(UroToday.com) The 2022 Annual Meeting of the American Urological Association was host to an AUA guidelines update session focused on renal masses, presented by Dr. Steven Campbell, MD, PhD.
Dr. Campbell began his presentation by stating that the primary focus of these guidelines is clinically localized renal masses suspicious for cancer in adults, including solid enhancing renal tumor and Bosniak 3 and 4 complex cystic renal masses. The literature is updated through January 2021 in this version of the guidelines and updated risk-based surveillance protocols for patients after intervention are merged into this document, whereas previously this was a separate guideline.
What is new or different for this version of the guidelines (2021-2022)?
- Indications for genetic counseling are expanded
- For the first time, the issue of adjuvant therapy has been addressed
- Regarding imaging, MRI with contrast can now be used even in patients with severe CKD or with ESRD
- Indications for RMB are more clearly defined: utility-based approach
- Issue of deciding about radical versus partial nephrectomy are now more clearly stated to make recommendations more granular and useful
- Indications and rational for active surveillance are now more granular, and follow up on active surveillance now is more explicitly defined
Dr. Campbell presented the guidelines as follows:
Evaluation/Diagnosis:
- Obtain high quality, multiphase, cross-sectional abdominal imaging to optimally characterize and clinically stage the renal mass.
- MRI with contrast can now be obtained even in patients with severe CKD or ESRD
- Risk of nephrogenic fibrosis with 2nd generation gadolinium agents is extremely low
Renal Mass Biopsy:
- Renal mass biopsy (RMB): counsel patients regarding the rationale, positive/negative predictive values, potential risks and non-diagnostic rates of RMB
- RMB should be considered when a mass is suspected to be hematologic, metastatic, inflammatory, or infectious
- Language changed to emphasize utility-based approach
- Should do RMB whenever it might influence management
- Young/healthy patients who are unwilling to accept the uncertainties associated with RMB
- Older/frail patients who will be managed conservatively independent of RMB
Counseling:
- A urologist shoul;d lead the counseling process and should consider all management strategies. A multidisciplinary team should be included when needed.
- Counseling should include current perspectives about tumor biology and a patient-specific oncologic risk of many small renal masses should be reviewed
- Counseling should review the most common and serious urologic and non-urologic morbidities of each treatment pathway and the importance of patient age, comorbidities/frailty, and life expectancy.
- Physicians should review the importance of renal dunctional recovery related to renal mass management, including risk of progressive CKD, potential short/long-term need for dialysis, and long-term overall survival considerations
- Consider referral to nephrology in patients with a high risk of CKD progression, including those with GFR <45 ml/min, confirmed proteinuria, diabetics with pre-existing CKD, or whenever GFR is expected to be <30 ml/min after intervention.
- Clinicians should recommend genetic counseling for any of the following: all patients ≤ 46 years of age with renal malignancy, those with multifocal or bilateral renal masses, or whenever 1) the personal or family history suggests a familial renal neoplastic syndrome; 2) there is a first-or second-degree relative with a history of renal malignancy or a known clinical or genetic diagnosis of a familial renal neoplastic syndrome (even if kidney cancer has not been observed); or 3) the patient’s pathology demonstrates histologic findings suggestive of such a syndrome.
- Expanded indications for genetic counseling: 4-6% of cases of renal cell carcinoma are now thought to be familial
Partial nephrectomy and nephron-sparing approaches:
- Prioritize partial nephrectomy for the management of the cT1a renal mass when intervention is indicated
- Prioritize nephron-sparing approaches for patients with an anatomically or functionally solitary kidney, bilateral tumors, known familial RCC, preexisting CKD, or proteinuria
- Consider nephron-sparing approaches for patients who are young, have multifocal masses, or comorbidities that are likely to impact renal function in the future.
Principles related to partial nephrectomy:
- Prioritize preservation of renal function by optimizing nephron mass preservation and avoiding prolonged warm, ischemia
- Negative surgical margins should be a priority. The extent of normal parenchyma removed should be determined by surgeon discretion taking into account the clinical situation and tumor characteristics, including growth pattern, and interface with normal tissue. Tumor enucleation should be considered in patients with familial RCC, multifocal disease, or severe CKD to optimize parenchymal mass preservation.
