(UroToday.com) The American Urological Association's 2025 Annual Meeting, between April 26 – 29, 2025, in Las Vegas, Nevada, was host to the Plenary Session: Paradigm-Shifting, Practice-Changing Clinical Trials in Urology. Dr. Felix Guerrero Ramos presented the first results from Cohort 4 of SunRISe-1, evaluating TAR-200 monotherapy in patients with bacillus Calmette-Guerin–unresponsive papillary disease–only high-risk non–muscle-invasive bladder cancer (NMIBC).
There remains a high unmet need in the BCG-unresponsive high-risk (HR) NMIBC space. Worldwide, more than 650,000 new cases of bladder cancer are diagnosed annually, with 75% of patients presenting with NMIBC, nearly half of whom are classified as high-risk.1 New treatments are urgently needed, as approximately 50% of patients with HR NMIBC experience recurrence or progression despite BCG, and radical cystectomy (RC) remains the standard of care. RC is a life-altering surgery associated with significant morbidity, substantial impact on quality of life, and a 90-day mortality rate ranging from 3% to 8%. Importantly, for patients with BCG-unresponsive HR NMIBC with papillary-only disease, there are currently no approved treatments, and investigational therapies report 12-month disease-free survival (DFS) or recurrence-free survival (RFS) rates between 44% and 55%.2,3
TAR-200 is a novel intravesical drug-releasing system that provides sustained delivery of gemcitabine and received FDA Breakthrough Therapy designation in 2023. Dr. Guerrero presented the first results of TAR-200 monotherapy (Cohort 4 of SunRISe-1) in the challenging population of patients with BCG-unresponsive high-risk NMIBC with papillary-only disease, highlighting the urgent need for new bladder-sparing alternatives to avoid RC.
A total of 52 patients with papillary-only disease were included in Cohort 4. Patients received TAR-200 treatment every three weeks for the first 24 weeks, followed by dosing every 12 weeks through week 96. The primary endpoint was disease-free survival (DFS), with key secondary endpoints including safety and durability of response. Response was assessed through quarterly cystoscopy, quarterly central cytology, local imaging every 24 weeks, and bladder biopsy by central assessment as clinically indicated. The study protocol did not allow for re-induction in nonresponders, in alignment with US FDA guidance. The study design is shown below.

The median age of patients was 71 years, with two-thirds being male. Of the cohort, 40% had T1 disease and 60% had Ta disease. Notably, 82.4% of patients declined surgery, highlighting the reluctance to undergo radical cystectomy (RC) at this early stage of disease, while 17.6% were deemed ineligible for surgery.

With a median follow-up of 12.8 months, the median DFS was not reached (95% CI, 12.1–not estimable). The DFS rates at 6 and 9 months were 85.3% and 81.1%, respectively. Overall, only 5.8% of patients (3 of 52) underwent radical cystectomy.

At 9 months, the DFS rates were 82.1% for patients with high-grade Ta disease and 79.4% for those with T1 disease. Regardless of T stage, TAR-200 demonstrated strong activity in this population.

