In this study, Dr. Albers and colleagues from Germany assess the role of RPLND for men with low volume Stage IIA/B seminoma without planned adjuvant therapy. Patients included had clinical stage IIA/B seminoma, <5 cm nodal disease (in transverse diameter), had a recurrence during surveillance or presented with stage II A/B disease or had a recurrence following carbo x 1 adjuvant therapy, and had HCG < 5 IU/L. They were treated with either open or robotic RPLND – however, it was a unilateral template procedure.
This is an interim analysis of an ongoing clinical trial. This was a two-part study, starting with a 9 patient feasibility pilot study which has then been expanded to a phase II study. To date, an additional 14 patients from 3/2016 to 1/2019 within the prospective phase II trial were accrued. Since May 2014, that brings the total to 23 patients with seminomatous GCT that have been included in both studies.
There was a planned interim analysis at 1.5 years to ensure that recurrence rates did not exceed a pre-specified cutoff of 30%.
In his presentation, he presented the data as two separate studies rather than as one combined study. He first focused on the 14 patients in the phase II study. The median age of this group was 36.5 years (range 28-49). Of these patients, 6 were stage IIA and 8 were stage IIB – most (10) had recurrences on surveillance, but 4 presented with metastatic disease and 2 had recurrences following adjuvant carbo. Median tumor size was 1.8 cm. In terms of approach, 7 had open and 7 had robotic RPLND to date. 8 patients had ipsilateral nerve sparing.
- As a comment about overstaging, 1 patient actually had no disease on final pathology
In terms of oncologic outcomes, after a mean follow-up is 12.5 month (range 3-25 months), 10/14 patients (71%) are free of recurrence. 4/14 (29%) developed a recurrence – details are found below:
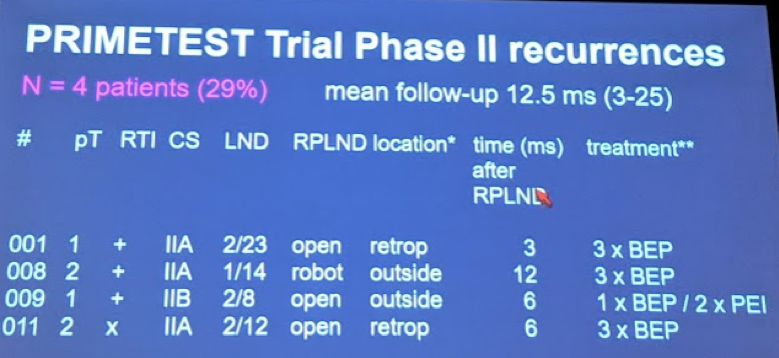
Mean time to recurrence was 6.8 months.
Interesting, 3 of those recurrences were in patients with IIA disease. The surgical approach was not associated with recurrence rates.
All patients with recurrences were cured with salvage chemotherapy.
*None of the recurrences occurred in the surgical field. However, 2 patients had retroperitoneal recurrences
He briefly reviewed the data from the 9 patients in the pilot study. In those 9 patients, 3 patients developed recurrences – interestingly, those 3 patients all had IIB and IIC disease (none had IIA disease). 7 patients had open RPLND and 1 patient had a robotic RPLND. One patient after DaVinci RPLND developed a ureteral stricture requiring ileal substitution. All patients with recurrence were treated with salvage chemotherapy and have done well.
Ultimately, however, the trial recruitment is planned for 30 men and was designed to exclude a > 30% recurrence to standard treatment. They still have 7 more patients in the phase II trial to recruit prior to meeting their endpoint. They plan to expand to a multicenter recruitment in Germany to help increase patient volume.
Based on these interim results, they justified continuing the study to completion. However, the caveat is that primary RPLND should only be performed within clinical trials and in high volume referral centers.
Importantly, a similar study entitled SEMS is underway in the United States. They are hoping to combine data with Dr. Daneshmand and the SEMS trial for a joint analysis.
Presented by: Peter Albers, MD, Professor of Urology, Department of Urology, Düsseldorf University, Germany
Written by: Thenappan Chandrasekar, MD (Clinical Instructor, Thomas Jefferson University) (twitter: @tchandra_uromd, @JEFFUrology) at the 2019 American Society of Clinical Oncology Genitourinary Cancers Symposium, (ASCO GU) #GU19, February 14-16, 2019 - San Francisco, CA