Radical nephrectomy:
- Physicians should consider RN for patients with a solid or Bosniak 3/4 complex cystic renal mass whenever increased oncologic potential is suggested by tumor size, RMB (if obtained), and/or imaging. (Moderate Recommendation; Evidence Level: Grade B) In this setting, RN is preferred if all of the following criteria are met: 1) high tumor complexity and PN would be challenging even in experienced hands; 2) no preexisting CKD or proteinuria; and 3) normal contralateral kidney and new baseline eGFR will likely be greater than 45 mL/min/1.73m2 even if RN is performed. If all of these criteria are not met, PN should be considered unless there are overriding concerns about the safety or oncologic efficacy of PN.
- AUA guidelines are the only one that provides a granular description of criteria for radical nephrectomy. The goal is utilization of radical nephrectomy for patients who really need it, while reducing overutilization of radical nephrectomy.
Other considerations after partial or radical nephrectomy:
- Pathologic evaluation of the adjacent renal parenchyma should be performed and recorded after partial or radical nephrectomy to assess for possible nephrologic disease, particularly for patients with CKD or risk factors for developing CKD.
- Clinicians should consider referral to medical oncology whenever there is concern for potential clinical metastasis or incompletely resected disease (macroscopic positive margin or gross residual disease). Patients with high-risk or locally advanced, fully resected renal cancers should be counselled about the risks/benefits of adjuvant therapy and encouraged to participate in adjuvant clinical trials, facilitated by medical oncology consultation when needed.
- This is a modification to the previous guidelines. A new statement about adjuvant treatment was added given the emergence of data showing potential benefit for immunotherapy in this setting (KEYNOTE-564)
Thermal Ablation;
- Clinicians should consider thermal ablation (TA) as an alternate approach for the management of cT1a solid renal masses <3 cm in size. A percutaneous technique is preferred.
- Both radiofrequency ablation (RFA) and cryoablation are options
- A RMB should be performed prior to or at the time of ablation to provide pathologic diagnosis and guide subsequent surveillance.
- RMB should be performed prior to TA if possible to facilitate more rational management
Active Surveillance:
- For patients with a solid renal mass <2cm, or those that are complex but predominantly cystic, clinicians may elect AS with potential for delayed intervention for initial management.
- This version of the guidelines now identifies patients with masses <2 cm or those that are predominantly cystic as strong candidates for AS
- Repeat cross-sectional imaging should be obtained approximately 3-6 months later to assess for interval growth. Periodic clinical/imaging surveillance can then be based on growth rate and shared decision-making with intervention recommended if substantial interval growth is observed or if other clinical/imaging findings suggest that the risk/benefit analysis is no longer equivocal or favorable for continued AS.
Dr. Campbell outlined factors favoring AS/expectant management:
- Patient-related
- Elderly
- Life expectancy <5 years
- High comorbidities
- Excessive perioperative risk
- Frailty/poor functional status
- Patient preference for AS
- Marginal renal function
- Tumor-related
- Tumor size <3 cm
- Tumor growth <5 mm/year
- Non-infiltrative
- Low complexity
- Favorable histology
- Predominantly cystic
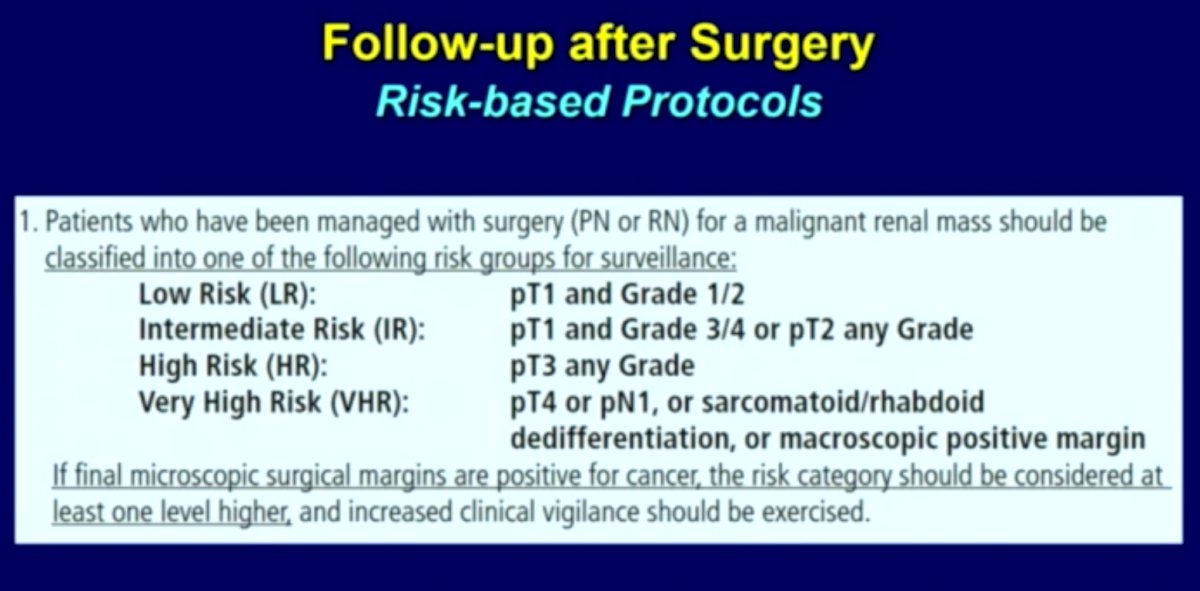
In this iteration of the renal mass guidelines, follow-up after intervention has been merged into the guidelines and revised extensively.
