(UroToday.com) The 2022 Annual Meeting of the American Urological Association was host to the Confederación Americana de Urología (CAU) Lecture, presented by Dr. Rafael Sanchez-Salas, addressing the contemporary paradigms of high-risk, locally advanced and oligometastatic prostate cancer.
Dr. Sanchez-Salas outlined the following goals for his talk:
- Understand the importance of heterogeneity in high risk and locally advanced prostate cancer
- Apprehend the positive impact of molecular imaging on lesion localization and stratification in the prostate cancer pathway
- Conventional imaging is currently being replaced by next-generation imaging with a clear impact on therapeutic decision making
- Genomic markers can further contribute to clinical particularization
- Discuss the importance of local treatment to the primary as part of the therapeutic options for every patient
Dr. Sanchez-Salas highlighted the following facts regarding high-risk, locally advanced and oligometastatic prostate cancer:
- High-risk and locally advanced prostate cancer are heterogeneous stages of disease that vary in their clinical aggressiveness and associated oncologic outcomes
- Effective staging of high-risk and locally advanced prostate cancer can change the therapeutic decision in patients found with oligometastatic disease
- Novel imaging modalities have gained space in the diagnosis and staging of prostate cancer, and the diffusion of these tools will continue to expand
Definitions for high-risk, locally advanced prostate cancer vary, however, in essence, it is a variant that has a significant chance of developing local or systemic recurrence, and patients are at higher risk for symptoms and/or death from prostate cancer. Numerous risk stratification tools for predicting prostate cancer death rates are currently available:

A recent nomogram predicting the risk of prostate cancer specific mortality in pre-treated cT1-4N0-1M0 high-risk, localized prostate cancer patients, published by Dess et al. in JAMA Oncol, estimated a ten-year prostate cancer specific mortality rate of >10% in patients in the highest risk group category,1 emphasizing the importance of treatment intensification in this cohort.

Mossanen et al. demonstrated that the heterogeneity of high-risk prostate cancer may be secondary to the variability in existing definitions, which have a significant impact on the prognostic outcomes.
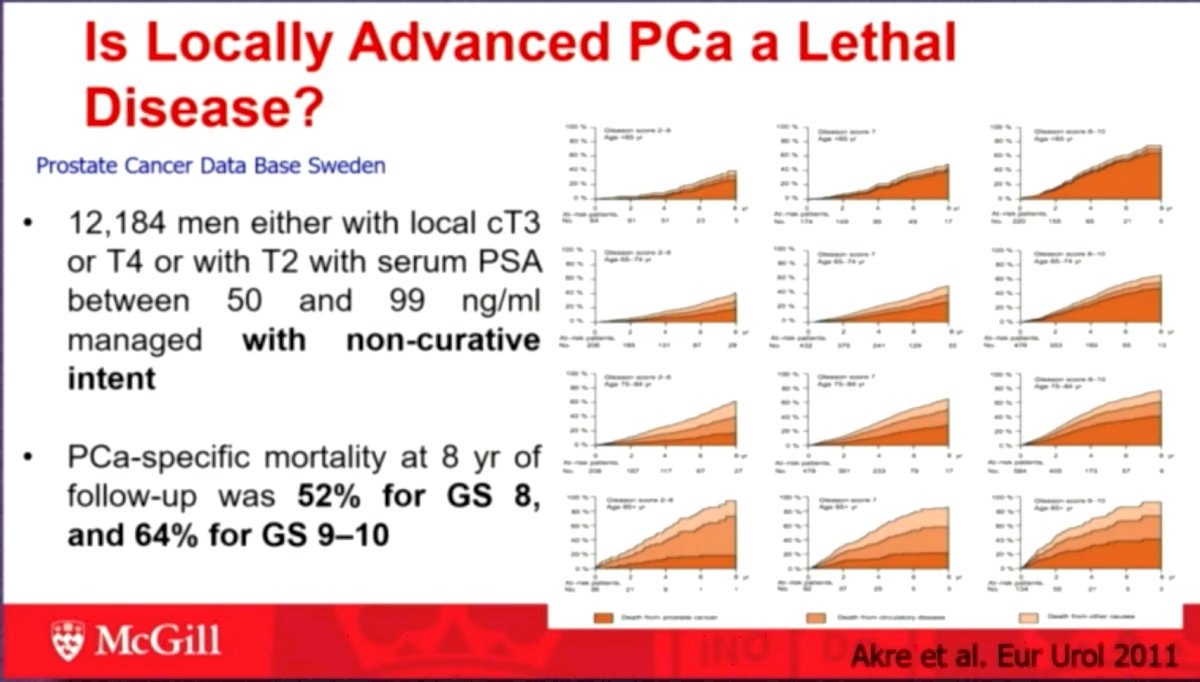
It has been well-established that locally advanced prostate cancer is a potentially lethal disease. Results from the Swedish Prostate Cancer Database evaluating 12,184 men with local cT3, T4, or cT2 with serum PSA between 50 and 99 ng/ml managed with non-curative intent have 8-year prostate-cancer specific mortality rates of 52% for Gleason Score (GS) 8 and 64% for GS 9-10.
