(UroToday.com) The Society of Urologic Oncology (SUO) 2021 annual meeting in Orlando, FL included an overview of molecular classification of upper tract urothelial carcinoma (UTUC), presented by Dr. Jonathan Coleman, MD, Associate Professor at the Memorial Sloan Kettering Cancer Center in New York, NY.
Dr. Coleman began his presentation by presenting data on next generation sequencing (NGS) of treatment naive non-muscle invasive bladder cancers (NMIBC) from 105 patients that demonstrated that TERT promoter mutations (73%) and chromatin-modifying gene alterations (69%) were highly prevalent across NMIBC grades and stages. ERBB2 or FGFR3 alterations were present in 57% of high-grade NMIBC tumors in a mutually exclusive pattern. DNA damage repair (DDR) gene alterations were seen in 30% of high grade NMIBC tumors, a rate similar to muscle invasive bladder cancer (MIBC), and were associated with a comparatively high mutational burden.1 Various MIBC transcriptional subtypes including luminal-papillary, luminal-infiltrated, luminal, basal/squamous, and neuronal have been defined. The questions thus become:
- How do these compare to upper tract disease?
- What is their clinical significance?
- What are the appropriate treatment strategies?
Dr. Coleman went on to elaborate on the distinguishing biologic features of UTUC. UTUC is predominantly high-grade at presentation (65% versus 40% in bladder cancer) and variant subtypes are rare in this disease (6.5% versus 20% in bladder cancer). There are also known causative factors that predominate for UTUC:
- Aristolochic acid (Birthwort)
- Lynch syndrome
- Mismatch repair genes (MMR)
- MLH1, MSH2, MSH6, PMS1, PMS 2, EPCAM, MLH3
- Detectable by immunohistochemistry (MMR/MSI)
- Reflex testing of all UTUC is recommended (reported prevalence of 9-12%)
While genomic studies may provide insight into biologic differences, the caveat remains that UTUC studies are dependent on retrospective, small cohort, institutional databases with rare outcomes and potential biases, whereas as bladder cancer studies are based on large genomic databases such as the TCGA. Case selection with UTUC studies is a key element to consider as concomitant or metachronous cancers act as confounders and cross contamination between upper and lower tracts remains a concern. Thus, Dr. Coleman believes that an adequate comparison requires patients with no prior history of concomitant or metachronous crossover disease.
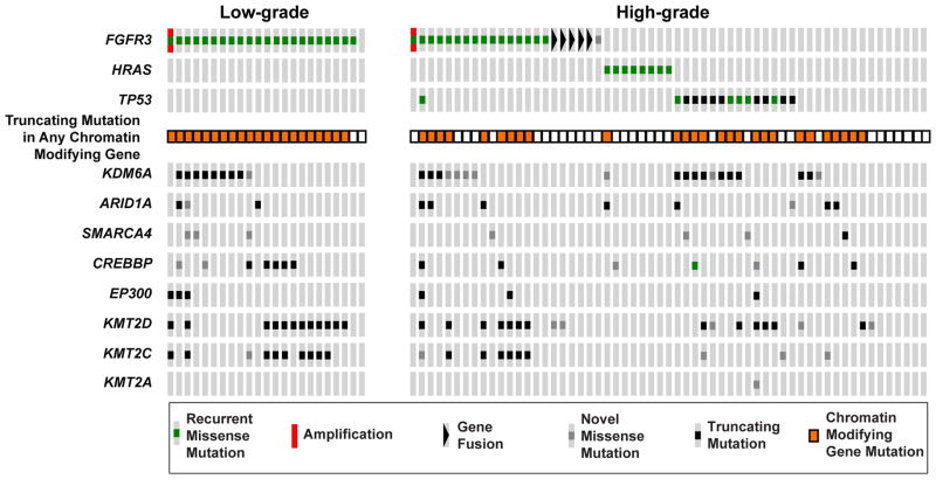
The genomic landscape of pure UTUC was described by Sfakianos et al. in 2015 whereby tumor and germline DNA from 83 patients with UTUC and 102 patients with bladder cancer were analyzed using NGS to identify somatic mutations and copy number alterations. FGFR3 (35.6% vs 21.6%; p=0.065), HRAS (13.6% vs 1.0%; p=0.001), and CDKN2B (15.3% vs 3.9%; p=0.016) were altered more commonly in high-grade UTUC compared to bladder cancer. Conversely, TP53 (25.4% vs 57.8%; p<0.001), RB1 (0.0% vs 18.6%; p<0.001), and ARID1A (13.6% vs 27.5%; p=0.050) were mutated less frequently in high-grade UTUC.2 These results imply a subtle biologic difference between UTUC and bladder cancer reflected in their clinical behavior. 