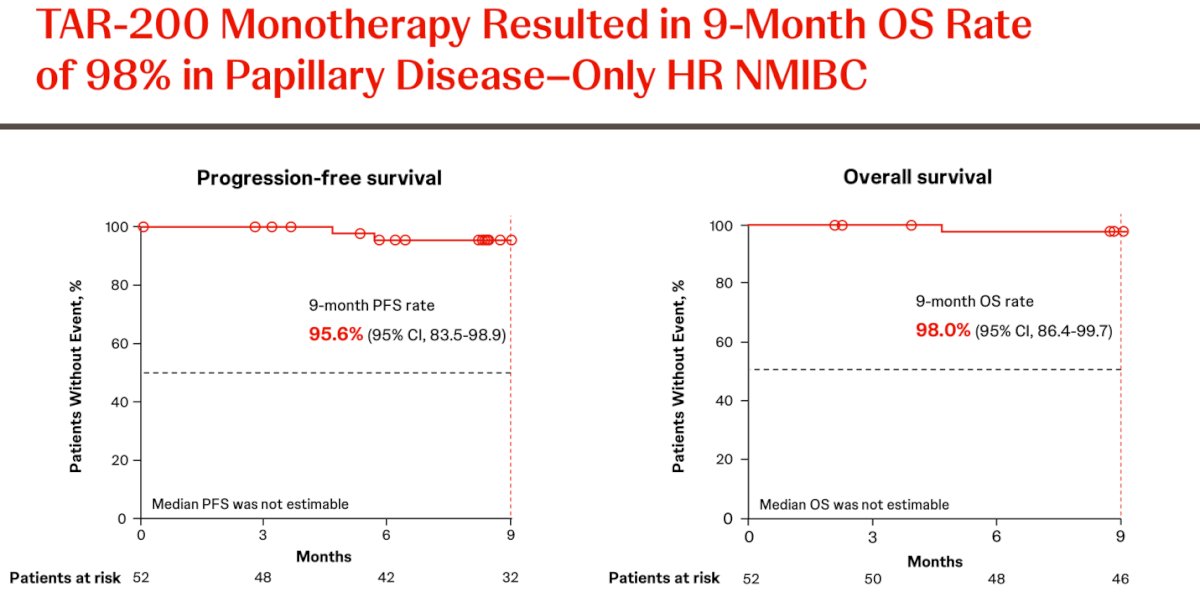
The progression-free survival (PFS) rate at 9 months was 95.6%, and although overall survival (OS) data were still immature, the OS rate was 98% at 9 months.
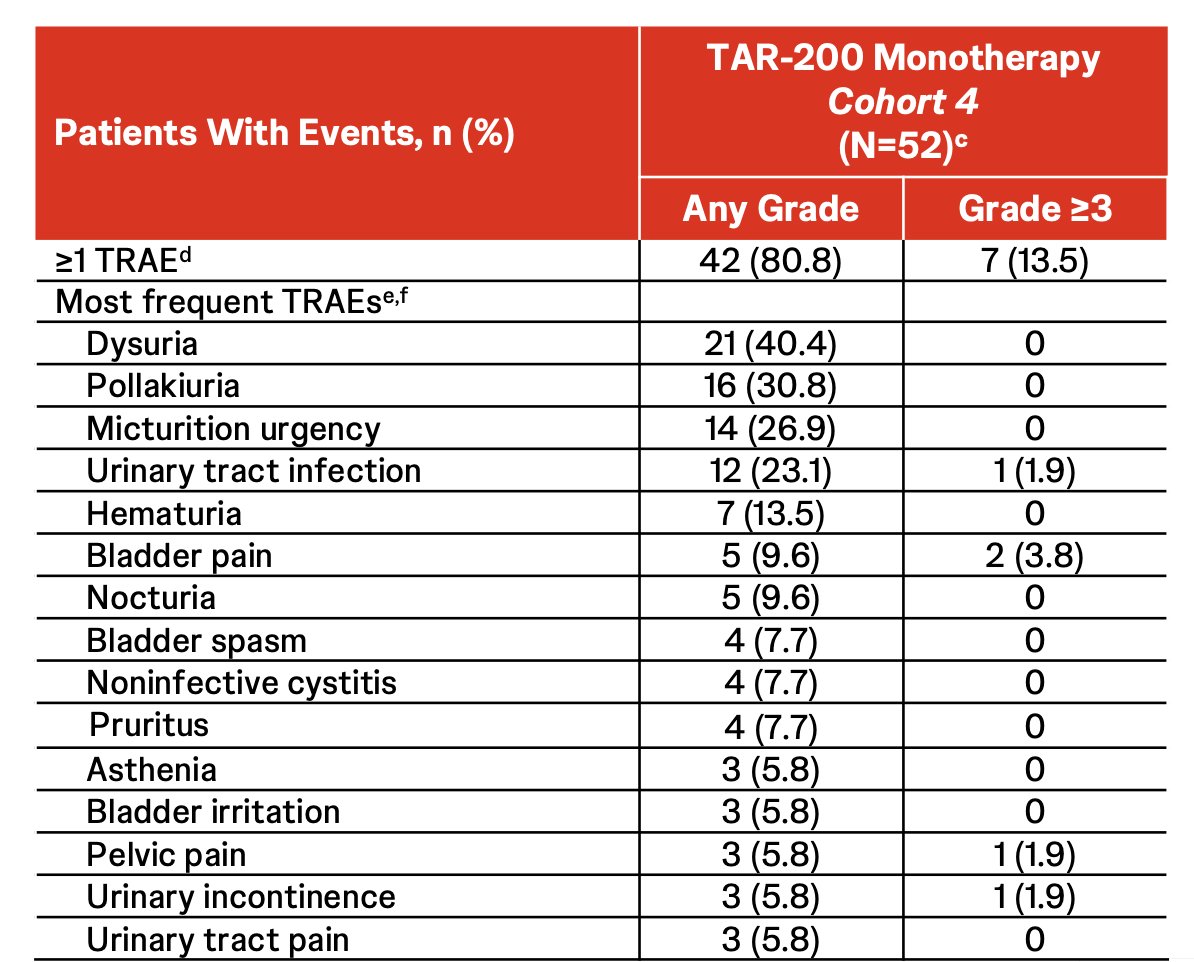
Most treatment-emergent adverse events (TEAEs) were grade 1 or 2, and the majority resolved quickly, with a median time to resolution of 3.7 weeks. Serious treatment-related adverse events (TRAEs) occurred in 3 patients (5.8%), and 4 patients (7.7%) discontinued treatment due to TRAEs. No treatment-related deaths were reported. The insertion success rate was 99.5% (387 of 389 insertions).
Dr. Guerrero concluded his presentation with the following key points:
- The first results of TAR-200 monotherapy in SunRISe-1 Cohort 4 showed impressive DFS rates in patients with BCG-unresponsive papillary-only high-risk NMIBC.
- DFS rates at 6 and 9 months were 85.3% and 81.1%, respectively.
- DFS rates remained consistently high across both high-grade Ta and T1 disease, reflecting the sustained tissue penetration achieved with TAR-200 via the iDRS.
- Only 5.8% of patients underwent subsequent radical cystectomy.
- High overall survival (OS) and progression-free survival (PFS) rates were observed at 9 months (98.0% and 95.6%, respectively).