Dr. Sanchez-Salas noted that we await the results of SPCG-15, which is a prospective randomized study comparing primary radical prostatectomy and primary radiotherapy plus androgen deprivation therapy for locally advanced prostate cancer.
With regards to the role of imaging in high-risk prostate cancer, multiparametric MRI (mpMRI) is useful for treatment planning, particularly in high-risk prostate cancer, with a PPV of 89% for extraprostatic extension with the 3T mpMRI. Prostate-specific membrane antigen (PSMA) imaging has a per-patient sensitivity of 77% and specificity of 97%. Quantitative PSMA parameters have similar potential to mpMRI for predicting extraprostatic extension of prostate cancer, with a significantly higher inter-reader agreement.
Given the diagnostic superiority of PSMA PET/CT as compared to conventional imaging, multiple guidelines have started to support the use of molecular imaging for staging. 68Ga-PSMA PET/CT has been shown to detect metastatic prostate cancer in 12.1% of men at initial diagnosis of prostate cancer. Around 25% of patients receiving PSMA PET/CT for intermediate/high-risk prostate cancer with negative imaging have cN1 or cM1 disease.
The prostate cancer oligometastatic disease space is a continuously changing paradigm with PSMA PET leading to the diagnosis of earlier stage disease, and new therapies changing survival and quality of life continuously emerging. Two questions thus arise:
- Should we treat the primary prostate cancer focus?
- Should we seek metastasis-directed therapy?
