(UroToday.com) The American Urological Association's 2025 Annual Meeting, in Las Vegas, Nevada, was host to the Plenary Session: Paradigm-Shifting, Practice-Changing Clinical Trials in Urology. Dr. Joseph Jacob discussed TAR-200 monotherapy in patients with bacillus Calmette-Guerin–unresponsive high-risk non–muscle-invasive bladder cancer carcinoma in situ: 1-year durability and patient-reported outcomes.
The standard of care for BCG-unresponsive high-risk NMIBC remains radical cystectomy (RC). However, RC is a life-changing operation associated with considerable morbidity, significant impact on quality of life, and a 90-day mortality risk of up to 8%. Many patients are either unable or unwilling to undergo RC.1
Real-world studies show that fewer than 20% of patients with high-risk NMIBC who recurred after BCG treatment ultimately undergo RC. Treatment options for BCG-unresponsive high-risk NMIBC, particularly CIS, remain limited. Current US FDA-approved therapies report overall complete response (CR) rates of 41% with pembrolizumab, 51% with nadofaragene firadenovec, and 62% with nogapendekin alfa inbakicept combined with BCG.2
TAR-200 is a novel intravesical drug-releasing system designed to provide sustained delivery of gemcitabine directly into the bladder. It has been granted FDA Breakthrough Therapy Designation. TAR-200 is placed using a urinary placement catheter in a brief, in-office procedure, offering a minimally invasive option for patients as illustrated below.

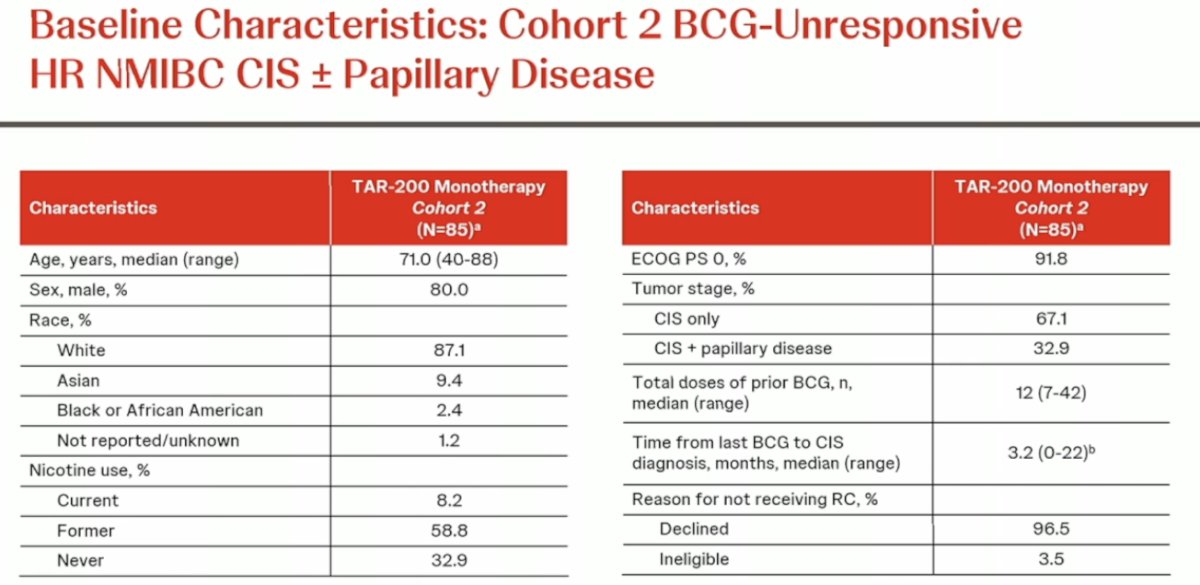
Dr. Jacob presented results from Cohort 2 of the SunRISe-1 trial, which included 85 patients who received TAR-200 every three weeks (Q3W, indwelling) for the first 24 weeks, followed by administration every 12 weeks (Q12W) through week 96. The primary endpoint was the overall complete response (CR) rate, with key secondary endpoints including duration of response, overall survival, safety, tolerability, and health-related quality of life (HRQOL). Notably, patients underwent quarterly cystoscopy, cytology, and mandated bladder biopsies at weeks 24 and 48. Patients who showed consistent disease progression while on treatment were required to be removed from the treatment arm. Study design is shown below.

Dr. Jacob highlighted that approximately two-thirds of patients had CIS-only disease, while one-third had CIS with papillary tumors. Notably, 96.5% of patients declined cystectomy, with only 3.5% deemed ineligible for surgery. This cohort represented a highly motivated group of patients seeking bladder-sparing therapy (BST).
Cohort 2 of the SunRISe-1 trial demonstrated the highest complete response (CR) rate reported to date. The overall CR rate was 82.4%, and the CR rate from treatment initiation at 12 months was 45.9%. Responses occurred rapidly following TAR-200 monotherapy, with a median time to response of 2.8 months (range, 2.1–8.3 months). Notably, 95.7% (67 of 70) of complete responses were achieved by the first disease assessment at three months.

