Based on multivariable Cox proportional hazards models, CV history was strongly associated wit the risk of subsequent hospitalization or emergency room visit for a CV event (HR=2.80, p <0.0001, [95% Confidence Interval (CI):2.37 - 3.31]).

In these models, a number of other variables were associated with the risk of CV event including high and moderate CV risk (vs low) (1.94, p <0.0001, [1.54 – 2.45] and 1.40, p <0.0049, [1.11 – 1.76], respectively), other metastatic drug therapy (1.62, p <0.001, [1.22 – 2.16]), time on GnRH agonist (1.05, p <0.0001, [1.02 – 1.07]) and age (1.06, p=0.04, [1.00-1.12]) were associated with higher risk for a CV event. Interestingly, patients who had previously undergone radiation or prostate cancer surgery had a lower risk of a CV event (HR=0.69, p <0.001, [95% CI: 0.57 – 0.84]).
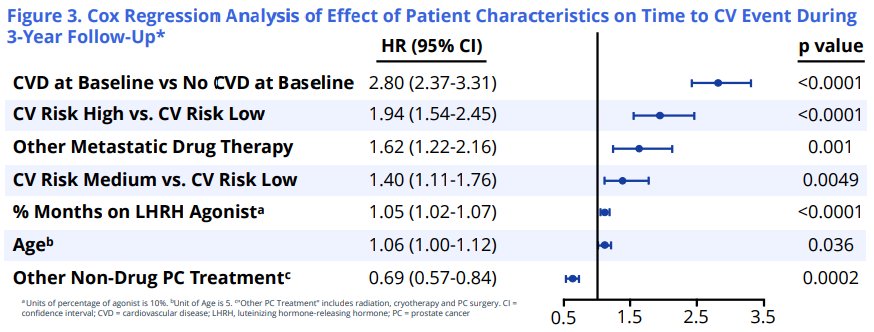
Thus, these authors conclude that a prior history of cardiovascular events was most strongly associated with a new CV event in the 3 years after starting ADT treatment.
Presented by: Benjamin Hugh Lowentritt, MD – Chesapeake Urology Associates. P.A