(UroToday.com) The 2022 Annual Meeting of the American Urological Association (AUA) was host to The International Bladder Cancer Group (IBCG) AUA Bladder Cancer Forum which featured a State-of-the-Art lecture by Dr. Seth Lerner regarding the current state of BCG unresponsive disease.
Dr. Lerner began his talk by introducing the revised definition of “BCG Unresponsive” high risk non-muscle invasive bladder cancer (NMIBC).
- Recurrent CIS +/- Ta or T1 within 12 months of completion of adequate BCG (At least 5 induction courses, 2 maintenance)
- Recurrent/persistent HGTa/T1 within 6 months of completion of adequate BCG
- T1HG at first evaluation after induction BCG (At least 5 induction courses)
- There is flexibility in use of 6- and 12-month time periods
Cystectomy remains the standard of care and this is supported by the current AUA guidelines. There is clear data from retrospective analyses that early radical cystectomy is associated with superior 5-year cancer specific survival rates when compared to delayed cystectomy for HG T1 patients (83% versus 67%). Very high risk NMIBC should not be treated with intravesical therapy if the patient is fit for surgery:
- Variant histology, lymphovascular invasion, multifocal/large volume HGT1/CIS, prostatic urethral cancer involvement
- Lerner highlighted the significance of prostatic urethral involvement with such patient having a 12.2-fold increased hazard of developing muscle invasive disease.
Dr. Lerner next elaborated on the FDA’s guidance with clinical trial design in the BCG-unresponsive disease space. Randomizing patients with BCG-unresponsive disease to a minimally effective drug as a concurrent control raises ethical concerns. Because effective drugs are not available and the alternative treatment is cystectomy, single-arm trials of patients with BCG unresponsive CIS disease with or without papillary disease are appropriate. The primary endpoint should be complete response and durability in patients with CIS.
Current alternatives to cystectomy when BCG fails the patients include:
- BCG/Interferon (for induction only – no longer readily available)
- Valrubicin, Pembrolizumab: only FDA approved drugs (CIS +/- Ta, T1)
- Gemcitabine
- Mitomycin +/- heat or microwave
- Gemcitabine/Mitomycin
- Gemcitabine/Docetaxel
- Clinical Trials
Valrubicin was the first agent approved in this disease space. 80 patients with CIS, 39% of whom had received at least 2 prior courses of BCG, received 6 or 9 weeks of Valrubicin. At 3 months, 35% of patients had no evidence of disease (positive cytology was allowed). The complete response rate at 6 months was 18% and at 2 years only 4% were disease free.1
Pembrolizumab was the next agent approved by the FDA in this disease space. Keynote-057 was a phase two clinical trial of 102 patients (96 in efficacy cohort). 64% of patients had CIS alone. Complete response at 3 months was achieved in 41% of patients and, among those who achieved this outcome, 53% maintained a complete response for greater than 9 months. Toxicities were as follows:
- Any grade: 66%
- Immune mediated: 22: 3%
- Immune-mediated Grade 3-4: 3%
- Discontinuation: 9%
- Immune mediated: 22: 3%
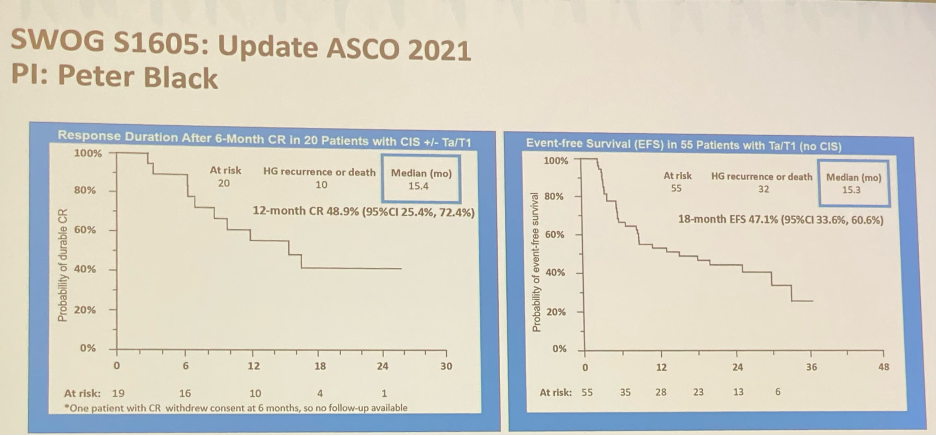
Updated results of SWOG S1605 led by Dr. Peter Black were recently presented at ASCO 2021. This was a single-arm phase II registration trial testing systemic atezolizumab (1200 mg IV) every 3 weeks for one year that aimed to enroll 135 (70 CIS and 65 non-CIS) eligible patients with histologically proven BCG-unresponsive high-risk NMIBC who were unfit for or declined radical cystectomy. The latest assessment reported the 18-month results for all eligible patients who received at least one protocol treatment. The co-primary endpoints were pathological complete response rate at 6 months in patients with CIS, and event-free survival in all patients at 18 months using Kaplan-Meier methods, conditional on a positive CIS response rate. Event-free survival in the subset with Ta/T1 disease and duration of response in CIS patients were secondary endpoints.
