(UroToday.com) The 2022 American Urological Association (AUA) Annual Meeting included the International Prostate Forum session and a presentation by Dr. Kirsten Greene discussing robotic-assisted radical prostatectomy (RARP) modifications that enhance continence return.
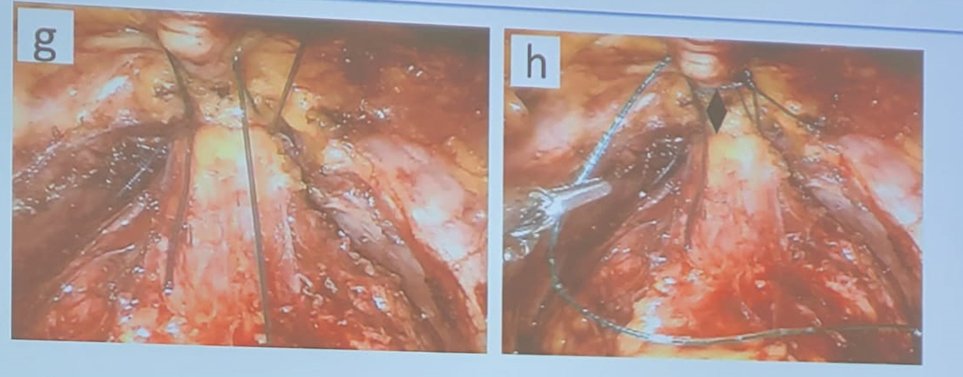
Dr. Greene began by emphasizing that urinary incontinence is “one of the most feared side effects” of radical prostatectomy given the effect it may have on quality of life. She further noted that definitions of urinary incontinence of urologic oncologists may differ from those employed by our colleagues in reconstruction (1 pad for protection vs totally pad free). Further, she highlighted that surgical technique matters in terms of urinary continence, and particularly, that there are modifications that may be made to improve the time to continence. She then highlighted a number of basic principles that form the foundation of continence recovery following radical prostatectomy including the maintenance of urethral length, the maintenance or recreation of urethral support (via anterior suspension to the puboprostatic ligaments), reconstruction of posterior support (using a Rocco stitch), and bladder neck preservation or reconstruction, including a detrusor wrap.
Among these, she highlighted first the periurethral suspension stitch. The use of this approach was associated with significant early improvements in continence with 3-month continence rates improving from 35% to 615.
She noted that there are meaningful differences between preservation of the bladder neck and its reconstruction. While preservation means that the bladder neck and urethra are maintained at the same diameter, reconstruction involves the use of sutures at 3-o’clock and 9-o’clock to reconstitute this anatomy. Notably, use of this surgical approach is associated with favourable pad free rates at 1-week (60% vs 54%) and at 3-months (80 vs 78%). Further, there was no difference in margin rates.
Dr. Greene then discussed Retzius sparing prostatectomy.
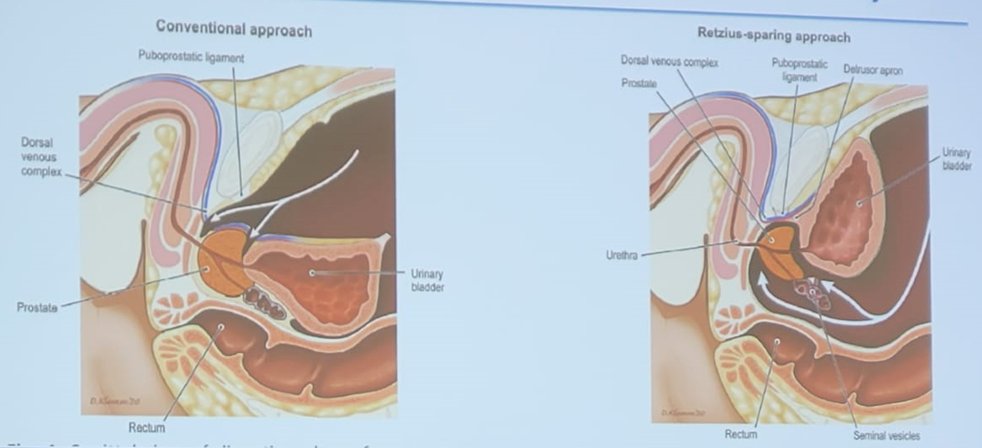
She highlighted a relatively recent Cochrane review comparing this Retzius-sparing approach with a standard robotic assisted laparoscopic prostatectomy. At one-week post-operatively, this systematic review and meta-analysis demonstrated favourable continence outcomes with a risk ratio of 1.74 (95% CI 1.41-2.14) compared to the standard robotic approach. Moving forward to three-months post-operatively, this benefit remained though the magnitude of effect was attenuated (risk ratio 1.33, 95% CI 1.06-1.68). However, by six-months post-operatively, Dr. Greene noted that there was no longer any difference between these two surgical approaches (risk ratio 1.09, 95% CI 0.99-1.20).
Beyond the data from this systematic review, she highlighted a randomized controlled trial from Delala and colleagues demonstrating the time to total continence (0 pads) or continence with a single security liner was significantly faster among patients who were randomized to the Retzius-sparing approach.
However, she noted that one of the potential downsides to this approach is an increase in positive surgical margins. In the Cochrane systematic review, while relying on only three studies to inform the question, the authors found an increased rate of positive surgical margins favouring Retzius-sparing (risk ratio 1.95 (95% CI 1.19-3.20).
She then discussed an alternative approach, termed the “Hood technique”, proposed by Dr. Tewari and colleagues in which an anterior approach is used but with preservation of the periurethral tissue in the space of Retzius. This allows for a more familiar surgical approach with the continence benefits of the Retzius-sparing technique but also with a lower positive margin rate. Across a number of studies comparing prospectively collected outcomes, this approach showed favourable time to return of continence compared to other studies of the Retzius-sparing approach.
Further, compared to other reports of the Retzius-sparing approach, this Hood technique was associated with lower positive surgical margin rates for both T2 (2.3% vs 7.9 to 25%) and T3 (3.7% vs 36-47%) disease. Additionally, complication rates were comparable or lower with this approach, potentially reflecting the authors experience and comfort with the familiarity of this approach being anterior.
Thus, she addressed the question of which approach should be preferred. She noted there are a number of ways to maintain or recreate urethral support including Retzius-sparing, the Hood technique, or a sling/stitch. Further, we can consider bladder neck preservation or reconstruction. In terms of preservation of the vasculature to the sphincter, both the Retzius-sparing technique and Hood technique achieve this. However, in terms of the detrusor apron, the Retzius-sparing approach preserves this while the Hood technique relies on reconstruction. In terms of positive surgical margins, the Hood technique or anterior approach appears to be favourable.
Thus, she highlighted that we should seek to perform a “less radical” prostatectomy by saving as much support as we possibly can through use of the anterior Hood, Retzius-sparing, and bladder neck sparing. Further, where dissection is required, she advocated “putting things back the way you found them”. She noted that all structures in the pelvis are important and we continue to learn about their importance in continence. Thus, she closed by emphasizing the importance of adhering to oncologic principles and respecting tissues.
Presented by: Kirsten Greene, MD, MAS, FACS, Professor of Urology, University of Virginia, Charlottesville, VA
Written by: Christopher J.D. Wallis, University of Toronto Twitter: @WallisCJD during the 2022 American Urological Association (AUA) Annual Meeting, New Orleans, LA, Fri, May 13 – Mon, May 16, 2022.