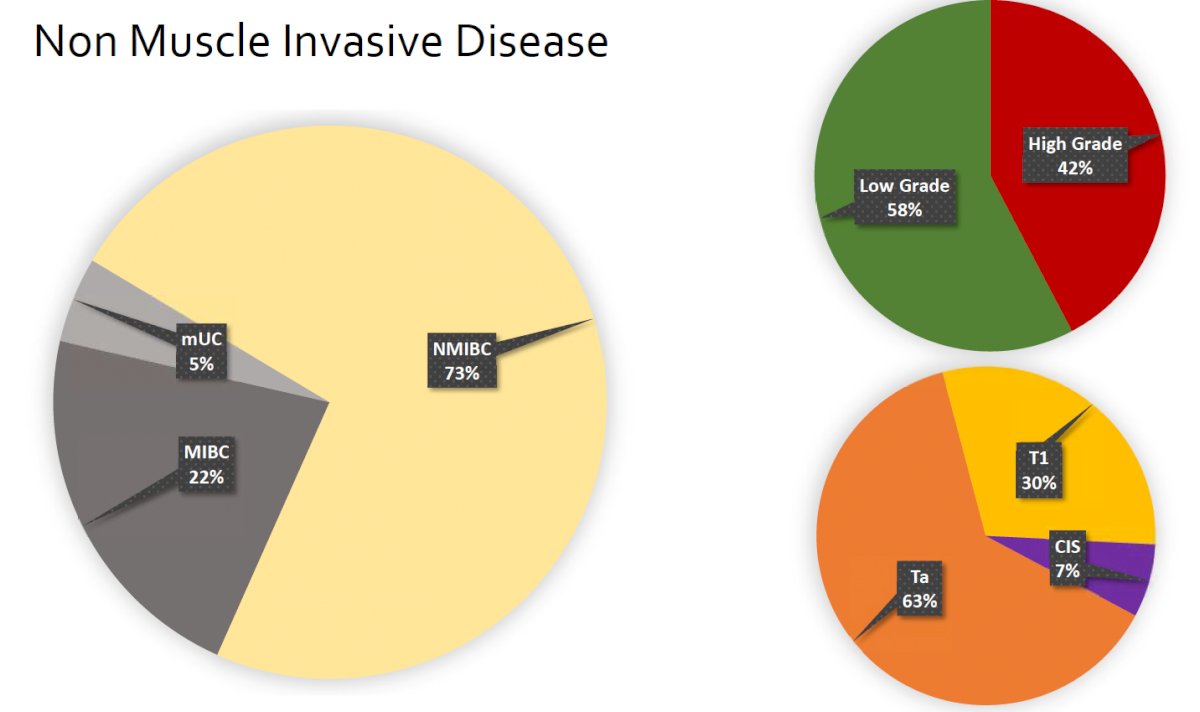
(UroToday.com) The 2022 Society of Urologic Oncology annual meeting featured a bladder cancer session, including a presentation by Dr. Ashish Kamat discussing new definitions for intermediate risk non-muscle invasive bladder cancer. Dr. Kamat started his presentation by highlighting that non-muscle invasive bladder cancer accounts for 73% of all bladder cancer diagnoses, including 42% high-grade disease and most commonly high-grade Ta (63%) non-muscle invasive bladder cancer:
With regards to intermediate risk non-muscle invasive bladder cancer, the AUA/SUO defines intermediate risk disease as any of the following:
- Recurrence within 1-year, low-grade Ta
- Solitary low-grade Ta > 3 cm
- Multifocal low-grade Ta
- High-grade Ta, <= 3 cm
- Low-grade T1 disease
Furthermore, the International Bladder Cancer Group (2011, 2014) defined intermediate risk disease as multiple or recurrent low-grade tumors. Prior to 2021, the EAU defined intermediate risk non-muscle invasive bladder cancer as “all tumors not defined in the two adjacent categories (low-grade and high-grade disease).” Since 2021, the EAU has provided additional granularity, noting that intermediate risk disease is defined as patients without CIS who are not included in either the low, high or very high-risk groups. Additional clinical risk factors include (i) age > 70 years of age, (ii) multiple papillary tumors, and (iii) tumors >3 cm in diameter. To further summarize, Dr. Kamat notes that the following Ta high-grade tumors are classified as intermediate risk non-muscle invasive bladder cancer:
- AUA: < 3cm, primary, solitary
- EAU: Could be >3 cm, could be multifocal, could be recurrent