In this trial, there were 172 patients enrolled, of which 166 received at least one dose of atezolizumab and were included in the safety analysis, and, of those, 128 were eligible and included in the efficacy analysis. As previously reported, 20 (27%) out of 74 patients with CIS attained a pathologic complete response at 6 months. The Kaplan Meier estimate of 12 months duration of response after 6-month complete response for CIS patients was 48.9% (95% CI 25.4% to 72.4%) and the median duration of response was 15.4 months. The Kaplan Meier event-free survival rate at 18 months in 74 patients with CIS was 17% (90% CI 9%, 25%), and the 18 months Kaplan Meier event-free survival rate in the overall population of 128 patients with Ta, T1, and CIS was 29% (90% CI 22%, 36%). The 18-month actuarial event-free survival rate in 55 patients with Ta/T1 disease was 47.1% (95% CI 33.6 to 60.6%).2
Steinberg et al have demonstrated retrospectively that sequential gemcitabine/docetaxel in this cohort has demonstrated efficacy. The 2-year recurrence free survival for the overall cohort was 46%.
- BCG unresponsive cases (with CIS): 50%
- BCG unresponsive cases (papillary alone); 58%
The 2-year progression free rate was 7%, and there was a low rate of discontinuation due to side effects (3.3%).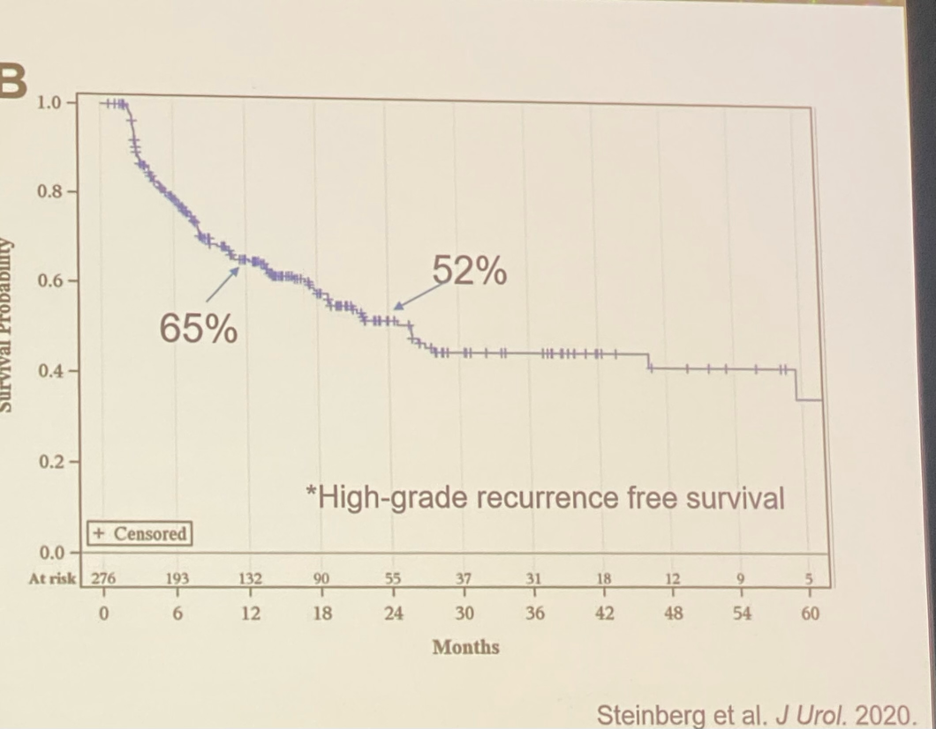
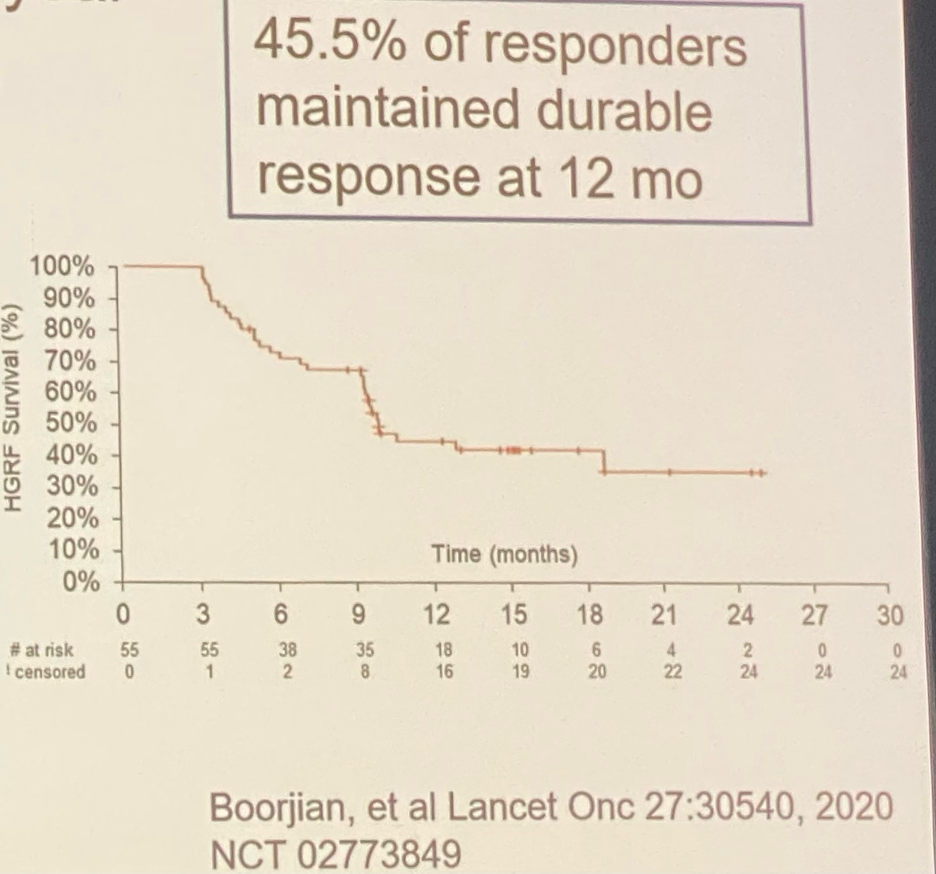
Phase 3 results for Nadoferagene Firadenovec (Phase 3 Adstiladrin®), given every 3 months for 1 year in 157 patients with BCG unresponsive disease:
- CIS patients:
- 3 months RFS: 53%
- 1-year RFS: 24%
- Median duration of CR: 9.7 months
- HG Ta/T1 [patients:
- 3 months RFS: 73%
- 1-year RFS: 44%
- Median duration of CT: 12.5 months
The phase III VISTA trial of Oportuzumab Monatox (ViciniumTM), a single fusion protein comprising an anti-EpCAM antibody fragment, peptide tether, and cytotoxic payload that delivers a toxin that kills tumor cells by blocking protein synthesis, was evaluated in 126 BCG-unresponsive patients. This drug is instilled for 2 hours twice weekly for 6 weeks, then weekly for 6 weeks. The maintenance regimen is instillation every 2 weeks for up to 2 years.
