(UroToday.com) The 2022 Annual Meeting of the American Urological Association (AUA) was host to The International Bladder Cancer Group (IBCG) AUA Bladder Cancer Forum which featured a State-of-the-Art lecture by Dr. Matthew Galsky regarding systemic therapy options for non-metastatic, muscle-invasive bladder cancer (MIBC).
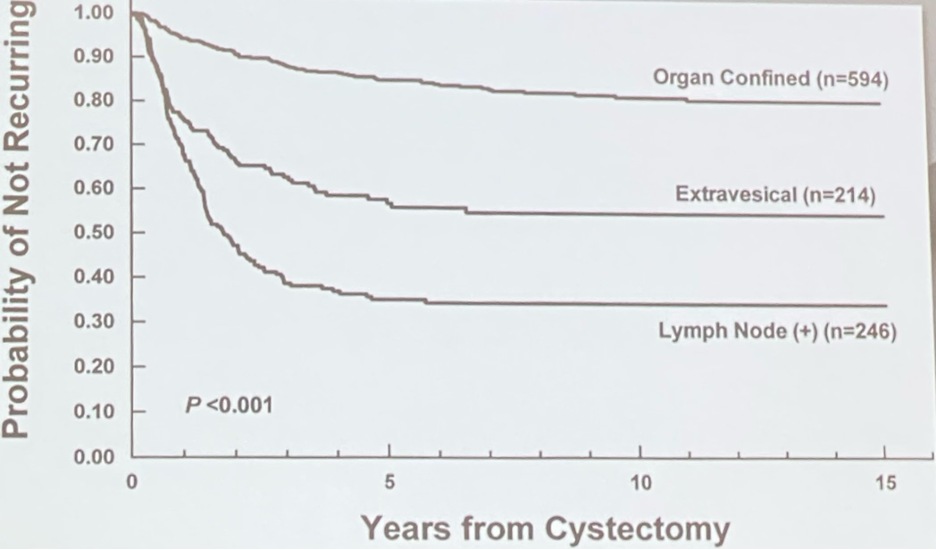
Dr. Galsky began his presentation by acknowledging that surgery alone is potentially curative for MIBC, but the risk of metastatic recurrence remains high.
At the current time, we don’t know who needs perioperative systemic therapy or who benefits from such therapy? These are related, yet distinct considerations. T and N staging are used to approximate who needs treatment, particularly pT3 and pN+ patients, but novel biomarkers such as ctDNA may help determine who benefits from treatment.
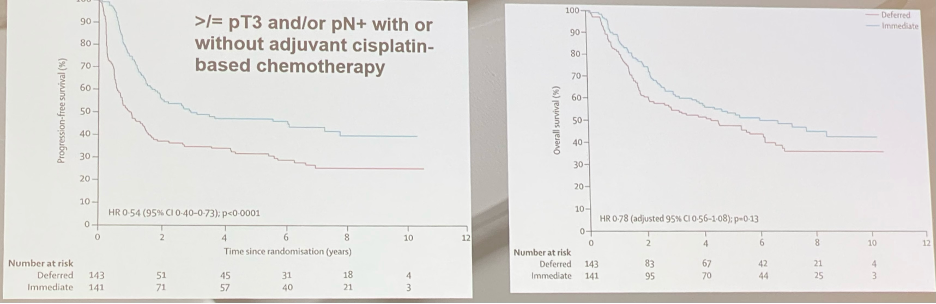
Completing perioperative chemotherapy trials has historically been challenging. The EORTC 30994 trial of immediate versus deferred chemotherapy after radical cystectomy in patients with pT3-4 or N+ M0 urothelial carcinoma of the bladder that randomized 284 of 660 planned patients to immediate adjuvant or deferred chemotherapy at relapse demonstrated superior progression-free survival (HR 0.54, 95% CI: 0.40-0.73) and non-significantly superior OS (HR 0.78, 95% CI: 0.56-1.08) in favor of immediate treatment.
