To this end, the Johns Hopkins Greenberg Bladder Cancer Institute and the American Urological Association held a Translational Research Collaboration entitled “Drug Development in NMIBC from Scientific, Regulatory, Clinician, and Patient Perspectives”. The first session of this symposium focused on Drug Development for BCG-naïve NMIBC. In this session, Dr. Robert Svatek presented on novel treatment approaches which may be used alone or in combination with BCG among patients with BCG-naïve NMIBC.
To begin, Dr. Svatek highlighted a number of considerations in the BCG-naïve space including the difficulty of performing superiority trials of novel approaches compared to BCG as the standard of care control arm, given its efficacy; that all recurrences are not equal; questions with choosing the right endpoint; and assessment bias given changing assessment approaches, including enhanced cystoscopy.
In the context of superiority trial design, recent analyses have demonstrated that the standard of care BCG approach with induction followed by maintenance is associated with high response rates and relatively good recurrence-free survival.

This sets a high bar to beat the current standard of care. Further, a subset of patients get a complete response even after just 6-week induction BCG course. As a result, all comparative trials of intravesical chemotherapy have, to date, showed inferior outcomes.

Dr. Svatek then discussed other issues with trial design in this population. First, while recurrence-free survival is a commonly used outcome, he emphasized that not all recurrence are equal, with differences in tumor size and multifocality among other issues. He then suggested that a more nuanced approach and consideration of the limitations of RFS as an endpoint is required.
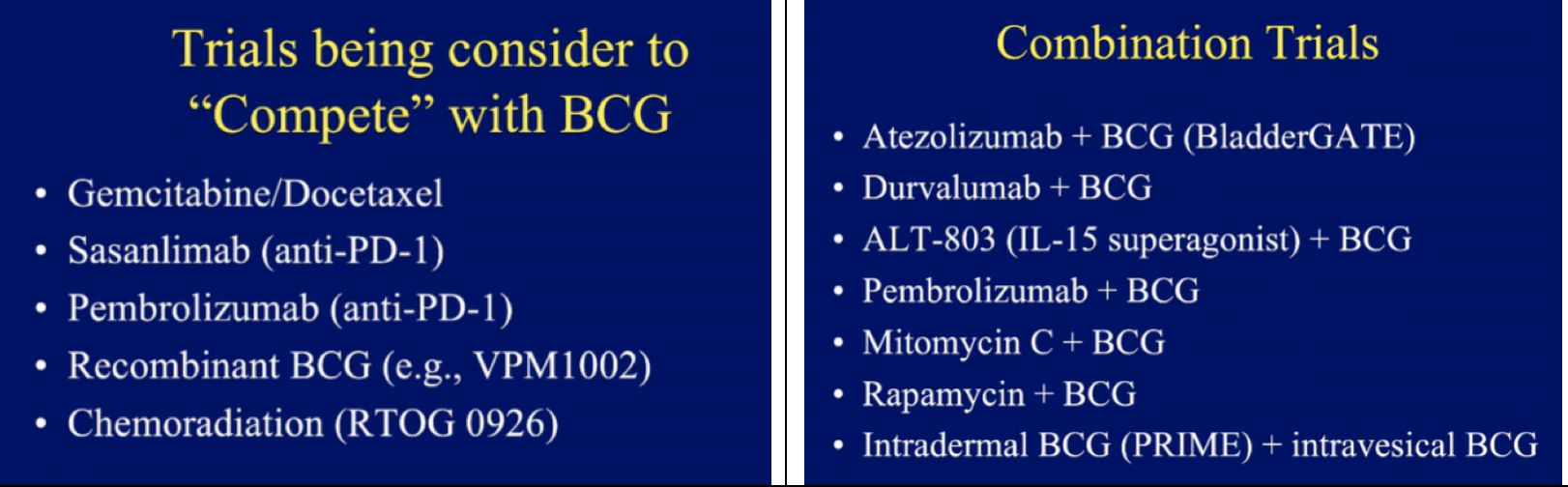
That said, he then highlighted a number of planned or ongoing trials to “compete” with BCG in the BCG-naïve population, most of which have a strong rationale based on lab data. Dr. Svatek expressed particular interest in recombinant BCG approaches. He also discussed a number of combination trials in which novel agents are being added to BCG. Many of these agents have previously been tested or used as monotherapy in more advanced bladder cancer.
