(UroToday.com) The American Urological Association's 2026 Annual Meeting, was host to the IP50: Bladder Cancer: Non-Invasive IV Session. Dr. Mukul Singhal presented interactive poster IP50-28: Quality care measures among patients with high-risk non-muscle invasive bladder cancer with papillary carcinoma or CIS receiving front-line BCG or other intravesical therapies.
Dr. Singhal began by noting that high-risk NMIBC is associated with a substantial disease burden and a high likelihood of recurrence and progression, necessitating intensive surveillance and repeated therapeutic interventions. He highlighted that patients often undergo multiple procedures and treatments, including TURBT, surveillance cystoscopy, and intravesical BCG therapy, all of which can significantly impact quality of life.
Given these challenges, organizations such as the NCCN and the AUA AQUA Registry have established several quality-of-care metrics aimed at optimizing management and improving outcomes in HR-NMIBC. However, Dr. Singhal emphasized that there remain limited real-world data evaluating adherence to these quality measures in the frontline treatment setting among patients with HR-NMIBC with CIS or papillary disease.
The investigators conducted a retrospective longitudinal study using SEER-Medicare data from 2007 through 2022, linking the National Cancer Institute SEER registry with Medicare claims data. The dataset included de-identified information compliant with HIPAA regulations.
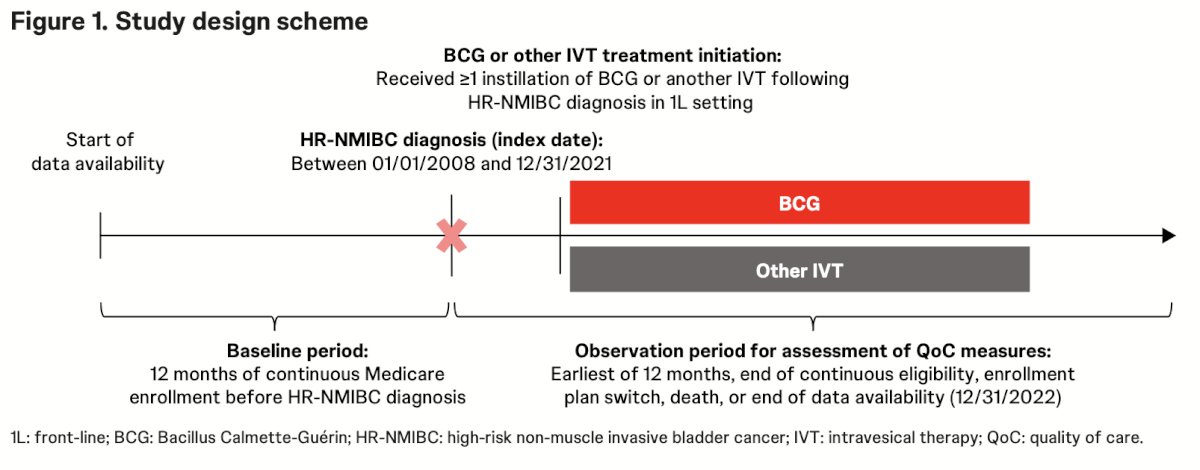
The study included patients aged 65 years or older with high-risk NMIBC with CIS or papillary carcinoma who initiated frontline treatment with BCG or other intravesical therapies, including mitomycin, gemcitabine, valrubicin, docetaxel, or epirubicin, without prior treatment for HR-NMIBC. The index date was defined as the date of HR-NMIBC diagnosis. Baseline characteristics were assessed during the 12 months prior to diagnosis, while patients were followed for up to 12 months after diagnosis or until disenrollment, plan switch, death, or end of available data. The study design is shown below:
Quality-of-care measures evaluated during follow-up included monitoring-related, treatment-related, and healthcare utilization metrics. Outcomes were analyzed descriptively using standard summary statistics for continuous and categorical variables.