Results from the pivotal trial by Grossman et al. demonstrated that the 5-year overall survival improved from 43% to 57% with neoadjuvant methotrexate, vinblastine, doxorubicin, and cisplatin.1
Another issue is that approximately 50% of patients can’t receive are cisplatin-ineligible. Even among those who do receive chemotherapy, residual cancer after neoadjuvant treatment is associated with poor prognosis and remains an unmet need.
How can we improve upon treatment of MIBC?
- Treatment regardless of cisplatin eligibility
- Treatment for patients with residual disease despite NAC (sequential and risk-stratified approach)
- Tools to inform who needs systemic therapy and who benefits
- De-escalation when possible
There are currently three trials (two with reported results) evaluating immune checkpoint inhibitors adjuvantly in patients with high-risk MIBC:
- pT2-4a or N+ for patients treated with neoadjuvant chemotherapy
- pT3-T4a pr N+ for patients declining or ineligible for neoadjuvant chemotherapy

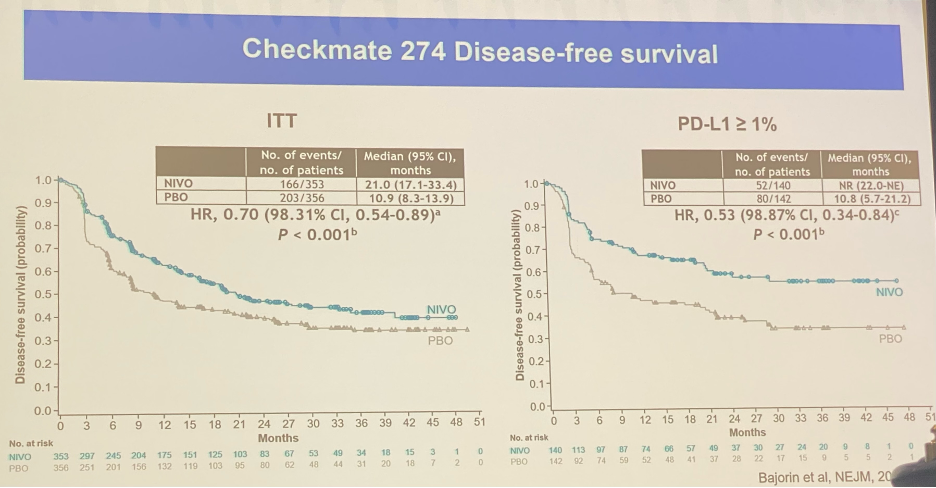
Checkmate-274 of adjuvant nivolumab was a positive trial, whereby patients in both the overall intention-to-treat population and PD-L1 >=1% experienced improved disease-free survival:2
- ITT: 21.0 months (17.1-33.4) versus 10.9 months (8.3-13.9)
- PD-L1 >=1%: NR (22.0-NE) versus 10.8 months (5.7-21.2)
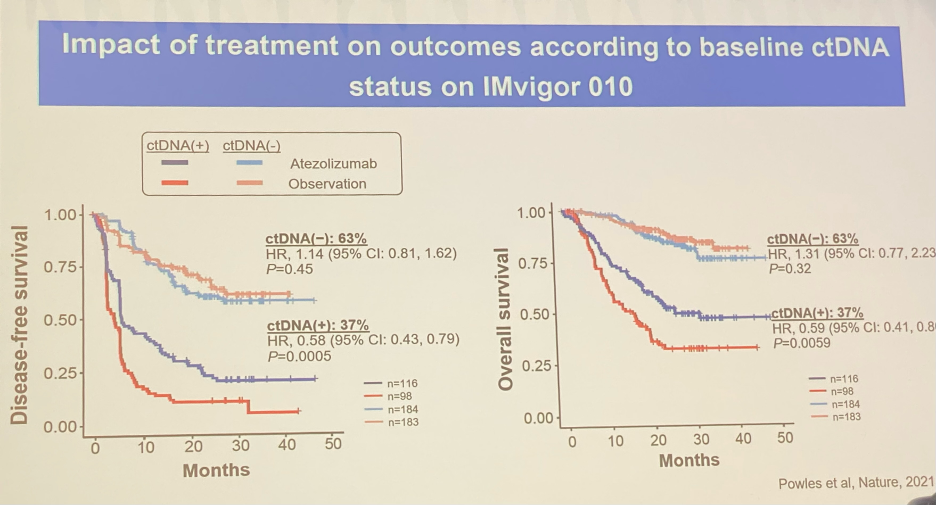
Although IMvigor-010 was a negative trial in the ITT population, data from the observation arm of 281 patients, risk-stratified by ctDNA status at baseline clearly demonstrated that patients who were ctDNA(+) had significantly worse disease-free survival (HR 6.3, p<0.001) and overall survival rates (HR 8.00, p<0.001).

