In our recently published work,1 we retrospectively analyzed the benefits and harms of multiple diagnostic pathways as proposed by Schoots et al.2 and Padhani et al.3 We reviewed a population of 499 biopsy-naïve men with suspicious MRI scans who were referred to our center for an MRI+US fusion biopsy between June/2016 and November/2019. We carefully analyzed the yields for clinically significant cancers (ISUP grade >1), indolent cancers and no cancers. We also analyzed their potential for biopsy avoidance.
In general, we found that any pathway that included MRI outperformed the systematic biopsies in all the measured outcomes, underscoring the value of MRI as the centerpiece for patient biopsy decisions. By employing a novel analytical method called ‘decision curve analysis’,4 we were able to analyze the balance of the benefits and harms (net-benefit) over a wide range of clinical scenarios. We can thus assess the net benefit of each pathway for men who are cancer averse versus those who are biopsy averse. We found that the ‘risk-based MRI-directed pathway’ was the one that resulted in the highest net benefit for all reasonable clinical scenarios.

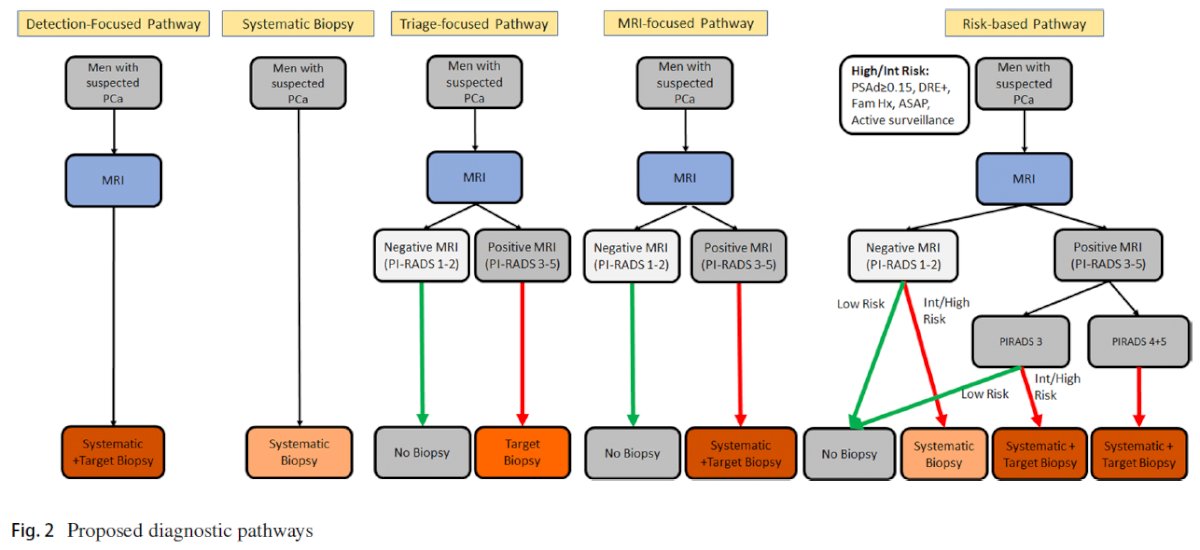
So, what is the risk-based pathway?
The risk-based MRI-directed pathway proposes an additional layer of clinical assessments and laboratory tests to further risk-stratify the MRI results. For instance, patients with a negative MRI or with an equivocal MRI at low-clinical risk can avoid an immediate biopsy. These men are clinically followed through a ‘safety net’ framework. Everyone else would need a biopsy because of an elevated risk of clinically significant cancer.
The criteria that we used for clinical risk assessments in men presenting for the first time were the prostate volume normalized PSA (PSA-density) of ≥0.15 ng/ml2, an abnormal digital rectal examination, and a family history of prostate cancer. We recognize that other clinical risk criteria may be helpful, but we used these criteria because they are readily available to radiologists and urologists at the time of clinical decisions.
Overall, we concluded that diagnostic pathways that use prostate MRI data combined with guided biopsies showed higher rates of detection of clinically significant prostate cancers, also enabling the reduction of indolent cancers that are unlikely to cause harm, while at the same time enabling biopsy avoidance for many men. Furthermore, when comparing the MRI pathways, the risk-based pathway had the best performance across a wide range of clinically relevant scenarios. Although our results are encouraging, they are based on look-back analysis and are therefore not directly practice-changing now. However, these results should be taken note of by urological guideline committees, who should lean towards recommending a “risk-based” MRI-directed biopsy decision approach.
Written by: Leonardo K. Bittencourt,1 Anwar R. Padhani,2 Clare M. Tempany,3 Ivo G. Schoots4
- University Hospitals and Case Western Reserve University, Cleveland, OH, USA
- Paul Strickland Scanner Centre, Mount Vernon Hospital, Northwood, UK
- Brigham and Women's Hospital, Harvard Medical School, Boston, MA, USA.
- Erasmus University Medical Center, Rotterdam, and Netherlands Cancer Institute, Amsterdam, The Netherlands.
References:
- Bittencourt, L.K., Guricova, K., Zucker, I. et al. Risk-based MRI-directed diagnostic pathway outperforms non-risk-based pathways in suspected prostate cancer biopsy-naïve men: a large cohort validation study. Eur Radiol (2022). https://doi.org/10.1007/s00330-021-08407-6.
- Schoots I., Padhani A., Rouvière O., et al. "Analysis of Magnetic Resonance Imaging–directed Biopsy Strategies for Changing the Paradigm of Prostate Cancer Diagnosis." European Urology Oncology. Volume 3, Issue 1. 2020. 32-41. ISSN 2588-9311.
- Padhani A., Barentsz J., Villeirs G. et al. "PI-RADS Steering Committee: The PI-RADS Multiparametric MRI and MRI-directed Biopsy Pathway." Weinreb Radiology. 2019. 292:2, 464-474
- Vickers A., Calster B., Steyerberg E. et al. "Net benefit approaches to the evaluation of prediction models, molecular markers, and diagnostic tests." BMJ. 2016. 352:i6.
Read the Abstract