General Principles of Follow-up after Intervention:
- Discuss the implications of stage, grade, and histology including the risks of recurrence and possible sequelae of treatment. Patients with pathologically-proven benign renal masses should undergo occasional clinical evaluation and laboratory testing for sequelae of treatment but most do not require routine periodic imaging.
- Patients with treated malignant renal masses should undergo periodic medical history, physical examination, laboratory studies, and imaging directed at detecting signs and symptoms of metastatic spread and/or local recurrence as well as evaluation for possible sequelae of treatment.
- Patients with treated malignant renal masses should have periodic laboratory testing including serum creatinine, eGFR, and urinalysis. Other laboratory evaluations (e.g., complete blood count, lactate dehydrogenase, liver function tests, alkaline phosphatase and calcium level) may be obtained at the discretion of the clinician or if advanced disease is suspected.
- Patients undergoing follow-up for treated renal masses with progressive renal insufficiency or proteinuria should be referred to nephrology.
- Patients undergoing follow-up for treated malignant renal masses should only undergo bone scan if one or more of the following is present: clinical symptoms such as bone pain, elevated alkaline phosphatase, or radiographic findings suggestive of a bony neoplasm.
- Patients undergoing follow-up for treated malignant renal masses with acute neurological signs or symptoms should undergo prompt magnetic resonance imaging (MRI) or computed tomography (CT) scanning of the brain and/or spine.
- For patients undergoing follow-up for treated malignant renal masses, additional site-specific imaging can be ordered as warranted by clinical symptoms suggestive of recurrence or metastatic spread. Positron emission tomography (PET) scan should not be obtained routinely but may be considered selectively.
- Patients with findings suggestive of metastatic renal malignancy should be evaluated to define the extent of disease and referred to medical oncology. Surgical resection or ablative therapies should be considered in select patients with isolated or oligo-metastatic disease.
- Patients with findings suggesting a new renal primary or local recurrence of renal malignancy should undergo metastatic evaluation including chest and abdominal imaging. If the new primary or recurrence is isolated to the ipsilateral kidney and/or retroperitoneum, a urologist should be involved in the decision-making process, and surgical resection or ablative therapies may be considered.

- Patients managed with surgery (partial or radical nephrectomy) for a renal malignancy should undergo abdominal imaging according to the above table1, with CT or MRI pre- and post-intravenous contrast preferred. After 2 years, abdominal ultrasound alternating with cross-sectional imaging may be considered in the low and intermediate risk groups at physician discretion. After 5 years, informed/shared decision-making should dictate further abdominal imaging.
Follow up after Thermal Ablation:
- Patients undergoing ablative procedures with biopsy that confirmed malignancy or was non-diagnostic should undergo pre- and post-contrast cross-sectional abdominal imaging within 6 months (if not contraindicated). Subsequent follow-up should be according to the recommendations for the intermediate risk postoperative protocol in the above Table 1.
Presented by: Steven Campbell, MD, PhD, Professor of Surgery, Program Director and Vice Chair of Urology, Cleveland Clinic, Cleveland, OH
Written by: Rashid Sayyid, MD, MSc – Urology Chief Resident, Augusta University/Medical College of Georgia, @rksayyid on Twitter during the 2022 American Urological Association (AUA) Annual Meeting, New Orleans, LA, Fri, May 13 – Mon, May 16, 2022.
References:
- Campell SC, Clark PE, Chang SS et al: Renal Mass and Localized Renal Cancer: Evaluation, Management, and Follow-Up: AUA Guideline Part I. J Urol 2021; 206: 199.
- Campbell SC, Uzzo RG, Karam JA, et al: Renal Mass and Localized Renal Cancer: Evaluation, Management, and Follow-up: AUA Guideline: Part II. J Urol 2021; 206: 209.