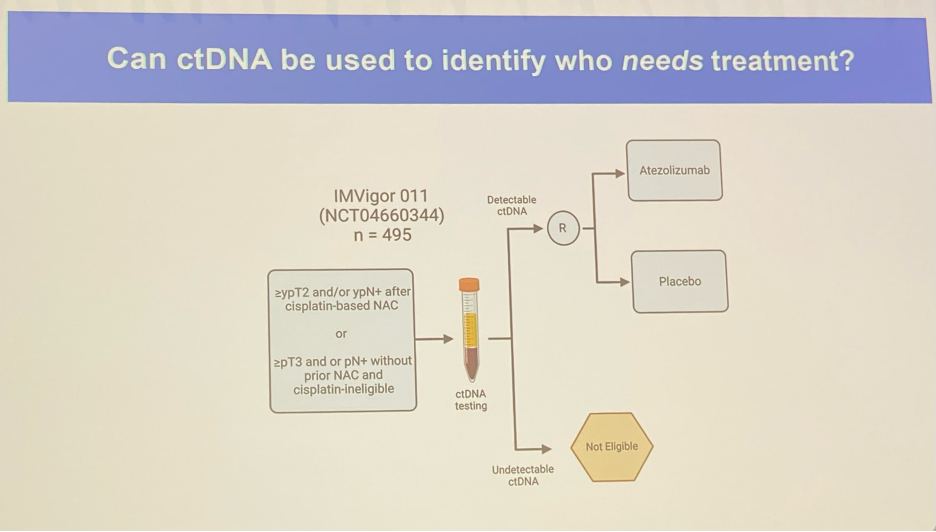
The next logical question was does response to adjuvant Atezolizumab vary by ctDNA status? Patients who were ctDNA(-) showed no improvement in DFS or OS with adjuvant therapy. Conversely, ctDNA(+) patients were noted to have improved DFS (HR 0.58, p<0.001) and OS (HR 0.59, p=0.006).3
IMVigor 011 (NCT04660344) will randomize patients with ctDNA(+), high-risk MIBC to adjuvant treatment versus placebo.
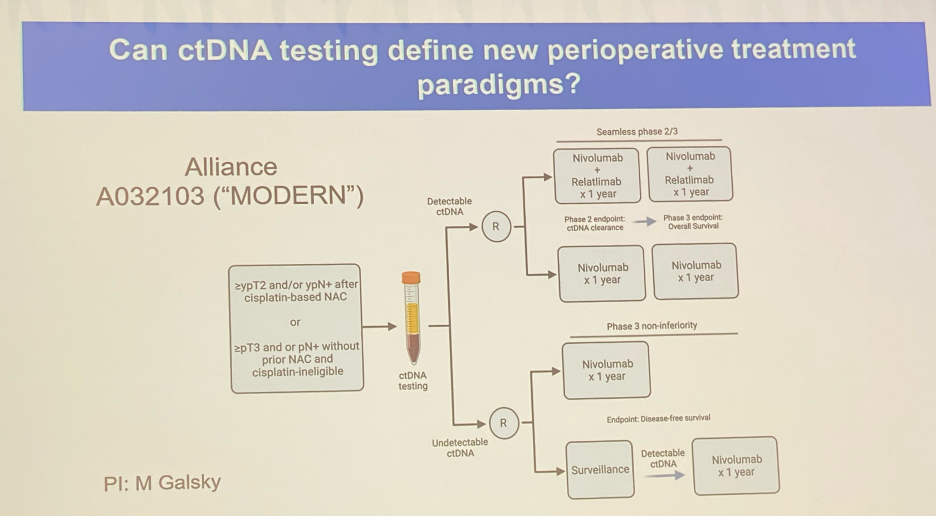
Next, Dr. Gaslky provided the study design for the Alliance A032103 (“MODERN”) that highlights how ctDNA testing may be able to define new, biomarker-based, patient-adapted perioperative treatment paradigms.