Dr. Sanchez-Salas went on to present the protocol for ARNEO, which is a single center, phase II, randomized placebo-controlled trials with 84 intermediate/high-risk prostate cancer patients amenable to radical prostatectomy with pelvic lymph node dissection who will undergo a 68Ga-PSMA-11 PET/MR and receive degarelix at standard dosage followed by either apalutamide (60 mg) or placebo for 12 weeks. Within thirty days from the last study medication intake, the same imaging will be repeated. Every patient will undergo PSA and testosterone testing the day of randomization, before the first drug intake, and after the last dose. Formalin-fixed paraffin-embedded tumor samples will be collected and used for transcriptome analysis, exome sequencing and immunohistochemistry. This study will allow for the evaluation of whether combined treatment with novel antiandrogens can result in (i) an increased proportion of patients with minimal residual disease, (ii) evaluate the molecular consequences of treatment intensification neoadjuvant, (iii) evaluate the consequences of new generation androgen receptor pathway inhibitors on 68 Ga-PSMA-11 PET/MR.2
High risk, locally advanced and oligometastatic prostate cancers might have similar clinical behavior. Contemporary detection of oligometastatic prostate cancer reflects the impact of novel imaging. Treatment of this heterogeneous population should take into account:
- Life expectancy
- Patients’ expectations
- Quality of life impact
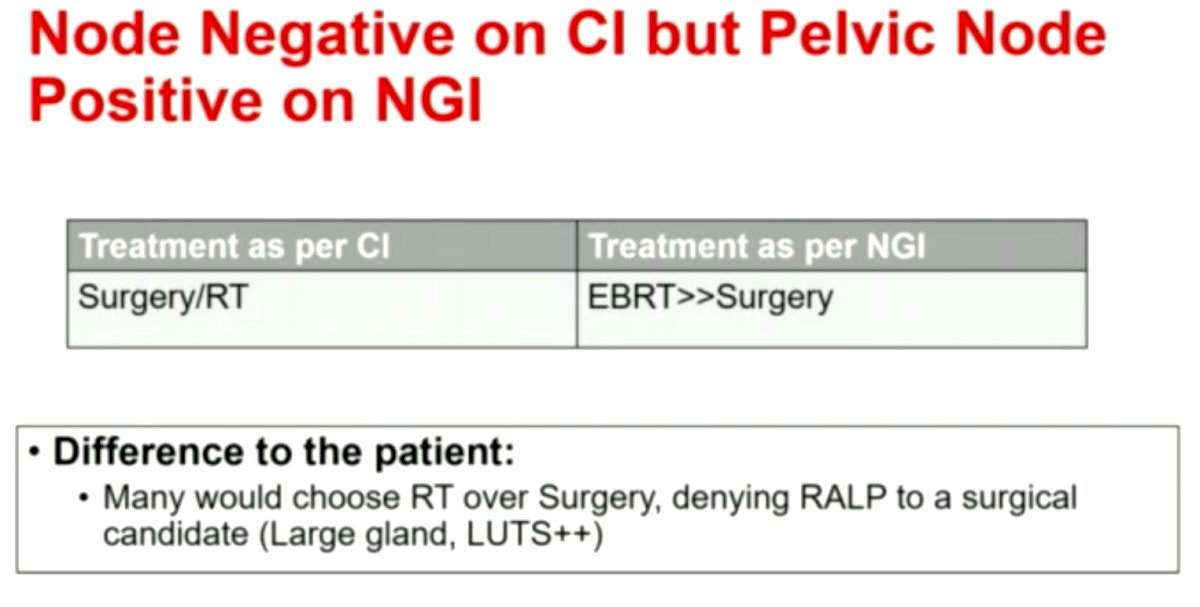
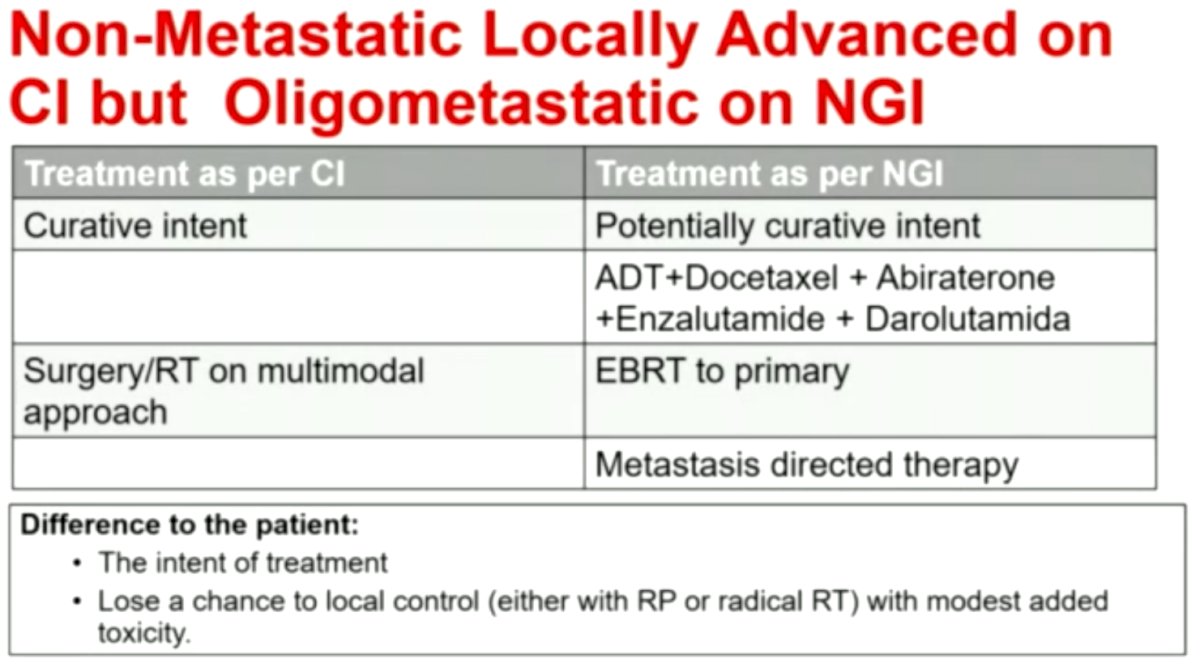
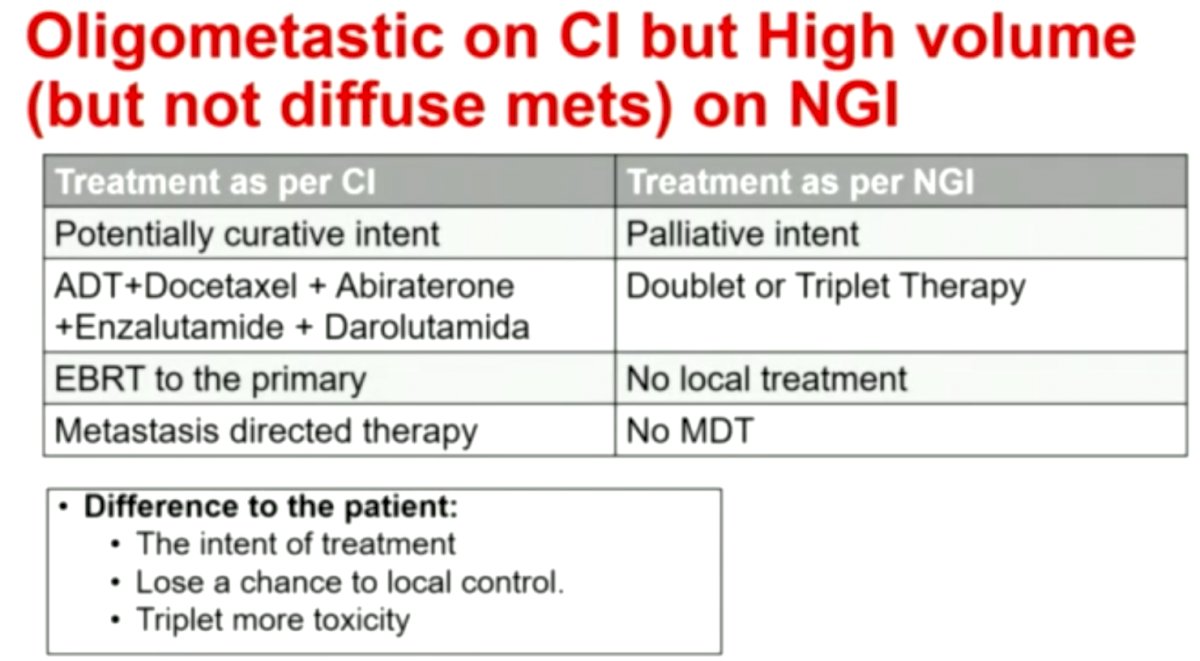
Several case scenarios can thus be expected after imaging stratification:
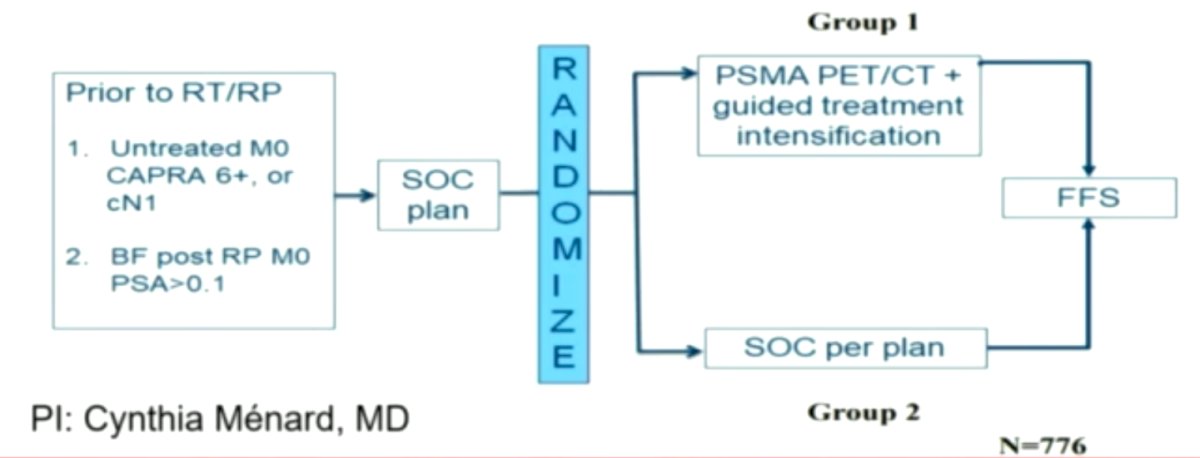