The same study used OncoPrint to compare mutations in FGFR3, HRAS, and TP53 between low-grade and high-grade UTUC. FGFR3 mutations were detected in 95.6% of low-grade tumors. Notably, a pattern of mutual exclusivity between FGFR3, HRAS, and TP53 was seen in the high-grade tumors. Alterations in chromatin-modifying genes were common in both the low-grade and high-grade tumors [2].
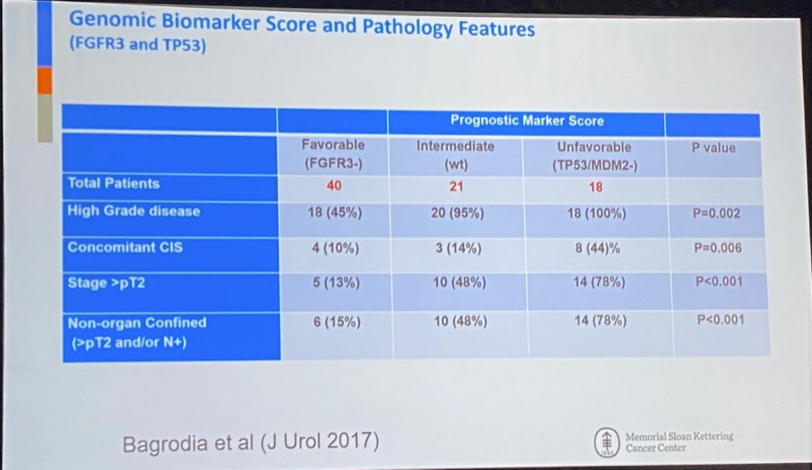
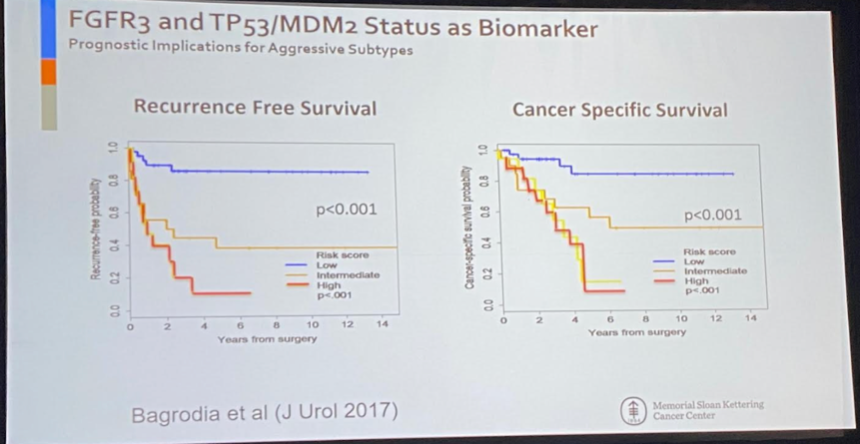
FGFR3 and TP53 have subsequently been used as genomic biomarker scores and were correlated with pathology features as demonstrated in the images below, with FGFR3- patients having more favorable pathologic features compared to TP53/MDM2- patients and superior recurrence free and cancer-specific survivals.
The Drop Down hypothesis was evaluated in a cohort of 195 patients, 29 of whom had UTUC with subsequent bladder cancer. The median time to recurrence in the study was 7.3 months. FGFR3, KDM6A, and CCND1 were associated with bladder recurrence (HR~3), whereas TP53 had a lower risk (HR=0.32). Notably, all UTUC and bladder cancer cases were clonal with bladder tumors reflecting UTUC genetically.3 UTUC is characterized by a high mutational burden and high microsatellite instability is seen mainly in Lynch Syndrome-associated cancers. There remain putative mechanisms involving DNA Damage Response (DDR) genes.
