In the past, evidence was published that statins might actually cause cancer. This included evidence that statins cause cancer in rodents.1 Additionally, low dose statins were shown to increase PC aggressiveness.2 Statins affect PC through a multitude of mechanisms, including cell proliferation, cell cycle progression, cell differentiation, invasiveness, mitogenesis, AKT activation, NFkB activation, angiogenesis, MTOR activation, P53 modulation, pro-inflammatory cytokines, and antiapoptotic effect.
More recent evidence suggests that statins can decrease PSA levels, a risk of overall PC, a risk of advanced PC, a risk of biochemical recurrence (BCR), and metastasis, progression on androgen deprivation therapy (ADT), and risk of mortality: cancer-specific survival (CSS) and other cause mortality.
A recent publication demonstrated that out of 323,426 men aged >65 years who had a screening PSA test, statin users had a reduced probability of having an abnormal screening PSA result. 3 Another publication demonstrated that statins use was inversely correlated to PSA levels, and men using statins for more than 5 years had a 13% reduction in PSA levels.4
Individual studies had conflicting results, but the majority of studies showed no effect on statin use on risk of overall PC. The most recent meta-analysis reported a modest but significant 7% reduction in risk of overall PC, but >20% in the risk of advanced PC.5
Most of the evidence supports that statins selectively lower the risk of advanced PC. The health professional’s follow-up study of 34,989 men6 demonstrated no association between statin use and risk of overall PC. Significant risk reduction of 49% of advanced PC was noted, especially when PC is metastatic or lethal (61%). The risk of advanced disease was lower with longer statin use <5 years – 40%, and more than 5 years – 74%.
There is some evidence that statins also reduce the risk of BCR after radiotherapy. A systematic review and meta-analysis demonstrated 21% reduction in the risk of BCR after radiotherapy. 7 Statin use slows the progression of PC in men undergoing radiotherapy, possibly by sensitizing the cells to radiotherapy. Postoperative statin reduces the risk of BCR following radical prostatectomy as well by 36%. 8
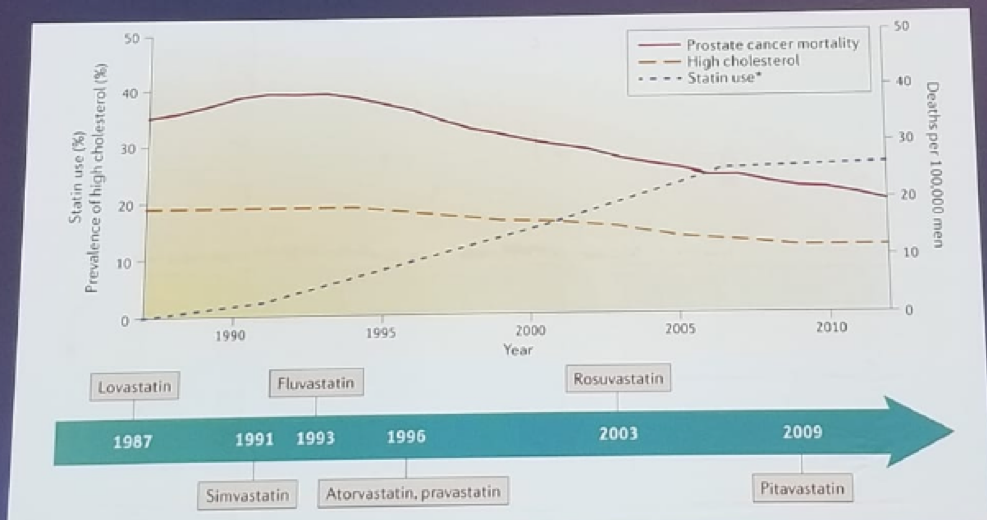
Statin use at the initiation of ADT prolongs time to castration-resistant PC (CRPC). It was demonstrated that men on statins had a much longer time to progression than men, not on statins (27.5 vs. 17.4 months). 9 Furthermore, post-diagnosis statin use was shown to decrease mortality in men with PC by 17%, and all-cause mortality by 19%.10 The decline in PC death rate in the USA in parallel to the market introduction of statins is shown in figure 1. It is clear from the presented evidence that statins have a protective role through the whole clinical course of PC.
Figure 1: The correlation between prostate cancer-specific death and the introduction of statins to the market
Leibovitch concluded his presentation by emphasizing the beneficial role that statins play in the entire course of PC. However, the evidence is still insufficient to recommend statins for all men with PC, and additional research is needed to establish whether statins have a genuine therapeutic potential in the management of PC.
References:
1. Newman and Hully: JAMA. 275:55-60, 1996
2. Car-Maldonado et al. Oncotarget 9 (2):1494-1504, 2017
3. Shi Y et al. Urology 84:1058-1065, 2014
4. Chang et al. J Clin Oncol 28:3951-3957, 2010
5. Bansal et al. Plos ONE; 7.e46691, 2012
6. Platz et al. J Natl Cancer Inst. 98(24):1819-25, 2006
7. Raval et al. Prostate Cancer and Prostatic Disease 19: 151-162, 2016
8. Allott et al. BJUI Int. 114:661-666, 2014
9. Harshman et al. JAMA Oncol 1(4): 495-504, 2015
10. Larsen et al. J Clin Oncol 35:3290-3297, 2017
Presented by: Ilan Leibovitch, MD, Meir Medical Center, Israel
Written by: Hanan Goldberg, MD, Urologic Oncology Fellow (SUO), University of Toronto, Princess Margaret Cancer Centre @GoldbergHanan at the 2018 FOIU 4th Friends of Israel Urological Symposium, July 3-5. 2018, Tel-Aviv, Israel