(UroToday.com) The 2023 European Society of Medical Oncology (ESMO) Annual Congress held in Madrid, Spain between October 20th and 24th, 2023 was host to a presidential session. Dr. Thomas Powles presented the late-breaking abstract results of EV-302/KEYNOTE-A39, an open label, randomized phase III study of enfortumab vedotin plus pembrolizumab versus chemotherapy in patients with previously untreated locally advanced and/or metastatic urothelial carcinoma.
There are approximately 200,000 deaths worldwide annually secondary to advanced urothelial carcinoma. Prognosis remains poor with low 5-year survival rates. Platinum-based chemotherapy has remained the standard of care 1st line therapy for patients with locally advanced/metastatic urothelial carcinoma for decades. While avelumab is approved as maintenance therapy in a subset of patients whose disease has not progressed following 1st line platinum-based chemotherapy, a high unmet need remains. Two previously published trials of chemotherapy in combination with PD-1/PD-L1 inhibitors have failed to improve survival in patients with locally advanced/metastatic urothelial carcinoma. 1,2
Enfortumab vedotin, a Nectin-4 directed antibody-drug conjugate, and pembrolizumab, a PD-1 inhibitor, have individually demonstrated a survival benefit in previously treated locally advanced/metastatic urothelial carcinoma. The combination of these two drugs was granted accelerated approval by the FDA for the treatment of such patients who are ineligible for cisplatin therapy. The objective of EV-302/KEYNOTE-A39 (NCT04223856) was to compare the combination of enfortumab vedotin + pembrolizumab (EV + P) versus platinum-based chemotherapy in previously untreated patients with locally advanced/metastatic urothelial carcinoma, regardless of cisplatin eligibility and PD-L1 expression status.
Patients in this trial were randomized in a 1:1 fashion, stratified by cisplatin eligibility, PD-L1 expression, and presence/absence of liver metastases, to EV + P (continued until disease progression per BICR, clinical progression, unacceptable toxicity, or completion of maximum cycles [35 for pembrolizumab]) versus gemcitabine + cisplatin or carboplatin for a maximum of 6 cycles. The dual primary endpoints were PFS by BICR and OS. OS analysis was planned at two interim analyses, including a later analysis, but as OS reached statistical significance in this primary analysis, this was considered the final analysis for OS in this trial.
The two arms were well-balanced for key demographic and baseline disease characteristics. The median age was 69 years. The vast majority (97%) had ECOG performance status of 0 – 1. The primary tumor location was the lower tract in approximately 75% of patients. 54% of patients were determined to be cisplatin eligible. 22% of patients had evidence of liver metastases. High PD-L1 expression was present in 58% of patients.

Dr. Powles noted that 22% of patients in the EV + P arm discontinued treatment due to an adverse event, compared to 14% of those in the chemotherapy arm.
PFS per BICR was significantly improved in the EV + P arm from a median of 6.3 months to 12.5 months (HR: 0.45, 95% CI: 0.38 – 0.45, p<0.001).
Subgroup analysis of PFS per BICR demonstrated consistent, clinically meaningful benefits across all evaluable subgroups.
OS was nearly double in the EV + P arm, with median survivals of 31.5 and 16.1 months in the EV +P and chemotherapy arms, respectively (HR: 0.47, 95% CI: 0.38 – 0.58, p<0.00001).