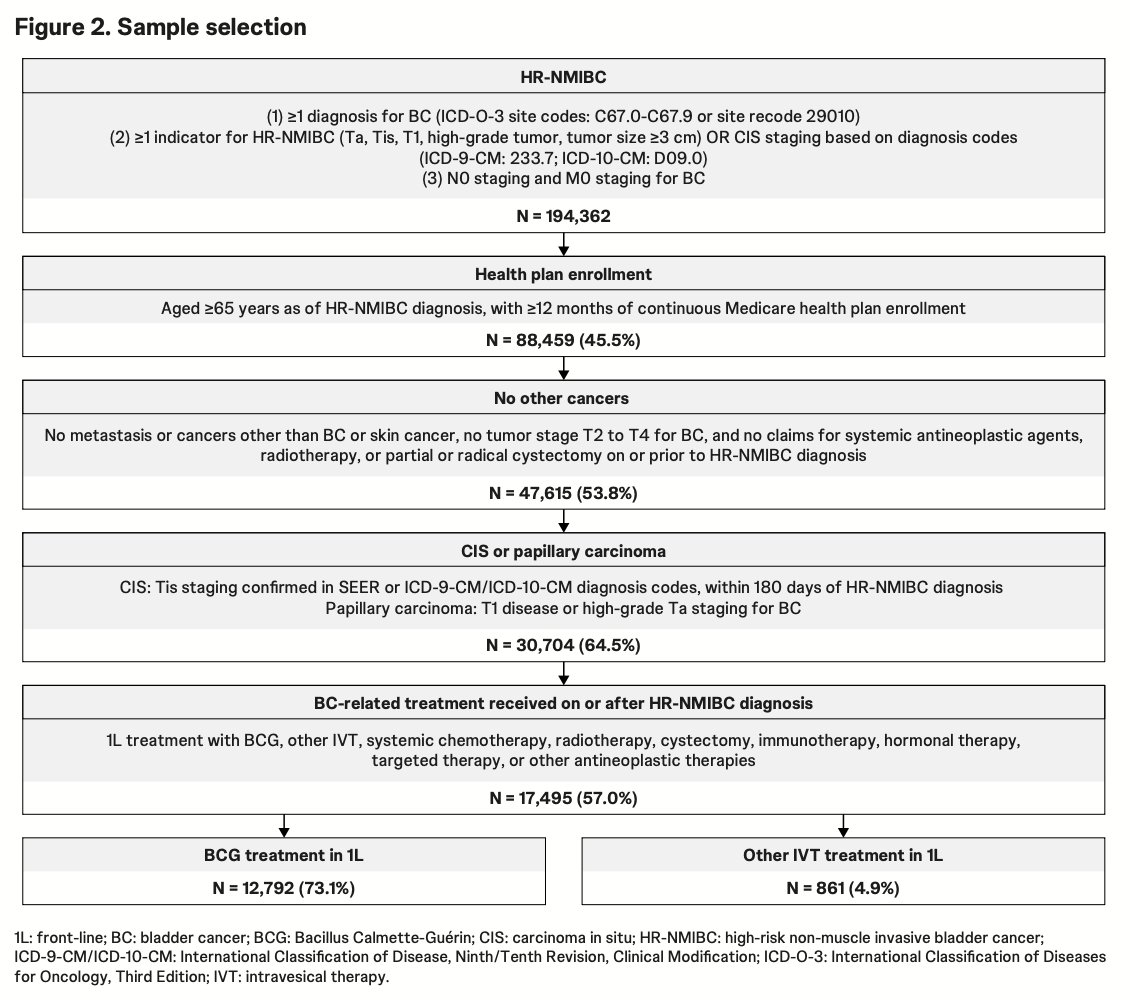
Dr. Singhal mentioned that from an initial cohort of 194,362 patients with HR-NMIBC identified in the SEER-Medicare database, sequential eligibility criteria including age ≥65 years, continuous Medicare enrollment, absence of metastatic or muscle-invasive disease, and confirmation of CIS or papillary carcinoma yielded a final treatment cohort of 17,495 patients. Among these patients, the majority received frontline BCG therapy (n=12,792; 73.1%), while a smaller proportion received other intravesical therapies (n=861; 4.9%).
