Five years ago, we were debating intermittent vs. continuous ADT on the heels of the Hussein et al. (NEJM 2013) data, which stated intermittent ADT was non-inferior to continuous ADT. In the mHSPC space, there have since been 3 major trials that have changed the landscape – CHAARTED,1 LATITUDE2 and STAMPEDE.3 At this time, in the setting of metastatic hsPCa, the main treatment options are ADT alone, abiraterone + ADT or docetaxel + ADT.
The first question is: does volume matter. And, the answer is yes, considering that prostate cancer is a disease that is biologically heterogeneous, clinically heterogeneous, and requires individual treatment plans.
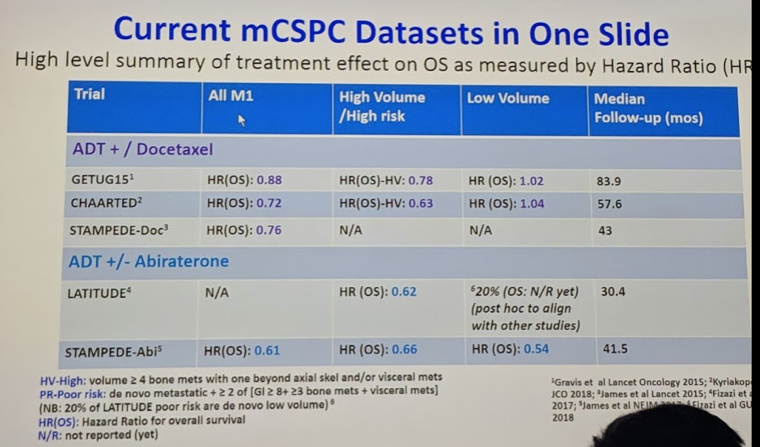
In CHAARTED, patients were stratified based on volume of disease. With longer follow-up, now at 53.7 months, there still remains a 10-month OS benefit in the entire population (HR 0.73). In the high volume patients, there has remained a 17-month OS benefit (HR 0.6), but in the low-volume patients, there is no OS benefit anymore.
In LATITUDE, only high-risk patients (visceral metastases, >= 3 bony mets, and Gleason >= 8 disease) were included. With a mean follow-up of 30 months, there was a 38% improvement in OS (HR 0.62) and 19-month rPFS benefit (HR 0.47).
In STAMPEDE (both the docetaxel arm and abiraterone arm), there was no stratification based on volume of disease. However, in both studies, when stratified for M1 vs. M0 disease, there did not appear to be any benefit in the high-risk M0 patients, suggesting the volume of disease matters. Indeed, at ESMO this year, in a post-hoc analysis of the STAMPEDE abiraterone data, Alex Hoyle retrospectively applied the LATITUDE high-risk and CHAARTED high-volume stratification. Interestingly, they found that abiraterone had similar OS and Prostate-cancer specific survival benefit in both the low and high risk patients.
This slide summarizes all that data:
In a separate analysis, the STAMPEDE authors indirectly compared their docetaxel arm to their abiraterone arm for all the major oncologic outcomes – and found that while abiraterone was favored for failure-free and PFS, it was relatively equivalent for MFS, DSS, and OS. Despite this, it is not “fashionable” to propose the more toxic agent (docetaxel) up front – even though it has similar efficacy, shorter dosing and is cheaper.
He argues that for men with high volume disease who are fit for chemotherapy, docetaxel should be given up front – better to give it when patients are fit, or else that window of opportunity may be lost. While it does have short term toxicity, following its 18-week administration, many of these adverse events resolve – so it may, in fact, have better long-term tolerability. As our goal is to get in as many treatments as possible, probably better to get docetaxel in early in eligible patients.
However, the story continues. Here are a list of ongoing trials that have yet to report – and may confuse the picture even more!
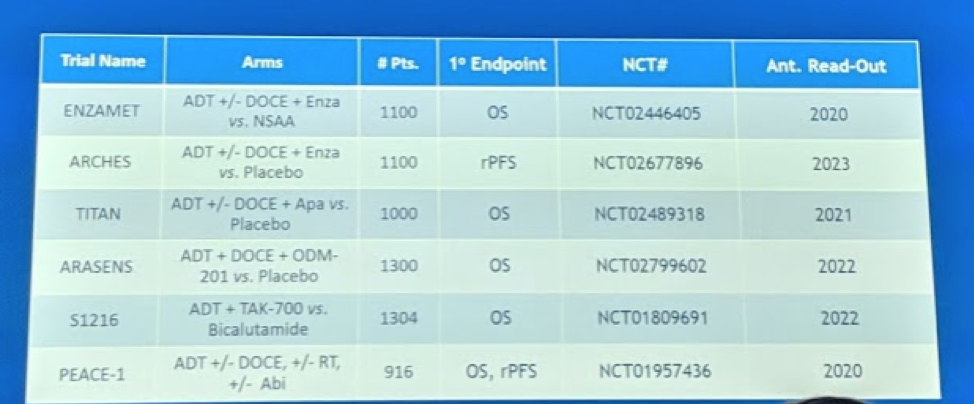
PEACE-1 specifically combines abiraterone and docetaxel.
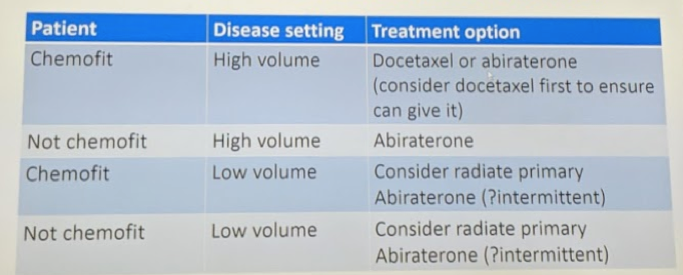
His summary slide for current recommendations:
Presented by: Joaquim Bellmunt, MD, Ph.D., Director of the Bladder Cancer Center at Dana-Farber Cancer Institute and Dana-Farber/Brigham and Women's Cancer Center, Harvard University, Boston, Massachusetts
Written by: Thenappan Chandrasekar, MD. Clinical Instructor, Thomas Jefferson University, Twitter: @tchandra_uromd, @TjuUrology, at the 16th Meeting of the European Section of Oncological Urology, #ESOU19, January 18-20, 2019, Prague, Czech Republic
References:
- Sweeney CJ, Chen YH, Carducci M, et al. Chemohormonal Therapy in Metastatic Hormone-Sensitive Prostate Cancer. N Engl J Med. 2015;373(8):737-746.
- Fizazi K, Tran N, Fein L, et al. Abiraterone plus Prednisone in Metastatic, Castration-Sensitive Prostate Cancer. N Engl J Med. 2017;377(4):352-360.
- James ND, de Bono JS, Spears MR, et al. Abiraterone for Prostate Cancer Not Previously Treated with Hormone Therapy. N Engl J Med. 2017;377(4):338-351.