- 89 patients with CIS
- CR at 3 months: 40%
- Among CR patients
- Median duration of response: 9.4 months (95% CI: 5.1-NE)
- 52% remained disease free for 9 months and 36% at 15 months after starting treatment
- RFS in 38 patients with papillary disease
- 3 months: 71%
- 6 months: 58%
- 12 months: 50%
- 24 months: 37%
- Median time to recurrence: 13.2 months (95% CI: 5.6-NE)
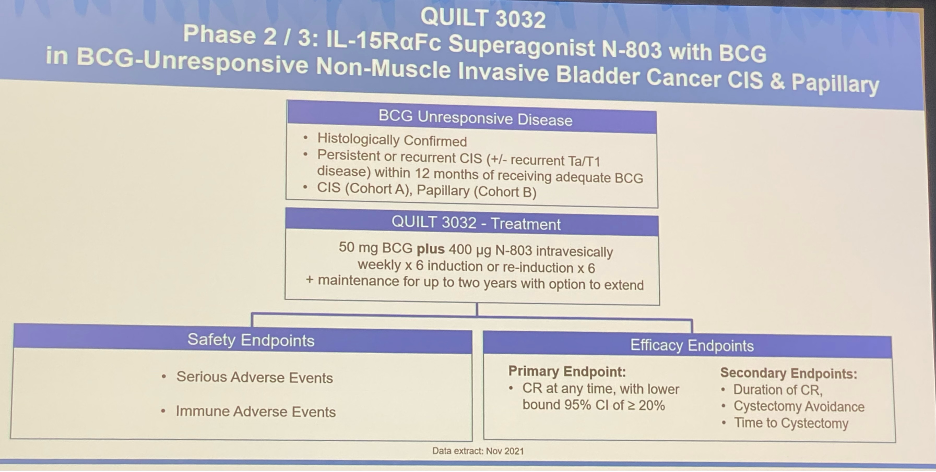
Dr. Lerner went on to present results from the recent QUILT 3032 trial, where patients with NMIBC were randomized to 50 mgBCG plus 40 ug N-803 intravesically weekly x 6 induction or re-induction x6 with up to 2 years maintenance, with an option to extend. The 12 and 24 month durable complete remission in cohort A (CIS) was 60% (95% CI: 45-72%) and 52% (95% CI: 40-65%), respectively.


Next, Dr. Lerner provided the study framework of the ALLIANCE trial (intravesical gemcitabine + systemic pembrolizumab):
Radiotherapy has historically had a limited role for NMIBC. Favorable results have been reported from a retrospective series of 141 patients with high-risk T1 disease treated with platinum-based chemoradiation, with a complete response rate of 88% and 5- and 10-year recurrence rates of 19% and 30%, respectively. As in trimodal therapy for muscle invasive disease, effectiveness for radiation declines if extensive CIS is present. The RTOG 0926 is a prospective trial of chemoradiation with 5-GU and mitomycin following BCG failure for T1 disease, as conducted by the NRG Oncology team.
- Primary endpoint: freedom from cystectomy 88% at 3 years (ASTRO 2021)
Dr. Lerner concluded that chemoradiation may thus emerge as a viable alternative for select BCG unresponsive patients, especially those unfit for cystectomy.

Presented by: Dr. Seth Lerner, MD, Professor and Chair, Department of Urology, Baylor University, Houston, TX
Written by: Rashid Sayyid, MD, MSc – Urology Chief Resident, Augusta University/Medical College of Georgia, @rksayyid on Twitter during the 2022 American Urological Association (AUA) Annual Meeting, New Orleans, LA, Fri, May 13 – Mon, May 16, 2022.
References:
- Dinney et al. Intravesical valrubicin in patients with bladder carcinoma in situ and contraindication to or failure after bacillus Calmette-Guérin. Urol Onc. 2013;31:1635.
- ASCO 2021: Phase II Trial of Atezolizumab in BCG-Unresponsive Non-Muscle Invasive Bladder Cancer: SWOG S1605, June 2021. Retrieved from: https://www.urotoday.com/conference-highlights/asco-2021/asco-2021-bladder-cancer/129954-asco-2021-phase-ii-trial-of-atezolizumab-in-bcg-unresponsive-non-muscle-invasive-bladder-cancer-swog-s1605.html
- AUA 2022: Final Clinical Results of Pivotal Trial of IL-15R&[alpha]Fc Superagonist N-803 with BCG in BCG-Unresponsive Non-Muscle Invasive Bladder Cancer (NMIBC) CIS and Papillary CohortsMay 2022. Retrieved from: https://www.urotoday.com/conference-highlights/2022-annual-meeting/aua-2022-bladder-caner/137101-aua-2022-final-clinical-results-of-pivotal-trial-of-il-15r-alpha-fc-superagonist-n-803-with-bcg-in-bcg-unresponsive-non-muscle-invasive-bladder-cancer-nmibc-cis-and-papillary-cohorts.html