Dr. Sanchez-Salas went on to present the PATRON trial, which will evaluate PSMA PET/CT guided intensification of therapy in patients at risk of advanced prostate cancer.
Dr. Sanchez-Salas concluded his presentation as follows:
- Locally advanced and oligometastatic prostate cancer:
- Understanding the most appropriate strategy for each patient is still an unsolved question
- Patient and disease characteristics are essential for decision making
- Heterogenous disease
- Personalized treatment is needed
- Imaging and biomarkers are here to stay
- Ask about the patient’s expectations
- Biology prevails Stratify patients
- Understanding the most appropriate strategy for each patient is still an unsolved question
Presented by: Rafael Sanchez-Salas, MD, Associate Professor of Urology, Department of Surgery, McGill University, Montreal, Quebec
Written by: Rashid Sayyid, MD, MSc – Urology Chief Resident, Augusta University/Medical College of Georgia, @rksayyid on Twitter during the 2022 American Urological Association (AUA) Annual Meeting, New Orleans, LA, Fri, May 13 – Mon, May 16, 2022.
References:
- Dess RT, Suresh K, Zelefsky MJ, et al. Development and Validation of a Clinical Prognostic Stage Group System for Nonmetastatic Prostate Cancer Using Disease-Specific Mortality Results From the International Staging Collaboration for Cancer of the Prostate. JAMA Oncol. 2020;6(12):1912-1920.
- Tosco L, Laenen A, Gevaert T, et al. Neoadjuvant degarelix with or without apalutamide followed by radical prostatectomy for intermediate and high-risk prostate cancer: ARNEO, a randomized, double blind, placebo-controlled trial. BMC Cancer. 2018;18(1):354.