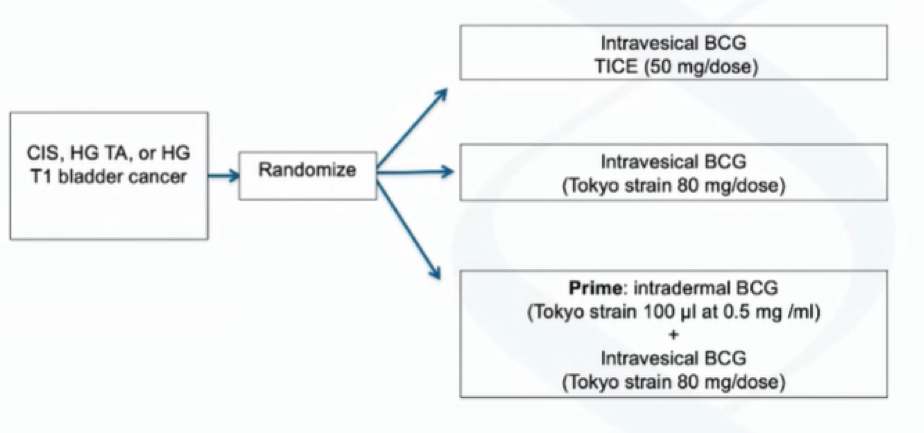
He specifically highlighted the PRIME trial. Also known as SWOG 1612, this study was based on lab data from a mouse model suggesting that intradermal BCG vaccination may improve response to intravesical BCG. This rationale was then tested in a small human trial in which BCG-naïve patients received PPD with percutaneous BCG followed by intravesical treatment. They monitored the bladder cystoscopically as well as urine and blood testing, which demonstrated beneficial effects on BCG-related T cells.
In the PRIME trial, the Tokyo BCG strain is being used for both intradermal inoculation and intravesical instillation in a three-arm design with TICE strain BCG also used as a standard of care comparator. This study was designed to test the superiority between of intravesical Tokyo strain BCG when combined with intradermal inoculation as compared to intravesical alone (arms 2 and 3) as well as testing the non-inferiority of intravesical Toyko strain alone to intravesical TICE strain (arms 1 and 2).
This trial is now accrued and is awaiting readout. However, further work suggests a more targeted approach. Genomic subtyping has identified two distinct subtypes of NMIBC, including subtype 1 (GS1) which relatively few copy number alterations, and subtype 2 (GS2) which a high frequency of chr9 deletions and mTOR pathway loss that may be targetable for mTOR inhibitors. In a murine-model, these mTOR pathway losses are targetable through the use of rapamycin which, in combination with BCG, demonstrates increased efficacy compared with BCG alone, through an effect moderated through gamma delta T cells. This effect was further demonstrated in a humanized mouse model in which human bladder tumors were implanted in immune-deficient mice.
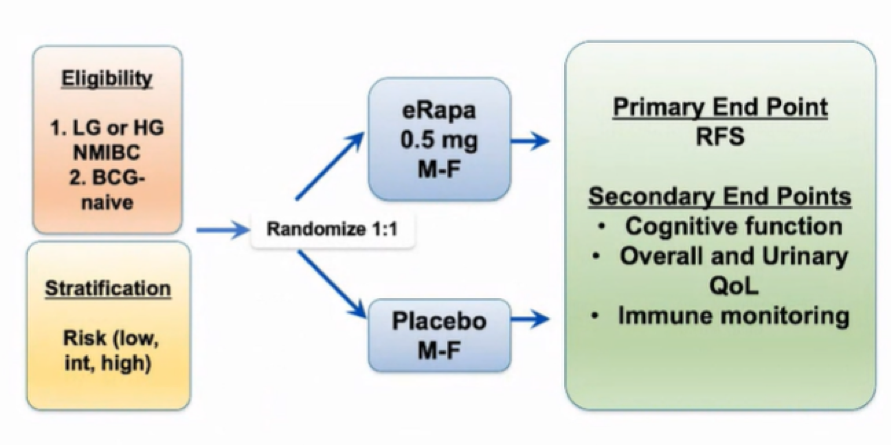
These preclinical data led to a small RCT of rapamycin + BCG vs BCG, designed and powered to assess effects on BCG-specific gamma-delta T cells, as well as safety and tolerability. This study met its primary endpoint, with an effect on gamma-delta Tcells without effect on CD4 or CD8 cells. This work contributed to R01 funded phase II trial that just activated to assess encapsulated rapamycin (eRapa). This study, while powered to assess recurrence-free survival, is taking a stratified approach looking to identify patient populations with the greatest benefit for a planned phase III trial. Based on the aforementioned data, Dr. Svatek emphasized that it is expected that those with GS2 are the most likely to benefit.
Presented by: Robert Svatek, MD, Urologist, UT Health San Antonio, Texas