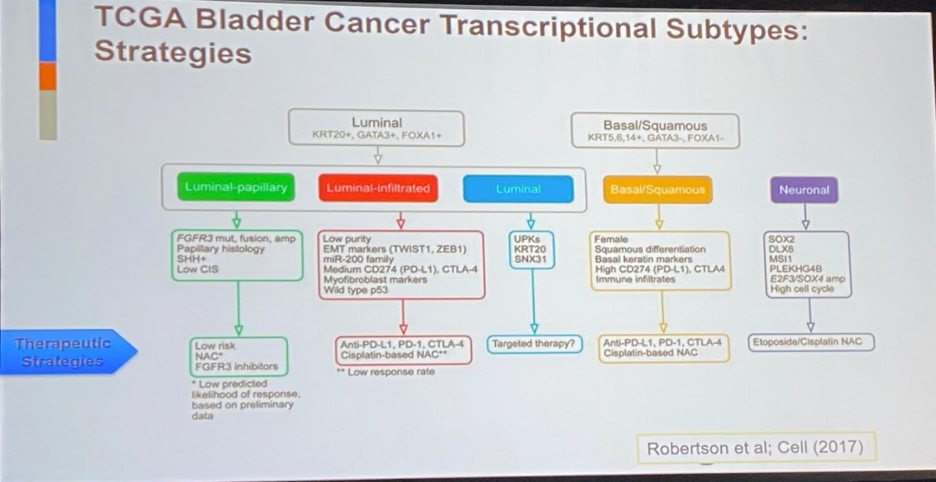
In the MIBC disease space, ERCC2 and DDR mutations have been shown to be favorable prognostic factors for OS in MIBC patients treated with platinum-based chemotherapy regimens. Similarly, the TCGA bladder cancer transcriptional subtypes has been used to guide treatment strategies. The challenge thus becomes to identify similar prognostic markers in the UTUC space.
Robinson et al. performed a multicenter integrated analysis of whole-exome and RNA sequencing of 37 UTUC cases4 and demonstrated that:
- Most UTUCs are luminal-papillary
- UTUC has a T-cell depleted immune contexture
- High FGFR3 expression is enriched in UTUC and correlates with its T-cell depleted immune microenvironment
- Sporadic UTUC is characterized by a lower total mutational burden than bladder cancer
Five anatomic variations in UTUC genetic profiles have been identified, ranked here from most favorable (hypermutated) to least favorable (triple negative) with regards to disease-specific survival.
- Hypermutated (Lynch) 5%
- FGFR3 mutated (35%)
- RAS Mutated (15%)
- TP53/MDM2 mutated (37%)
- Triple Negative (6%)
Further work by Fujii et al. utilized RNA sequencing data from 168 UTUC samples to identify five specific expression subtypes (C1-C5), with moderate to weak correlations with phi coefficients of 0.22-0.56 between expression and mutational subtypes. C1 subtypes had the best prognostic profile, followed by C2 and C3-C5. Dr. Coleman went on to present unpublished data by his team evaluating UTUC microenvironment with immune response gene sets upregulated in clusters.
Dr. Coleman summarized his talk with the following important points:
- UTUC and bladder cancer are genetically similar but have very different distributions of mutations and associated expression patterns associated with clinical outcomes
- FGFR3 as biologic driver and major target
- HRAS and RB1
- Association with stage, grade, and cancer specific survival
- Luminal papillary expression phenotype, T-cell depleted
- Genomic changes as biomarkers - Tools for risk stratification
- Developing strategies: Neoadjuvant chemotherapy, imuunotherapy, lymph node disseciton ,etc.
- Precision medicine approaches
- FGFR3 (40-60%), Checkpoint/Immuno (MSI-H, T-Cell depleted), platinum-based (ERCC2), PIK3CA - Role for combination strategies
- Techniques for sequencing/tumor modeling from patient derived samples are promising for tumor microenvironment studies - providing deeper insight
Presented by: Jonathan Coleman, MD, Associate Professor, Urology, Department of Surgery, Memorial Sloan Kettering Cancer Center, New York, NY
Written by: Rashid Sayyid, MD, MSc – Urology Chief Resident, Augusta University/Medical College of Georgia, @rksayyid on Twitter during the 2021 Society of Urologic Oncology (SUO) Winter Annual Meeting, Orlando, FL, Wed, Dec 1 – Fri, Dec 3, 2021.
References:
- Pietzak EJ, Bagrodia A, Cha EK, et al. Next-generation Sequencing of Nonmuscle Invasive Bladder Cancer Reveals Potential Biomarkers and Rational Therapeutic Targets. Eur Urol. 2017 Dec;72(6):952-959.
- Sfakianos JP, Cha EK, Iyer G, et al. Genomic Characterization of Upper Tract Urothelial Carcinoma. Eur Urol. 2015 Dec;68(6):970-7.
- Audenet F, Isharwal S, Cha EK, et al. Clonal Relatedness and Mutational Differences between Upper Tract and Bladder Urothelial Carcinoma. Clin Cancer Res. 2019 Feb;25(3):967-976.
- Robinson BD, Vlachostergios PJ, Bhinder B, et al. Upper tract urothelial carcinoma has a luminal-papillary T-cell depleted contexture and activated FGFR3 signaling. Nat Commun. 2019 Jul;10(1):2977.