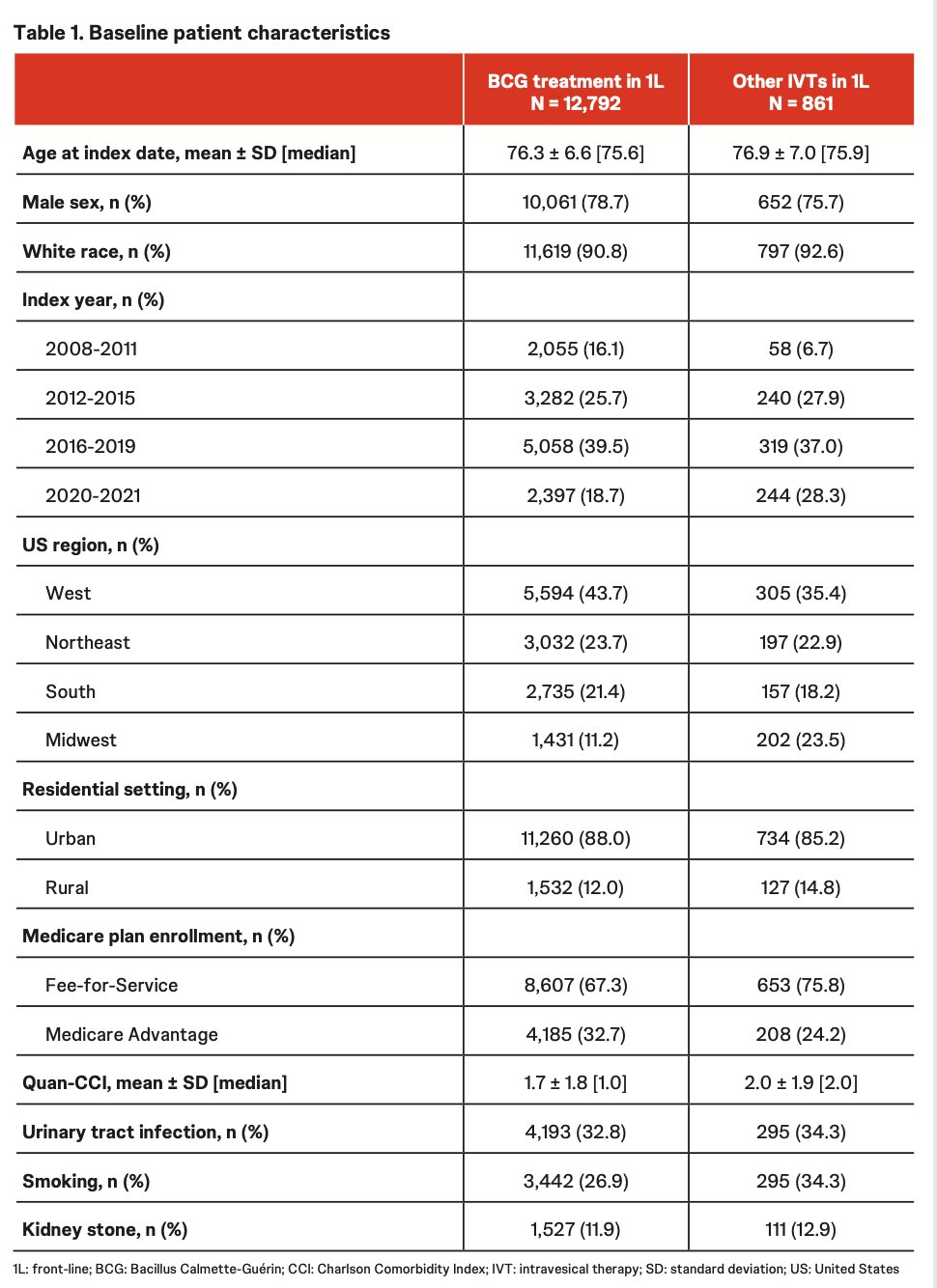
Among 17,495 patients initiating frontline treatment for HR-NMIBC, 12,792 (73%) received BCG, while 861 (5%) received other intravesical therapies. Patients in both cohorts were predominantly older, male, and White, with a mean age of approximately 76–77 years. Among patients treated with non-BCG intravesical therapies, the most commonly utilized agents were mitomycin (64%), followed by gemcitabine (25%) and gemcitabine plus docetaxel (5%) as shown in the table below.