Subgroup analyses by cisplatin eligibility demonstrated that the OS benefit was consistent in both subgroups.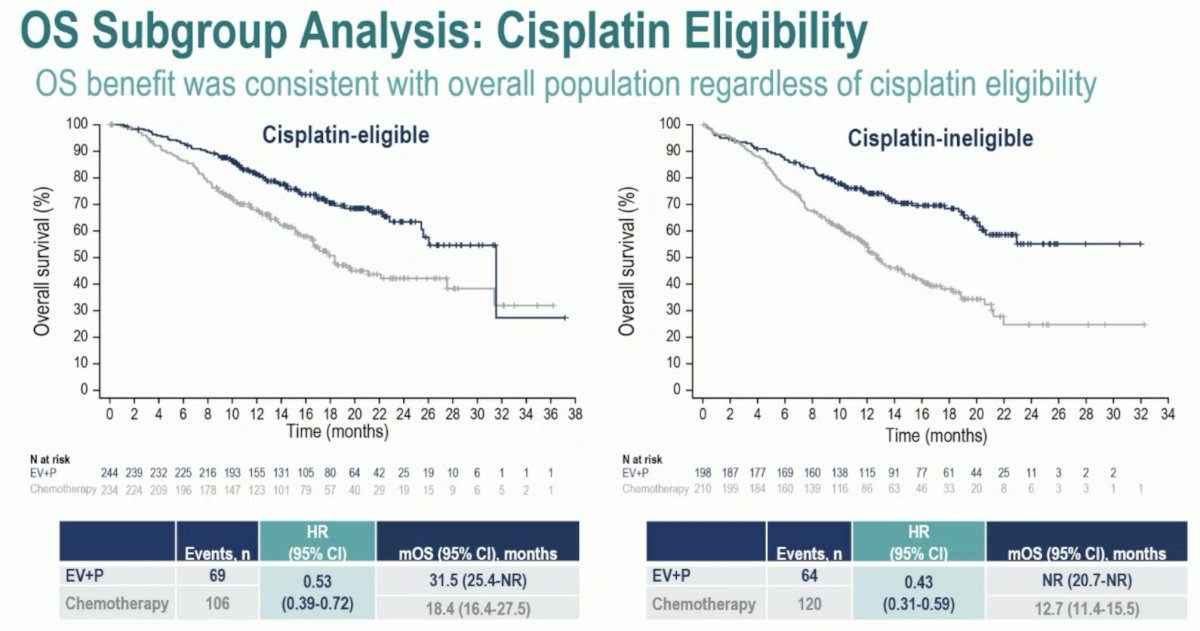
Similarly, a significant OS benefit was seen in both PD-L1 high and low expression subgroups:
Subgroup analyses by age, sex, ECOG performance status, primary disease site of origin, and presence/absence of liver metastases demonstrated consistent OS benefits in favor of EV + P.
The ORR was higher with EV +P (68% versus 44%), with the complete response rate notably higher with EV + P (29.1% versus 12.5%).
As expected, a higher proportion of patients in the chemotherapy arm received a subsequent systemic therapy (66.2% versus 28.9%), most commonly in the form of PD-1/L1 inhibitor therapy for those in the chemotherapy arm (58.6%) and platinum-based therapy (24.9%) in the EV + P arm.
Treatment-related adverse events (TRAEs) were consistent with the known safety profiles of each of the drugs. Serious TRAEs occurred in 27.7% of patients in the EV + P arm, compared to 19.6% with chemotherapy. TRAE leading to death occurred in 4 patients (0.9%) in each arm. Overall, grade 3+ adverse events occurred in 56% and 70% of patients in the EV + P and chemotherapy arms, respectively.
The most common EV TRAEs were skin reactions, peripheral neuropathy, ocular disorders, and hyperglycemia.
Dr. Powles concluded his presentation with the following take home messages:
- EV-302/KEYNOTE-A39 is the first time that platinum-based chemotherapy has been surpassed in overall survival in patients with previously untreated locally advanced/metastatic urothelial carcinoma
- Enfortumab vedotin + pembrolizumab show statistically significant and clinically meaningful improvements in efficacy over chemotherapy
- PFS: HR=0.45; OS: HR=0.47
- Median PFS and OS were nearly doubled in the EV + P arm compared with chemotherapy
- The benefits in pre-specified subgroups and stratification factors were consistent with those observed in the overall population
- The safety profile of EV + P was generally manageable, with no new safety signals observed
- These results support EV + P as a potential new standard of care for 1st line locally advanced/metastatic urothelial carcinoma
Presented by: Thomas Powles, MD, MBBS, MRCP, Professor of Genitourinary Oncology, Director, Barts Cancer Centre at St. Bartholomew's Hospital, London, UK
Written by: Rashid K. Sayyid, MD, MSc – Society of Urologic Oncology (SUO) Clinical Fellow at The University of Toronto, @rksayyid on Twitter during the 2023 European Society of Medical Oncology (ESMO) Annual Congress held in Madrid, Spain between October 20th and 24th, 2023
References:- Powles T, Csoszi T, Ozguroglu M, et al. Pembrolizumab alone or combined with chemotherapy versus chemotherapy as first-line therapy for advanced urothelial carcinoma (KEYNOTE-361): a randomised, open-label, phase 3 trial. Lancet Oncol. 2021;22(7):931-945.
- Galsky MD, Arija JAA, Bamias A, et al. Atezolizumab with or without chemotherapy in metastatic urothelial cancer (IMvigor130): a multicentre, randomised, placebo-controlled phase 3 trial. Lancet. 2020;395(10236):1547-1557.