Dr. Galsky next provided a summary table of the current Phase 2 studies exploring neoadjuvant IO therapy. These trials have demonstrated pT0N0 rates of 7-46%, which are similar to those seen with historical neoadjuvant chemotherapy regimens.

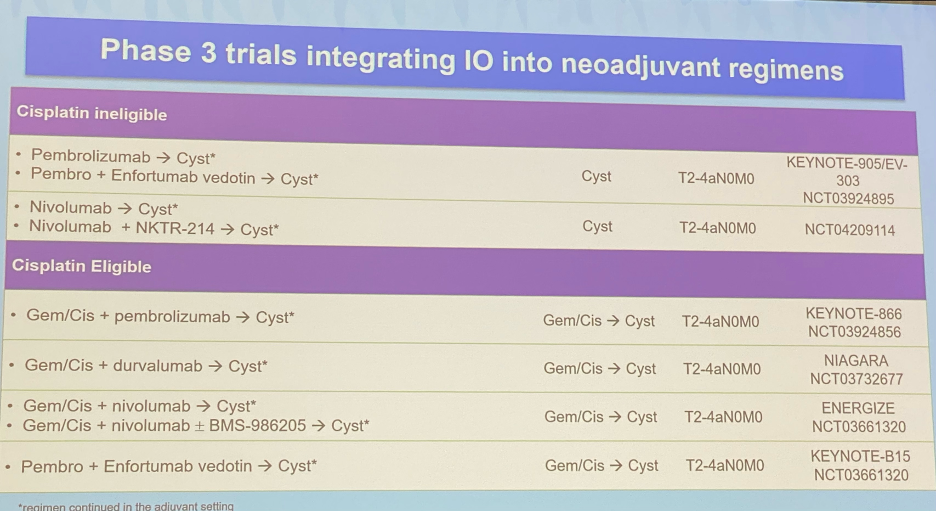
There are currently numerous phase 3 trials integrating immunotherapy agents into neoadjuvant regimens.
Dr. Galsky concluded with the following:
- Adjuvant IO has changed the landscape
- Neoadjuvant trials will impact adjuvant space
- ctDNA could impact paradigm
Presented By: Dr. Matthew Galsky, MD, Professor of Medicine, Director of Genitourinary Medical Oncology, Mount Sinai, New York, NY
Written By: Rashid Sayyid, MD, MSc – Urology Chief Resident, Augusta University/Medical College of Georgia, @rksayyid on Twitter during the 2022 Annual Meeting of the American Urological Association, New Orleans, LA, May 13 – 16, 2022
References:
- Grossman HB, Natale RB, Tangen CM, et al. Neoadjuvant chemotherapy plus cystectomy compared with cystectomy alone for locally advanced bladder cancer. N engl J Med. 2003;349(9):859-66.
- Bajorin DF, Witjes JA, Gschwend JE, et al. Adjuvant Nivolumab versus Placebo in Muscle-Invasive Urothelial Carcinoma. N Engl J Med. 2021;384(22):2102-2114.
- Bellmunt J, Hussain M, Gschwend JE, et al. Adjuvant atezolizumab versus observation in muscle-invasive urothelial carcinoma (IMvigor010): a multicentre, open-label, randomised, phase 3 trial. Lancet Oncol. 2021;22(4):525-37.