- No new safety signals were detected; most TEAEs were grade 1 or 2 lower urinary tract symptoms, with low rates of serious TRAEs and few discontinuations due to TRAEs.
- The ongoing phase 3 SunRISe-5 study (NCT06211764), comparing TAR-200 monotherapy to intravesical chemotherapy in patients with BCG-unresponsive or BCG-experienced papillary-only high-risk NMIBC, will provide further evidence supporting TAR-200’s potential in this setting.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the American Urological Association's 2025 Annual Meeting, between April 26 – 29, 2025, in Las Vegas, NV.
Related content: SunRISe-1 Trial: Bladder-Sparing Results for BCG-Unresponsive Disease - Felix Guerrero-Ramos
- GLOBOCAN. Cancer Tomorrow (https://gco.iarc.fr/tomorrow/en/dataviz/isotype?cancers=30&single_unit=50000&years=2025).
- Babjuk M, et al. EAU Guidelines. Edn. Presented at the EAU Annual Congress, Madrid 2025. Eur Urol. 2022; 81: 75–94. ISBN 978-94-92671-29-5.
- AUA/SUO Guidelines. Non-Muscle Invasive Bladder Cancer. American Urological Association. Available at: https://www.auanet.org/guidelines-and-quality/guidelines/bladder-cancer-non-muscle-invasive-guideline. Accessed April 26, 2025.