- International Bladder Cancer Group: All high-grade are high-risk
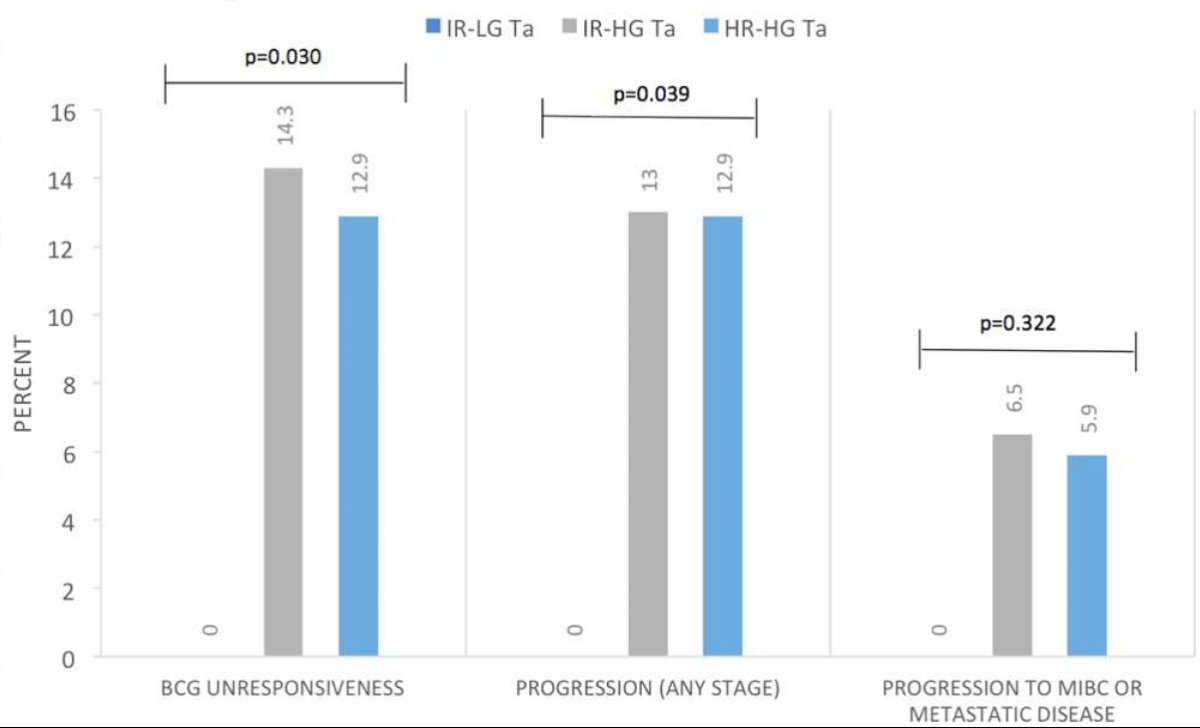
According to Dr. Kamat and work done by his group, all high-grade Ta tumors should be classified as high-risk based on evidence to their response to BCG.1 Among patients treated at the MD Anderson Cancer Center, BCG unresponsiveness developed in 13% of high-risk high-grade Ta tumors and 14% of intermediate-risk high-grade Ta tumors compared to 0.0% of intermediate-risk low grade Ta tumors (p=0.003). While no patients with intermediate-risk low grade Ta tumors progressed, progression rates were similar in high-risk high-grade Ta tumors and intermediate-risk high-grade Ta tumors (≥T2: 5.9% and 6.5%; T1: 13% and 13%, respectively):
As such, Dr. Kamat emphasized that Ta high-grade tumors should be classified as high-risk:
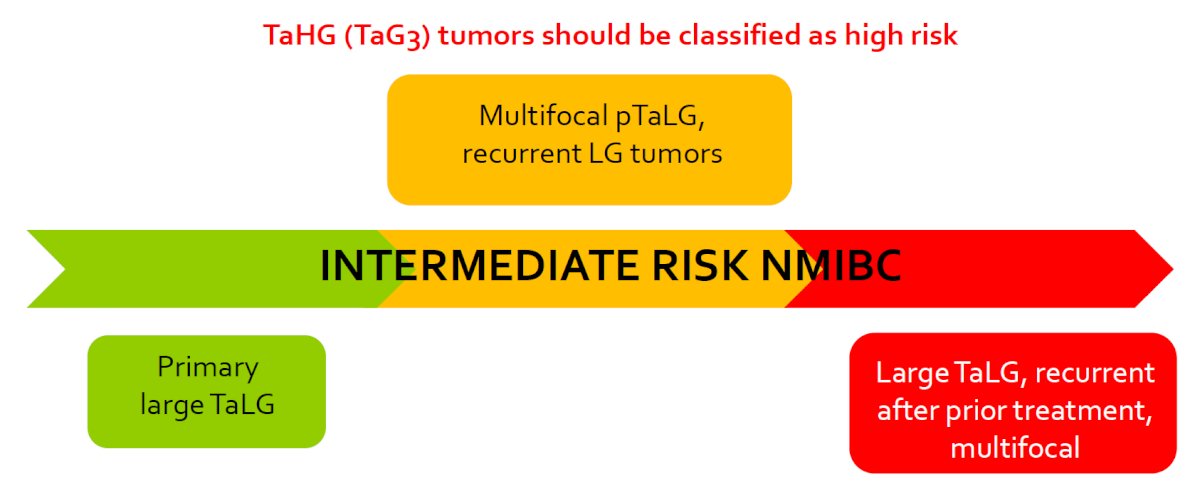
Recent work from the International Bladder Cancer Group has provided updated definitions and management recommendations for the treatment of intermediate risk non-muscle invasive bladder cancer.2 Among intermediate risk (low-grade tumors), the following risk factors should be assessed:
- Tumor size >3 cm
- Multiple tumors
- Early recurrence (<1 year)
- Frequent recurrence (>1/year)
- Failure of previous intravesical treatment
Those patients with none of the above risk factors, should be treated similarly to those with low-risk disease (no additional treatment). Patients with 1-2 risk factors, they should be treated as intermediate risk disease and thus treated with additional adjuvant induction intravesical chemotherapy (or BCG if prior chemotherapy has been used). For patients with >= 3 risk factors, they should be treated as high risk disease with BCG/chemotherapy for at least 1 year, with maintenance therapy:

Based on these definitions, the following 5-year recurrence and progression rates have been observed:
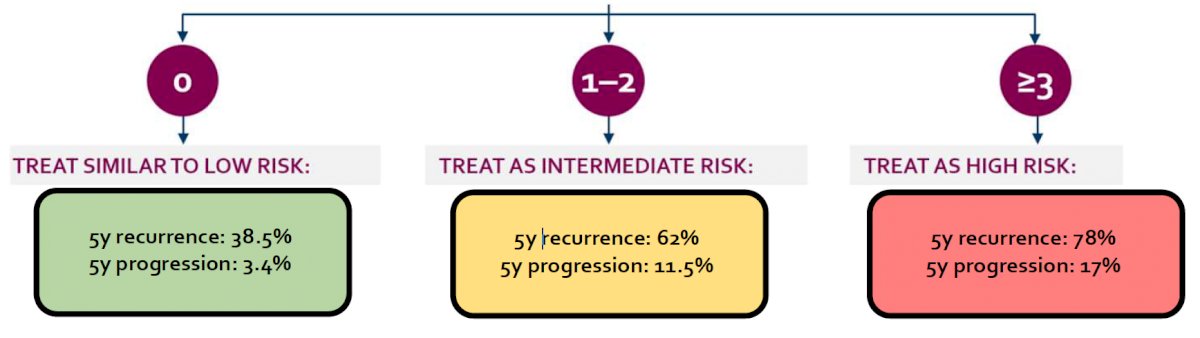
Dr. Kamat additionally emphasized that those patients classified as high-risk could also include tumors that are high-grade Ta solitary, non-recurrent, and <3 cm.
Dr. Kamat concluded his presentation by discussing new definitions for intermediate risk non-muscle invasive bladder cancer with the following take home messages, highlighting that intermediate risk non-muscle invasive bladder cancer should be considered as a spectrum:
- Standardization in defining intermediate risk non-muscle invasive bladder cancer is required
- Risk stratification is necessary to guide treatment decisions
- Covariate adjustments using prognostic factors leads to optimal trial design
Presented by: Ashish Kamat, MD, MBBS, The University of Texas MD Anderson Cancer Center, Houston, TX
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, @zklaassen_md on Twitter during the 23rd Annual Meeting of the Society of Urologic Oncology (SUO), Nov 30 – Dec 2, 2022. San Diego, CA
References:
- Bree KK, Hensley PJ, Lobo N, et al. All High-Grade Ta Tumors Should be Classified as High Risk: Bacillus Calmette-Guerin Response in High-Grade Ta Tumors. J Urol. 2022 Aug;208(2):284-291.
- Tan WS, Steinberg G, Witjes JA, et al. Intermediate-risk non-muscle invasive bladder cancer: Updated Consensus Definition and Management Recommendations from the International Bladder Cancer Group. Eur Urol Onc. 2022 Oct;5(5):505-516.