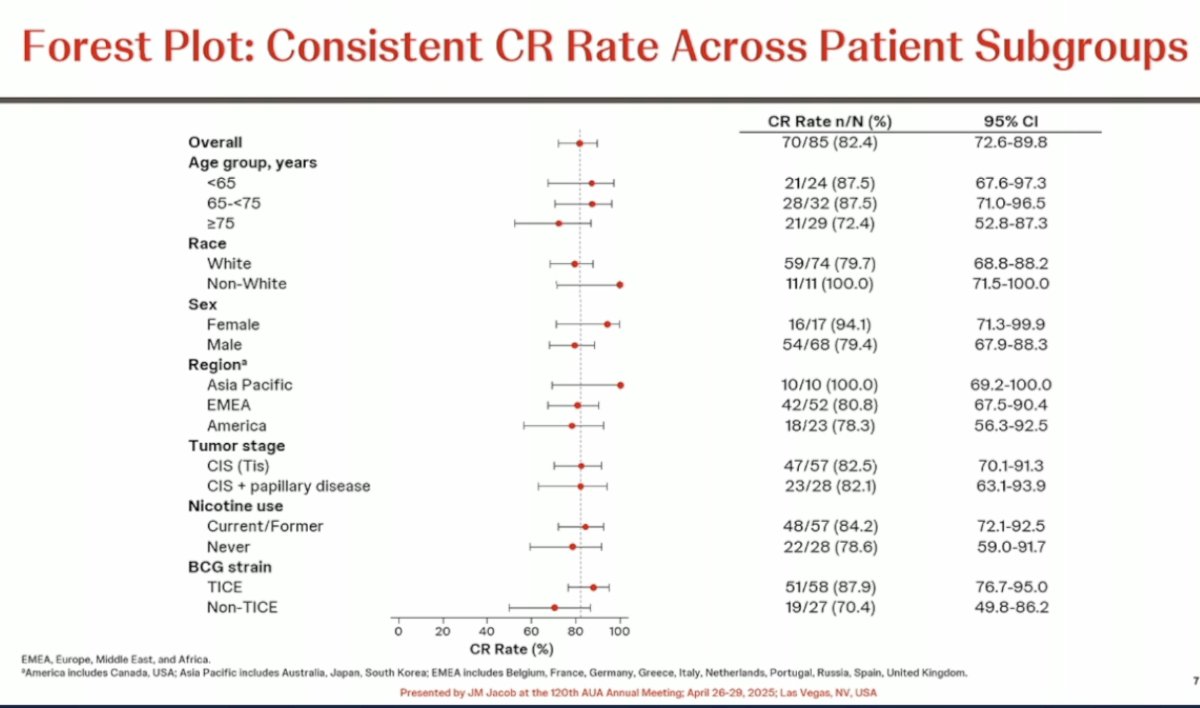
The investigators observed a consistent complete response (CR) rate across all patient subgroups, as demonstrated in the forest plot below.
Notably, 52.9% of responses lasted for at least 12 months, and 47.1% of responses remain ongoing. Among the 11 patients who completed two years of treatment, nine patients continued to maintain their response.

Durable responses were observed with TAR-200 monotherapy. The estimated 12-month duration of response (DOR) rate was 56.2%. Another way to assess durability is by noting that the curve flattens around the 12-month mark, which is a favorable predictor of long-term response. The median DOR was 25.8 months. Additionally, 86.6% of patients remained cystectomy-free at one year.

Regarding quality of life (QoL), patients maintained stable QoL while on TAR-200 treatment. Mean EORTC QLQ-C30 Global Health Status (GHS) scores were 75.0 (SD, 16.7) and physical functioning (PF) scores were 86.2 (SD, 17.3) at baseline, and both remained stable throughout treatment.

Dr. Jacob highlighted the table below, which summarizes outcomes for TAR-200 on the left and compares them to other available treatment options on the right. Notably, among all patients who received TAR-200 therapy, 44% had a response that lasted for at least one year.

Most treatment-emergent adverse events (TEAEs) were grade 1 or 2 and resolved after a median of 3.1 weeks. Impressively, there was a 99% insertion success rate, with urologists reporting no significant difficulties placing the devices. Serious treatment-related adverse events (TRAEs) occurred in 5 patients (5.9%), and only 3 patients (3.5%) discontinued treatment due to TRAEs. No treatment-related deaths were reported.

Dr. Jacob concluded his presentation with the following take-home messages:
- TAR-200 monotherapy provides the highest single-agent CR rate (82.4%) reported to date in patients with BCG-unresponsive high-risk NMIBC.
- Onset of response was rapid, with 95.7% of CRs achieved at the first disease assessment, without the need for reinduction.
- TAR-200 monotherapy responses were durable, with a median duration of response of 25.8 months and 52.9% of responses lasting for ≥1 year.
- Overall health status and physical functioning were maintained while on TAR-200 treatment.
- TAR-200 was well tolerated, with serious treatment-related adverse events (TRAEs) and TRAEs leading to discontinuation being rare.
- TAR-200 is currently under review by the US FDA following submission of a New Drug Application.
Presented by: Joseph Jacob, MD, MCR, Urologic Oncologist and Associate Professor of Urology at Upstate Cancer Center, Syracuse, NY.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 American Urological Association (AUA) annual meeting held in Las Vegas, NV, Saturday, April 26 - Tuesday, April 29, 2025
References:
- Maibom SL, Joensen UN, Poulsen AM, Kehlet H, Brasso K, Røder MA. Short-term morbidity and mortality following radical cystectomy: a systematic review. BMJ Open. 2021 Apr 14;11(4):e043266. doi: 10.1136/bmjopen-2020-043266. PMID: 33853799; PMCID: PMC8054090.
- Boorjian SA, Alemozaffar M, Konety BR, et al. Intravesical nadofaragene firadenovec gene therapy for BCG-unresponsive non-muscle-invasive bladder cancer: a single-arm, open-label, repeat-dose clinical trial. Lancet Oncol. 2021;22(1):107–117.