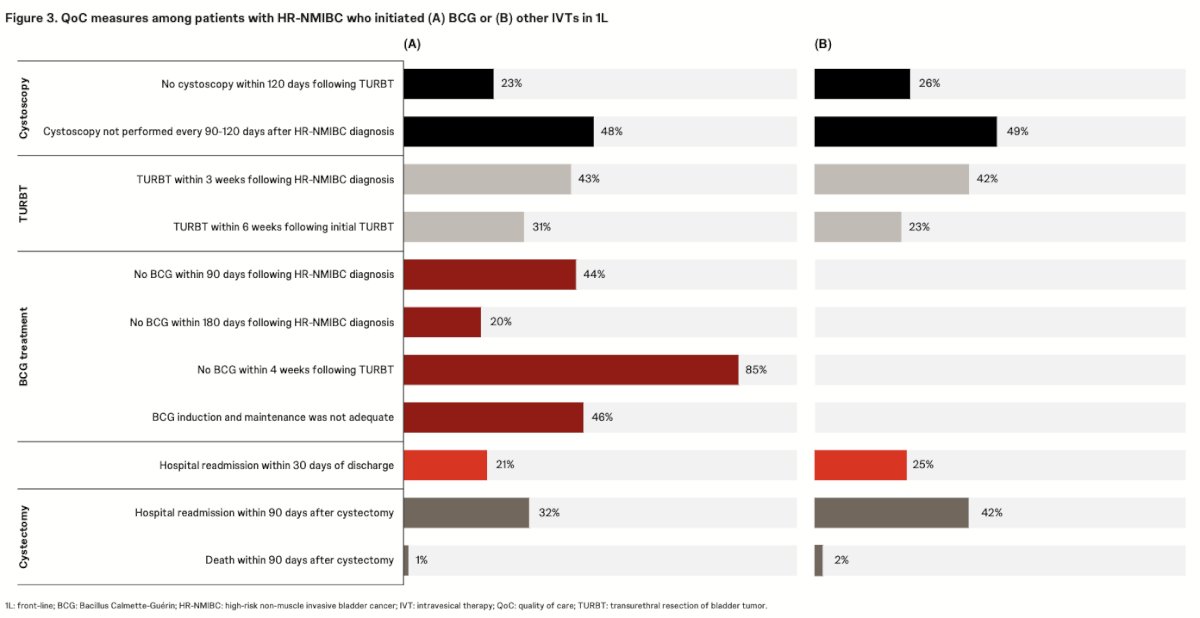
Quality-of-care metrics revealed substantial gaps in the management of patients with HR-NMIBC. Among patients treated with BCG, 44% did not initiate therapy within 90 days of diagnosis, while 46% failed to receive adequate induction or maintenance BCG. Additionally, nearly half of patients did not undergo surveillance cystoscopy at the recommended 90–120 day intervals, and only 31% underwent repeat TURBT within 6 weeks following the initial procedure. Hospital readmission rates were also notable, with 21% of hospitalized patients readmitted within 30 days and 32% of patients undergoing cystectomy readmitted within 90 days. Similar trends were observed among patients treated with other intravesical therapies, including suboptimal cystoscopic surveillance, low rates of repeat TURBT, and high post-hospitalization and post-cystectomy readmission rates.
Dr. Singhal acknowledged several important study limitations. As a retrospective claims-based analysis, the study is subject to inherent limitations including coding inaccuracies, incomplete documentation, and missing data, which may have led to misclassification of diagnoses, treatments, or quality-of-care measures. Additionally, the HR-NMIBC diagnosis date was based on the earliest available staging or diagnosis code within the database and, therefore, may not accurately reflect the true onset of disease, particularly for patients diagnosed before the available study period. Finally, because the analysis was restricted to the SEER-Medicare population, the findings may not be generalizable to younger patients or those without Medicare coverage.
Dr. Singhal concluded with the following key takeaways:
- Significant gaps in quality-of-care measures remain among Medicare-insured patients with HR-NMIBC receiving bladder-sparing frontline therapy for CIS or papillary carcinoma
- Deficiencies were observed across multiple domains, including treatment delivery, surveillance practices, and healthcare utilization
- Suboptimal adherence to recommended BCG administration and surveillance cystoscopy schedules highlights opportunities to improve real-world care
- Routine assessment and implementation of HR-NMIBC quality-of-care metrics may help reduce care gaps and improve patient outcomes in the frontline setting
Presented by: Mukul Singhal, PhD, Director, Real-world value & evidence, Genitourinary cancers, at J&J, PA, United States
Written by: Julian Chavarriaga, MD, Clinical Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health @chavarriagaj on Twitter during tthe American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.